You might also like
- Statin Drugs-What Your Doctor Should Have Told YouDocument3 pagesStatin Drugs-What Your Doctor Should Have Told YouDr. Michael Ackerman100% (1)
- Iron Man - USA 3 2007Document179 pagesIron Man - USA 3 2007api-39180899100% (3)
- Hh2sgonzupzxf4gu1w1wym1fDocument1 pageHh2sgonzupzxf4gu1w1wym1fHarsh AryaNo ratings yet
- The Natural Diabetes Cure: Curing Blood Sugar Disorders Without DrugsDocument88 pagesThe Natural Diabetes Cure: Curing Blood Sugar Disorders Without DrugsangelobuffaloNo ratings yet
- LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Document3 pagesLPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Puneet jain.aca100% (1)
- MAX Health CheckupDocument10 pagesMAX Health Checkuppriyanka.singh1996.pssNo ratings yet
- 1-Dengue Antigen NS1, IgG & IgM - PO1576121305-961 PDFDocument16 pages1-Dengue Antigen NS1, IgG & IgM - PO1576121305-961 PDFArijit GoraiNo ratings yet
- A10 - Rohtak Lab Home Visit 1267, Chotu Ram Chowk, Opp Nilli Kothi, Civil Road RohtakDocument2 pagesA10 - Rohtak Lab Home Visit 1267, Chotu Ram Chowk, Opp Nilli Kothi, Civil Road RohtakjyotiNo ratings yet
- XIJU5502Document3 pagesXIJU5502Praveen ReddyNo ratings yet
- Unlq6073 PDFDocument8 pagesUnlq6073 PDFSrinu VijayaNo ratings yet
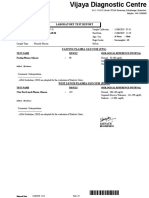
- Vijaya DiagnosticDocument5 pagesVijaya Diagnosticuma reddyNo ratings yet
- Laboratory Test Report: Mr. D Venkata Narayna 39 Years MaleDocument2 pagesLaboratory Test Report: Mr. D Venkata Narayna 39 Years Malepavan kumarNo ratings yet
- Report F412b1a3Document18 pagesReport F412b1a3055Nitish BhatiaNo ratings yet
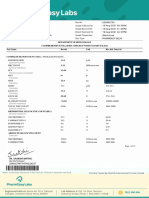
- Department of Clinical Biochemistry: Fasting Blood Sugar 96 MG/DLDocument2 pagesDepartment of Clinical Biochemistry: Fasting Blood Sugar 96 MG/DLAnand M SNo ratings yet
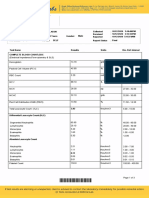
- Haematology Test Name Results Biological Reference Interval Units Specimen Test Method CBC - Complete Blood CountDocument2 pagesHaematology Test Name Results Biological Reference Interval Units Specimen Test Method CBC - Complete Blood CountlijoNo ratings yet
- Module Five Wellness Plan HOPEDocument15 pagesModule Five Wellness Plan HOPEZelda Raniblanket100% (1)
- LFT RFT LP RBS EsrDocument1 pageLFT RFT LP RBS EsrDeepak SharmaNo ratings yet
- S10 - Lpl-Ludhiana 12-C, SARABHA NAGAR, LUDHIANA-141001, Pu Njab LudhianaDocument4 pagesS10 - Lpl-Ludhiana 12-C, SARABHA NAGAR, LUDHIANA-141001, Pu Njab LudhianaInderpreet SinghNo ratings yet
- The Egyptian Heart Journal: Haitham Galal Mohammed, Adel Mohamed ShabanaDocument6 pagesThe Egyptian Heart Journal: Haitham Galal Mohammed, Adel Mohamed ShabanaDaniel Zagoto100% (1)
- Report 831a66a7 PDFDocument23 pagesReport 831a66a7 PDFViral PatelNo ratings yet
- S28 - Lpl-Hyderbad Shop No - G-29,30 & 12 Swarna Jayanthi Complex, Ameerpet Hyderabad 38Document4 pagesS28 - Lpl-Hyderbad Shop No - G-29,30 & 12 Swarna Jayanthi Complex, Ameerpet Hyderabad 38Thaneswar beheraNo ratings yet
- HeaderDocument11 pagesHeaderSrinivas MalladiNo ratings yet
- Papa Reports 04-07-2022Document6 pagesPapa Reports 04-07-2022Anish goyalNo ratings yet
- KESHAV KASHYAP Lipid ProfileDocument3 pagesKESHAV KASHYAP Lipid ProfiletestNo ratings yet
- Diagnostic Report: FinalDocument5 pagesDiagnostic Report: FinalMiniNo ratings yet
- Haematology Test Name Result Unit Bio. Ref. Range MethodDocument28 pagesHaematology Test Name Result Unit Bio. Ref. Range MethodVijaya SheelamNo ratings yet
- 1-Senior Citizen Advanced Package - PO3427386675-856Document18 pages1-Senior Citizen Advanced Package - PO3427386675-856Ravi PrakashNo ratings yet
- Pankaj Das - Aarogyam 1.2 + FBSDocument10 pagesPankaj Das - Aarogyam 1.2 + FBSplasmadragNo ratings yet
- Cardiac Rehab BookletDocument32 pagesCardiac Rehab BookletAbu Bakr Siddique100% (1)
- Laboratory Test Report: Mrs. V Valli Kumari 81 Years FemaleDocument2 pagesLaboratory Test Report: Mrs. V Valli Kumari 81 Years FemaleumaNo ratings yet
- 1-Basic Health Screening (Includes 29 Tests) - PO2403760062-868Document5 pages1-Basic Health Screening (Includes 29 Tests) - PO2403760062-868SMILLING CLOUDNo ratings yet
- SpectrophotometerDocument13 pagesSpectrophotometerRanjana NailwalNo ratings yet
- S65 - PSC Haldwani Diagnostic Centre - Home Visit Sahukara Line, Opp. SS Jeena Base Hospital Nainital, HaldwaniDocument3 pagesS65 - PSC Haldwani Diagnostic Centre - Home Visit Sahukara Line, Opp. SS Jeena Base Hospital Nainital, Haldwanirajasereddy1275No ratings yet
- Department of Hematology Covid-19 Health Checkup (Post Recovery)Document8 pagesDepartment of Hematology Covid-19 Health Checkup (Post Recovery)Geetika GuptaNo ratings yet
- Khaleel Ur Rahman: Haematology Fever PackageDocument5 pagesKhaleel Ur Rahman: Haematology Fever Packageaashi77No ratings yet
- LabTest 01jan2023Document1 pageLabTest 01jan2023Mohammad YameenNo ratings yet
- Self Amalendu Bikash Nath (66Y/M) 3B Amardham Apartment South Station Road Agarpara Near Aqua Diamond Water FactoryDocument19 pagesSelf Amalendu Bikash Nath (66Y/M) 3B Amardham Apartment South Station Road Agarpara Near Aqua Diamond Water FactoryOritra BanerjeeNo ratings yet
- D-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: Name Ref. by Test Asked::: Patientid: Home CollectionDocument4 pagesD-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: Name Ref. by Test Asked::: Patientid: Home Collectionfaiyaz432No ratings yet
- Heart Disease Case StudyDocument13 pagesHeart Disease Case Studyapi-284823421100% (1)
- Lipids MetabolismDocument11 pagesLipids MetabolismfakhribabikerNo ratings yet
- Opdbills 4950545655505348Document1 pageOpdbills 4950545655505348Koshindar GaurNo ratings yet
- CBC-Report RDocument1 pageCBC-Report Ryoutube premiumNo ratings yet
- Mrs Anar DeviDocument14 pagesMrs Anar DeviM.DNo ratings yet
- WRUV7926Document3 pagesWRUV7926rajashekarcse533No ratings yet
- Himani Singhal 56024602023 04 19 10 55 14 598 1 6 452 133264571589922492 PDFDocument16 pagesHimani Singhal 56024602023 04 19 10 55 14 598 1 6 452 133264571589922492 PDFONE SURE LABNo ratings yet
- S53 - Syed Kashif Ghani-Fpsc Zakir Nagar: Patientreportscsuperpanel - General - Panel - Analyte - SC (Version: 6)Document11 pagesS53 - Syed Kashif Ghani-Fpsc Zakir Nagar: Patientreportscsuperpanel - General - Panel - Analyte - SC (Version: 6)Khalid Mohammad Khalid TanwiriNo ratings yet
- S60 - Fofo Greater Noida Shop No.-5, LGF, Amrapali Leisure Valley Greater Noida West (U.P)Document2 pagesS60 - Fofo Greater Noida Shop No.-5, LGF, Amrapali Leisure Valley Greater Noida West (U.P)Deepanshu Singh KushwahaNo ratings yet
- ReportDocument5 pagesReportSandip WankhedeNo ratings yet
- (Merge) Hepatitis C Virus HCV Test Report Format Example Sample Temp 20240101 141Document5 pages(Merge) Hepatitis C Virus HCV Test Report Format Example Sample Temp 20240101 141M ShafiqNo ratings yet
- SVLT Lab Report DetailsDocument2 pagesSVLT Lab Report DetailsKirtivaan MishraNo ratings yet
- Sars-Cov-2 by RT PCR (Qualitative) : Icmr Reg .No. - SanpalagDocument1 pageSars-Cov-2 by RT PCR (Qualitative) : Icmr Reg .No. - SanpalagHaimanti NathNo ratings yet
- Typhoid Test ReportDocument4 pagesTyphoid Test ReportDEEPAK DubeyNo ratings yet
- S P VashistDocument27 pagesS P VashistGhissu GangNo ratings yet
- Date 23/apr/2023 12:20PM Unit Bio Ref Interval: Kindly Correlate With Clinical FindingsDocument14 pagesDate 23/apr/2023 12:20PM Unit Bio Ref Interval: Kindly Correlate With Clinical FindingsashiNo ratings yet
- SRL Diagnostics App On Your Mobile Device by Using QR Code. CALL Our Customer Care On 91115 91115Document1 pageSRL Diagnostics App On Your Mobile Device by Using QR Code. CALL Our Customer Care On 91115 91115Akhil ChawlaNo ratings yet
- Test Description Value(s) Unit(s) Reference Range: Pt/InrDocument2 pagesTest Description Value(s) Unit(s) Reference Range: Pt/InrSuhas KapseNo ratings yet
- Department of Clinical Biochemistry: Hba1C With EagDocument1 pageDepartment of Clinical Biochemistry: Hba1C With EagMR: B H A V A N T HNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval Total T3Document3 pagesLaboratory Test Report: Test Name Result Biological Reference Interval Total T3Chandu Chan LyristNo ratings yet
- Blood Report PDFDocument3 pagesBlood Report PDFDebabrata DasNo ratings yet
- Date 28/mar/2023 10:09AM Unit Bio Ref Interval: Laboratory Investigation ReportDocument12 pagesDate 28/mar/2023 10:09AM Unit Bio Ref Interval: Laboratory Investigation ReportChauhanNo ratings yet
- Specimen: Nasopharyngeal Swab: Dr. Girish Gaur Lab Director and Senior Consultant Molecular DiagnosticsDocument1 pageSpecimen: Nasopharyngeal Swab: Dr. Girish Gaur Lab Director and Senior Consultant Molecular DiagnosticsBhavy BansalNo ratings yet
- FrmPatientViewAllReport - 2023-04-06T211159.013 PDFDocument9 pagesFrmPatientViewAllReport - 2023-04-06T211159.013 PDFamir.khann4411No ratings yet
- Haematology Complete Blood Count (CBC EXT) : 021808250310 MR - AJAY KUMAR 662326Document7 pagesHaematology Complete Blood Count (CBC EXT) : 021808250310 MR - AJAY KUMAR 662326ANSHU KUMAR RANANo ratings yet
- GANESANDocument8 pagesGANESANBuvanesh BalajiNo ratings yet
- Laboratory Test Report: Test Name Result Sars-Cov-2 (RDRP Gene)Document5 pagesLaboratory Test Report: Test Name Result Sars-Cov-2 (RDRP Gene)Imran AhmedNo ratings yet
- Self Anil Yadav (30Y/M) Mfine Basic Full Body Check 23A Shakti Vihar Gali No 1 Meetha Pur Delhi DelhiDocument7 pagesSelf Anil Yadav (30Y/M) Mfine Basic Full Body Check 23A Shakti Vihar Gali No 1 Meetha Pur Delhi DelhiRavish TrivediNo ratings yet
- Tahenyat Karimkhan. 2-35-37 PMDocument1 pageTahenyat Karimkhan. 2-35-37 PMchildicuNo ratings yet
- Laboratory Test Report: Sars-Cov-2Document1 pageLaboratory Test Report: Sars-Cov-2sandeep yadav0% (2)
- Circresaha 119 312617Document14 pagesCircresaha 119 312617Andrianna NastasyaNo ratings yet
- Tuvalu Standard Treatment GuidelinesDocument401 pagesTuvalu Standard Treatment GuidelinesportosinNo ratings yet
- Sas Ron CodyDocument35 pagesSas Ron Cody王No ratings yet
- Fenugreek An OverviewDocument19 pagesFenugreek An OverviewArun EbenezerNo ratings yet
- A29 - Neva Diagnostic Centre Dumurtala Kaliaganj Murhsidabad 742305 West Bengal JalangiDocument5 pagesA29 - Neva Diagnostic Centre Dumurtala Kaliaganj Murhsidabad 742305 West Bengal Jalanginafiul islamNo ratings yet
- Blood Test Normal ValuesDocument11 pagesBlood Test Normal Valueschristophe1967No ratings yet
- TIens ProductsDocument12 pagesTIens ProductsGhulam AbbasNo ratings yet
- Sas 11Document8 pagesSas 11Reizel GaasNo ratings yet
- What Are FatsDocument20 pagesWhat Are FatsbobNo ratings yet
- Kroll V10 SP21 Feature NotesDocument20 pagesKroll V10 SP21 Feature Notesmorteza piraliNo ratings yet
- Tenp DPT Biochemistry: DR Pius KiptemburDocument13 pagesTenp DPT Biochemistry: DR Pius KiptemburGerald Limo Arap ChebiiNo ratings yet
- Healthy Living Event Proposal 2013 Group 3Document7 pagesHealthy Living Event Proposal 2013 Group 3api-235001675No ratings yet
- Csat (Paper-Ii) Full Length Test - 4: Time Allowed: 2 Hours Maximum Marks: 200Document35 pagesCsat (Paper-Ii) Full Length Test - 4: Time Allowed: 2 Hours Maximum Marks: 200sx46bNo ratings yet
- Chapter 47 - Lipid-Lowering AgentsDocument13 pagesChapter 47 - Lipid-Lowering AgentsJonathonNo ratings yet
- European Heart JournalDocument50 pagesEuropean Heart JournalAgustin CNo ratings yet
- Bios Life CDocument8 pagesBios Life CJakob HechenbergerNo ratings yet
- 2 - AtherosclerosisDocument16 pages2 - AtherosclerosisUnnati PatelNo ratings yet
- Innovating Baked PapayaDocument11 pagesInnovating Baked PapayaJefer GatchalianNo ratings yet
- New Thesis With Corrections Grad School CorrectionsDocument62 pagesNew Thesis With Corrections Grad School Correctionsapi-535934790No ratings yet
- Health and FitnessDocument210 pagesHealth and FitnessEric MensahNo ratings yet
- Hippophae Rhamnoides Seguridad y NutriciónDocument9 pagesHippophae Rhamnoides Seguridad y NutriciónGrisel CCNo ratings yet
- Literature Review On Lipid ProfileDocument7 pagesLiterature Review On Lipid Profileea7gjrm5100% (1)