You might also like
- Chemical Handling ProcedureDocument15 pagesChemical Handling ProcedureGHULAM MOHYUDDINNo ratings yet
- Stem Cells in OrthodonticsDocument4 pagesStem Cells in OrthodonticsInternational Journal of Innovative Science and Research Technology100% (1)
- Alzheimer's Disease: A Guide to Symptoms, Causes, Stages and TreatmentsDocument16 pagesAlzheimer's Disease: A Guide to Symptoms, Causes, Stages and TreatmentsKathleen DiangoNo ratings yet
- Bronquiolite Guidelines AAPDocument32 pagesBronquiolite Guidelines AAPDiego Guedes da SilvaNo ratings yet
- Discharge PlanDocument4 pagesDischarge Plandeo_gratias14No ratings yet
- Introducing The Wireframe DNA Appliance Singh Lipka JAAGO 2009 ArticleDocument4 pagesIntroducing The Wireframe DNA Appliance Singh Lipka JAAGO 2009 ArticleAnders CroccoNo ratings yet
- Chemtrails EffectsDocument1 pageChemtrails EffectsGary CloseNo ratings yet
- Mariyam Zehra PG 1St Year Department of OrthodonticsDocument101 pagesMariyam Zehra PG 1St Year Department of OrthodonticsMariyam67% (3)
- Neurofeedback ResearchDocument50 pagesNeurofeedback Researchdocs1234567No ratings yet
- NLE 2015 Questions SampleDocument8 pagesNLE 2015 Questions SampleJona Suarez100% (4)
- The Osteoporotic Syndrome: Detection, Prevention, and TreatmentFrom EverandThe Osteoporotic Syndrome: Detection, Prevention, and TreatmentNo ratings yet
- Impacts of Orthodontic Treatment On PeriDocument10 pagesImpacts of Orthodontic Treatment On PeriCatia Sofia A PNo ratings yet
- BifosfonatosyortodonciaDocument8 pagesBifosfonatosyortodonciavivigaitanNo ratings yet
- Chambrone2016 ONM2Document5 pagesChambrone2016 ONM2drjaviervaldezNo ratings yet
- Tooth Socket HealingDocument16 pagesTooth Socket HealingluisNo ratings yet
- 10 7126-Cumudj 932462-1750007Document8 pages10 7126-Cumudj 932462-1750007desy natalia anggorowatiNo ratings yet
- Estimulacion Electrica en RatasDocument10 pagesEstimulacion Electrica en RatasdaniamrqNo ratings yet
- Laporan Jurnal ReadingDocument35 pagesLaporan Jurnal ReadingfadiahannisaNo ratings yet
- Paget's disease presenting with root resorptionDocument4 pagesPaget's disease presenting with root resorptionNurani AtikasariNo ratings yet
- Root Resorption Abuabara 2007Document4 pagesRoot Resorption Abuabara 2007Aly OsmanNo ratings yet
- BifosfonatosDocument6 pagesBifosfonatosAna Paulina Marquez LizarragaNo ratings yet
- Iglesias-Linares Et Al. (2010)Document9 pagesIglesias-Linares Et Al. (2010)Laís C. PoletoNo ratings yet
- Idiopathic Impaired Tooth Eruption - An Orthodontic PerspectiveDocument5 pagesIdiopathic Impaired Tooth Eruption - An Orthodontic PerspectiveIJAR JOURNALNo ratings yet
- Pi Is 0889540699702908Document9 pagesPi Is 0889540699702908djosephjohn89No ratings yet
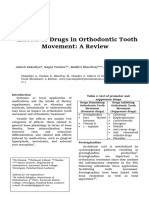
- Effects of Drugs in Orthodontic Tooth Movement: A ReviewDocument6 pagesEffects of Drugs in Orthodontic Tooth Movement: A ReviewvprakshaindiaNo ratings yet
- Factores de Inhibicion de ProsteogerinaDocument11 pagesFactores de Inhibicion de ProsteogerinaWilliam Alexander Bocanegra AcostaNo ratings yet
- Content ServerDocument9 pagesContent ServerNicoll SQNo ratings yet
- Sonnykalangi,+40 +ok+ (6) +Nidia+Limarga+550-555+doiDocument6 pagesSonnykalangi,+40 +ok+ (6) +Nidia+Limarga+550-555+doialif kausarNo ratings yet
- Dioguardi, 2023Document20 pagesDioguardi, 2023Aneliza de Fatima Moraes da SilvaNo ratings yet
- Orthodontic Tooth Movement After Inhibition of Cyclooxygenase-2Document5 pagesOrthodontic Tooth Movement After Inhibition of Cyclooxygenase-2Laís C. PoletoNo ratings yet
- Matrix Metalloproteinase 8 Is The Major Potential C - 2012 - Journal of ProsthodDocument7 pagesMatrix Metalloproteinase 8 Is The Major Potential C - 2012 - Journal of Prosthodradwam123No ratings yet
- Minamoto 2020Document10 pagesMinamoto 2020parakhrishabh8No ratings yet
- BRONJinDentalImplantPatientsGossAustralia PDFDocument7 pagesBRONJinDentalImplantPatientsGossAustralia PDFJing XueNo ratings yet
- Thirunavukarasu 2015Document4 pagesThirunavukarasu 2015James Alexander Toruño GordonNo ratings yet
- Is Dental Implant Placement Compatible in Patients Treated With BiphosphonatesDocument5 pagesIs Dental Implant Placement Compatible in Patients Treated With BiphosphonatesosiglesiNo ratings yet
- Biology of The Alveolar Bone - Orthodontic Tissue Regeneration (OTR) PDFDocument5 pagesBiology of The Alveolar Bone - Orthodontic Tissue Regeneration (OTR) PDFDonald FlorezNo ratings yet
- OutDocument14 pagesOutlorena8804No ratings yet
- Classification of Tooth Mobility Concept RevisitedDocument3 pagesClassification of Tooth Mobility Concept RevisitedAristya SidhartaNo ratings yet
- 732-Article Text-1301-1-10-20230406Document6 pages732-Article Text-1301-1-10-20230406Meiky eka SaputraNo ratings yet
- Effects of Drugs and Systemic Factors on Orthodontic TreatmentDocument7 pagesEffects of Drugs and Systemic Factors on Orthodontic TreatmentOrtodoncia 1No ratings yet
- Dental Complications and Management of Patients On Bisphosphonate Therapy A Review ArticleDocument6 pagesDental Complications and Management of Patients On Bisphosphonate Therapy A Review ArticleyomiboyNo ratings yet
- The Potential Use of Pharmacological Agents To Modulate Orthodontic Tooth Movement (OTM)Document9 pagesThe Potential Use of Pharmacological Agents To Modulate Orthodontic Tooth Movement (OTM)vprakshaindiaNo ratings yet
- Extreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical ManagementDocument8 pagesExtreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical Managementcarmen espinozaNo ratings yet
- Assessment of The Effectiveness of Alendronic Acid in Dental ImplantsDocument3 pagesAssessment of The Effectiveness of Alendronic Acid in Dental ImplantsCentral Asian StudiesNo ratings yet
- Understanding Bisphosphonates and Osteonecrosis of The JawDocument9 pagesUnderstanding Bisphosphonates and Osteonecrosis of The JawGabriela OlateNo ratings yet
- SJ BDJ 2013 1191Document5 pagesSJ BDJ 2013 1191Aditya Rama DevaraNo ratings yet
- Role of Trauma From Occlusion in Periodontal Disease-A ControversyDocument6 pagesRole of Trauma From Occlusion in Periodontal Disease-A Controversywendyjemmy8gmailcomNo ratings yet
- Gingival Bone Resorption in Rat Models of Periodontitis and Orthodontic Tooth MovementDocument7 pagesGingival Bone Resorption in Rat Models of Periodontitis and Orthodontic Tooth MovementLouis HutahaeanNo ratings yet
- Ferreira 2018Document10 pagesFerreira 2018NORMA EDITH JIMENEZ LUNANo ratings yet
- Asds 02 0215Document3 pagesAsds 02 02156mf9jf6h99No ratings yet
- Role of Trauma From Occlusion in Periodontal Disease-A ControversyDocument5 pagesRole of Trauma From Occlusion in Periodontal Disease-A ControversyrmeyyNo ratings yet
- Variables Affecting Orthodontic Tooth Movement With Clear AlignersDocument10 pagesVariables Affecting Orthodontic Tooth Movement With Clear AlignersGoutamNo ratings yet
- Management of Internal Root Resorption A ReviewDocument8 pagesManagement of Internal Root Resorption A ReviewDana StanciuNo ratings yet
- Endodontic Orthodontic Relationships A Review of Integrated Treatment PlanningDocument18 pagesEndodontic Orthodontic Relationships A Review of Integrated Treatment PlanningAlfonso SernaNo ratings yet
- Articol RJMEDocument4 pagesArticol RJMELaura IosifNo ratings yet
- The Influence of Orthodontic Movement On Periodontal Tissues LevelDocument12 pagesThe Influence of Orthodontic Movement On Periodontal Tissues LevelMardiniuc Andra-LuciaNo ratings yet
- Osteoporosis OrthodonticsDocument5 pagesOsteoporosis OrthodonticsIslam GhorabNo ratings yet
- Medication Related Osteonecrosis of The JawDocument26 pagesMedication Related Osteonecrosis of The Jawapi-265532519100% (1)
- Stem Cell Based Tooth Regeneration - An Alternative Approach To Implant DentistryDocument6 pagesStem Cell Based Tooth Regeneration - An Alternative Approach To Implant DentistryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Biomedicine & Pharmacotherapy: Zhou-Shan Tao, Wan-Shu Zhou, Hong-Guang Xu, Min YangDocument11 pagesBiomedicine & Pharmacotherapy: Zhou-Shan Tao, Wan-Shu Zhou, Hong-Guang Xu, Min YangrosanaNo ratings yet
- The Dental Implication of Bisphosphonates RJNDocument10 pagesThe Dental Implication of Bisphosphonates RJNmaxfaxNo ratings yet
- Physical Properties of Root Cementum: Part 26. Effects of Micro-Osteoperforations On Orthodontic Root Resorption: A Microcomputed Tomography StudyDocument10 pagesPhysical Properties of Root Cementum: Part 26. Effects of Micro-Osteoperforations On Orthodontic Root Resorption: A Microcomputed Tomography StudyMonojit DuttaNo ratings yet
- 1042 FullDocument9 pages1042 Fulloki harisandiNo ratings yet
- Seminars in Orthodontics Volume 13 Issue 4 2007 (Doi 10.1053 - J.sodo.2007.08.008) Masaru Yamaguchi Kazutaka Kasai - The Effects of Orthodontic Mechanics On The Dental PulpDocument9 pagesSeminars in Orthodontics Volume 13 Issue 4 2007 (Doi 10.1053 - J.sodo.2007.08.008) Masaru Yamaguchi Kazutaka Kasai - The Effects of Orthodontic Mechanics On The Dental PulpMr-Ton DrgNo ratings yet
- The Use of Bisphosphonates in Children. Review of The Literature and Guidelines For Dental ManagementDocument11 pagesThe Use of Bisphosphonates in Children. Review of The Literature and Guidelines For Dental ManagementHemil Dario Rosales MolinaNo ratings yet
- Retrospective Study: Lateral Ridge Augmentation Using Autogenous Dentin: Tooth-Shell Technique vs. Bone-Shell TechniqueDocument12 pagesRetrospective Study: Lateral Ridge Augmentation Using Autogenous Dentin: Tooth-Shell Technique vs. Bone-Shell TechniqueNarissaporn ChaiprakitNo ratings yet
- Oral Osteonecrosis Induced by Drugs in A Multiple Myeloma PatientDocument4 pagesOral Osteonecrosis Induced by Drugs in A Multiple Myeloma Patientbraily_cardenasNo ratings yet
- Research in Tooth Movement BiologyDocument9 pagesResearch in Tooth Movement BiologyJUAN FONSECANo ratings yet
- Dose-Dependent Effects of ZoledronicDocument12 pagesDose-Dependent Effects of ZoledronicAndreea GorbanescuNo ratings yet
- 3.bisphosphonates in DentistryDocument10 pages3.bisphosphonates in DentistryAndreea GorbanescuNo ratings yet
- Articol 2 Engleză EPIDocument4 pagesArticol 2 Engleză EPIAndreea GorbanescuNo ratings yet
- Possibility of Unilateral Cast Partial Denture A Case ReportDocument8 pagesPossibility of Unilateral Cast Partial Denture A Case ReportAndreea GorbanescuNo ratings yet
- Retention Assessment of High Performance Poly-Etheretherketone Removable Partial Denture FrameworksDocument9 pagesRetention Assessment of High Performance Poly-Etheretherketone Removable Partial Denture FrameworksAndreea GorbanescuNo ratings yet
- Rehabilitation of Patient With Immediate Cast Partial Denture Using Patient's Natural Maxillary Anterior TeethDocument6 pagesRehabilitation of Patient With Immediate Cast Partial Denture Using Patient's Natural Maxillary Anterior TeethMeta Anjany FirmansyahNo ratings yet
- 1 s2.0 S001185321830096X MainDocument16 pages1 s2.0 S001185321830096X MainSeto PNo ratings yet
- Evaluation of Two Protocols To Measure The Accuracy of Fixed Dental Prostheses An in Vitro StudyDocument5 pagesEvaluation of Two Protocols To Measure The Accuracy of Fixed Dental Prostheses An in Vitro StudyAndreea GorbanescuNo ratings yet
- 1577un 2026-01Document79 pages1577un 2026-01ngovantienNo ratings yet
- English Final QPDocument10 pagesEnglish Final QPYash ChouhanNo ratings yet
- Seminar Presentation On Management of Diabetic Ketoacidosis BY:Kelil Kedir (CII)Document34 pagesSeminar Presentation On Management of Diabetic Ketoacidosis BY:Kelil Kedir (CII)Meraol HusseinNo ratings yet
- Arbour2013 HypoplasiaDocument5 pagesArbour2013 HypoplasiaCarolina GomezNo ratings yet
- National Cancer Control Program OverviewDocument15 pagesNational Cancer Control Program OverviewAparna Kingini100% (1)
- Steven Taylor - Cognitive-Behavioral Models of Health AnxietyDocument8 pagesSteven Taylor - Cognitive-Behavioral Models of Health AnxietyAnalia SierraNo ratings yet
- Orthopedics in Reptiles and Amphibians: ArticleDocument17 pagesOrthopedics in Reptiles and Amphibians: Articleagus setiawanNo ratings yet
- Gen Bio PDFDocument6 pagesGen Bio PDFGwyne Shenette Karylle NoscalNo ratings yet
- Subarachnoid Hemorrhage: Overview and RecommendationsDocument56 pagesSubarachnoid Hemorrhage: Overview and RecommendationsSarah Shafa MarwadhaniNo ratings yet
- Margi KC Amavata 2Document54 pagesMargi KC Amavata 2hetvi.m.patel.1999No ratings yet
- All Hazards Public Health Emergency Response PlanDocument77 pagesAll Hazards Public Health Emergency Response PlanHartford CourantNo ratings yet
- Emergency First Aid and CPRDocument15 pagesEmergency First Aid and CPRvhlactaotaoNo ratings yet
- Teaching P. E & HEALTH Sir BacnisDocument11 pagesTeaching P. E & HEALTH Sir BacnisLovely CarbonelNo ratings yet
- CWTS Final For InstructorDocument147 pagesCWTS Final For Instructorbarbie janeNo ratings yet
- DepEd LCP July3Document49 pagesDepEd LCP July3Jelai ApallaNo ratings yet
- Sanjeevani BookDocument16 pagesSanjeevani BookAmit SinghNo ratings yet
- Special South Carolina Pecan Festival Section InsideDocument14 pagesSpecial South Carolina Pecan Festival Section Insidenriddick03No ratings yet
- Beta - Lactam Antibiotics: Prof. R. K. Dixit Pharmacology and Therapeutics K. G. M. U. LucknowDocument29 pagesBeta - Lactam Antibiotics: Prof. R. K. Dixit Pharmacology and Therapeutics K. G. M. U. LucknowHely PatelNo ratings yet
- Cronic Kidney Disease: Prof. Dr. Agus Tessy SP - PD KGH Systema UrologiDocument39 pagesCronic Kidney Disease: Prof. Dr. Agus Tessy SP - PD KGH Systema UrologifauziyahabidahNo ratings yet
- Tests for Liver Function: Serum BilirubinDocument4 pagesTests for Liver Function: Serum BilirubinHiba EmadNo ratings yet
- Descriptors for Vigna aconitifolia and V. trilobata plant varietiesDocument44 pagesDescriptors for Vigna aconitifolia and V. trilobata plant varietiesprayogaNo ratings yet
- June 2022 QP - Component 3 Eduqas Biology A-LevelDocument44 pagesJune 2022 QP - Component 3 Eduqas Biology A-LeveltariffgillNo ratings yet