You might also like
- Pedia Prevous Board Questions PDFDocument103 pagesPedia Prevous Board Questions PDFJulius Matthew LuzanaNo ratings yet
- Rescue and Carry Methods Power PointDocument75 pagesRescue and Carry Methods Power PointJean Minette Prado88% (8)
- Nurses Notes Case 8Document4 pagesNurses Notes Case 8JERRYMAE RIVERANo ratings yet
- Hypertension - A Companion To Braunwald - S Heart Disease 3rd Edition (2017)Document503 pagesHypertension - A Companion To Braunwald - S Heart Disease 3rd Edition (2017)JOLANDA ANGELIN100% (1)
- Nursing Care Plan: Epidural Hematoma Post CraniotomyDocument14 pagesNursing Care Plan: Epidural Hematoma Post CraniotomyTepperoni78% (23)
- Myasthenia GravisDocument7 pagesMyasthenia Gravisエド パジャロン100% (1)
- Clinical Replacement Student Packet-2Document12 pagesClinical Replacement Student Packet-2ida50% (2)
- Nursing Care Plan For CholecystitisDocument4 pagesNursing Care Plan For CholecystitisEemyaj Jaymee88% (8)
- Nursing Care Plan For Covid-19 PatientDocument4 pagesNursing Care Plan For Covid-19 PatientAkande83% (6)
- Chapter 25: Assessment: Respiratory System Harding: Lewis's Medical-Surgical Nursing, 11th EditionDocument9 pagesChapter 25: Assessment: Respiratory System Harding: Lewis's Medical-Surgical Nursing, 11th EditionKrishna RamaNo ratings yet
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- NCP (Appendicitis)Document3 pagesNCP (Appendicitis)Jenny Ajoc100% (1)
- Time Chart: Data Action ResponseDocument2 pagesTime Chart: Data Action ResponseAziil Liiza100% (2)
- English For NursesDocument166 pagesEnglish For NursesAlexandrutza IuliaNo ratings yet
- Nursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceDocument6 pagesNursing Care Plan: Lorma Colleges Con Template Related Learning ExperiencePauline GarciaNo ratings yet
- Enteral Tube FeedingDocument9 pagesEnteral Tube FeedingneuronurseNo ratings yet
- Strovac Prospect EnglishDocument6 pagesStrovac Prospect EnglishSorin Rusu75% (4)
- Case Study, Chapter 20, Assessment of Respiratory FunctionDocument11 pagesCase Study, Chapter 20, Assessment of Respiratory FunctionMaddyNo ratings yet
- NCP of Respiratory DistressDocument3 pagesNCP of Respiratory DistressDarwin QuirimitNo ratings yet
- NCP Priority1Document13 pagesNCP Priority1Jezebhel ArestaNo ratings yet
- Cristobal, Rocelyn P. MS Lec Post Task Triage FinalDocument10 pagesCristobal, Rocelyn P. MS Lec Post Task Triage FinalRocelyn CristobalNo ratings yet
- Nursing Care Plan: Cystic FibrosisDocument4 pagesNursing Care Plan: Cystic FibrosisYael EzraNo ratings yet
- NCM 118 SDL#1 - Orcullo 4NFDocument5 pagesNCM 118 SDL#1 - Orcullo 4NFGerelNo ratings yet
- Laude Unit 8 Assignment Part 1 - ISBARDocument6 pagesLaude Unit 8 Assignment Part 1 - ISBARLacangan, Thea YvonneNo ratings yet
- Clinical Case Study - Online Discussion Form Fall 2020-1Document14 pagesClinical Case Study - Online Discussion Form Fall 2020-1Sabrina Odies100% (1)
- APPENDICITISDocument15 pagesAPPENDICITISTiffany AdriasNo ratings yet
- APOLONIO, Reyjan L. (NCP 1)Document2 pagesAPOLONIO, Reyjan L. (NCP 1)REYJAN APOLONIONo ratings yet
- University of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisDocument3 pagesUniversity of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisLyn MhoreNo ratings yet
- TTP Care Plan 1 JevansDocument8 pagesTTP Care Plan 1 Jevansapi-439893609No ratings yet
- This Study Resource WasDocument3 pagesThis Study Resource WasCarlito AglipayNo ratings yet
- Date/Shift Focus DataDocument2 pagesDate/Shift Focus Datakuro hanabusaNo ratings yet
- Lung Cancer N C P BY BHERU LALDocument2 pagesLung Cancer N C P BY BHERU LALBheru Lal100% (1)
- LACANGAN Unit 8 Assignment Part 1 - ISBARDocument3 pagesLACANGAN Unit 8 Assignment Part 1 - ISBARLacangan, Thea YvonneNo ratings yet
- A Nursing Care Plan Presented To The Faculty of The Nursing DepartmentDocument4 pagesA Nursing Care Plan Presented To The Faculty of The Nursing DepartmentAnge MinguitoNo ratings yet
- NP IiiDocument9 pagesNP IiiVia LatrasNo ratings yet
- Case Presentaion Pe (FinalDocument29 pagesCase Presentaion Pe (FinalFatema AkhterNo ratings yet
- RLE Case PresentationDocument26 pagesRLE Case PresentationShaine BalverdeNo ratings yet
- Fdar Lp6 MontemayorDocument5 pagesFdar Lp6 MontemayorEden Marie MangaserNo ratings yet
- Finalnursing Process ProjectDocument13 pagesFinalnursing Process Projectapi-531834240No ratings yet
- Nursing Care Ineffective Airway Clearance: Arranged byDocument9 pagesNursing Care Ineffective Airway Clearance: Arranged byAlri LestariNo ratings yet
- Case Presentation (2023)Document17 pagesCase Presentation (2023)Infection QcghNo ratings yet
- Ocne1 2supportDocument9 pagesOcne1 2supportapi-349380871No ratings yet
- Askep DialisisDocument6 pagesAskep Dialisisvictor zhefaNo ratings yet
- Peads CRDocument44 pagesPeads CRGoh Kwang YanNo ratings yet
- NCP PneumoniaDocument6 pagesNCP PneumoniaMerliah LofrancoNo ratings yet
- Subjective: "Nahihirapan Ako Huminga" As Verbalized by The Patient. Objective: Bt-38.5 C HR - 114 BPM BP - 110/70 MMHG RR - 28 BPM Diaphoretic RiDocument4 pagesSubjective: "Nahihirapan Ako Huminga" As Verbalized by The Patient. Objective: Bt-38.5 C HR - 114 BPM BP - 110/70 MMHG RR - 28 BPM Diaphoretic Ristrawberrykate26No ratings yet
- NCP For CAP TB.Document5 pagesNCP For CAP TB.Cherry Ann BalagotNo ratings yet
- 12b Clinical Update Example 2018Document9 pages12b Clinical Update Example 2018Ana BienneNo ratings yet
- DIVERTICULOSISDocument21 pagesDIVERTICULOSISTiffany AdriasNo ratings yet
- Final Na Jud Ni As In!Document19 pagesFinal Na Jud Ni As In!joyrena ochondraNo ratings yet
- Epp Bab 1-2Document17 pagesEpp Bab 1-2Ahmad BuchoriNo ratings yet
- 602 26.06.3 PDFDocument2 pages602 26.06.3 PDFAnnisa Rahma SariNo ratings yet
- Ulcerative ColitisDocument17 pagesUlcerative ColitisTiffany AdriasNo ratings yet
- A Case Study of RupturedDocument12 pagesA Case Study of RupturedkisNo ratings yet
- Thuy Functional DimensionDocument3 pagesThuy Functional DimensionTweetie PieNo ratings yet
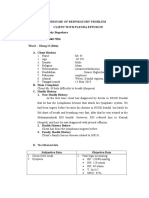
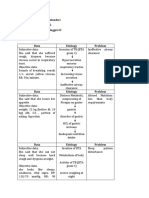
- Resume of Respiratory ProblemDocument5 pagesResume of Respiratory ProblemIbi Yulia SetyaniNo ratings yet
- Nursing Diagnosis Nursing Intervention Rationale Exchange: Prioritized Nursing Problem For Bronchopulmonary DisplasiaDocument9 pagesNursing Diagnosis Nursing Intervention Rationale Exchange: Prioritized Nursing Problem For Bronchopulmonary DisplasiaJinaan MahmudNo ratings yet
- NCPDocument3 pagesNCPJanelle Kate SaleNo ratings yet
- Assesment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssesment Diagnosis Planning Intervention Rationale EvaluationTrisha Suazo100% (1)
- Nama: Alif Lusy Wulandari Nim: 01.2.17.00592 Mata Kuliah: Bahasa Inggris IIDocument8 pagesNama: Alif Lusy Wulandari Nim: 01.2.17.00592 Mata Kuliah: Bahasa Inggris IIAlif lusy WulandariNo ratings yet
- Nurses Notes Case 8Document4 pagesNurses Notes Case 8JERRYMAE RIVERANo ratings yet
- Materi Nursing Care PlanDocument1 pageMateri Nursing Care PlanSiti nur Kholifatus samsiyahNo ratings yet
- NCP Case Analysis GastritisDocument7 pagesNCP Case Analysis GastritisSteffi GolezNo ratings yet
- Assessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoDocument5 pagesAssessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoMaria Francheska OsiNo ratings yet
- Covid 19 Pandemic With KeyDocument2 pagesCovid 19 Pandemic With KeyNan LibraNo ratings yet
- Jurnal Case Control UTS (Idrus) 5Document8 pagesJurnal Case Control UTS (Idrus) 5Reny NapitupuluNo ratings yet
- Neuromuscular Junction Disorders: Myasthenia GravisDocument20 pagesNeuromuscular Junction Disorders: Myasthenia GravisIzabella MihályNo ratings yet
- Cranial NervesDocument5 pagesCranial NervesTHE BLINKNo ratings yet
- UNDS111 Finals (Annotated)Document14 pagesUNDS111 Finals (Annotated)DELA CRUZ, JENISSE LOUISSENo ratings yet
- Central Dogma and Genetic MedicineDocument4 pagesCentral Dogma and Genetic MedicineedricNo ratings yet
- Fundamentals of Nursing PDocument31 pagesFundamentals of Nursing Papi-26587879100% (4)
- Public Health Competencies HandbookDocument33 pagesPublic Health Competencies Handbookapi-556450573No ratings yet
- ICU Related MCQ QuizDocument12 pagesICU Related MCQ Quizezzat salemNo ratings yet
- Myelomeningocele: A New Functional Classification: PerspectiveDocument5 pagesMyelomeningocele: A New Functional Classification: PerspectiveLema Ulloa ZoraidaNo ratings yet
- Ridwan Olawale: Dr. 'WaleDocument6 pagesRidwan Olawale: Dr. 'WaleRidwan OlawaleNo ratings yet
- Cone Beam CT Literature ReviewDocument6 pagesCone Beam CT Literature Reviewm1dyhuh1jud2100% (1)
- A Study On Impact of COVID-19 Lockdown On Psychological Health, Economy and Social Life of People in KashmirDocument12 pagesA Study On Impact of COVID-19 Lockdown On Psychological Health, Economy and Social Life of People in KashmirDavit SoesantoNo ratings yet
- 1-History-of-MedTech 2Document47 pages1-History-of-MedTech 2Sarah NiñoNo ratings yet
- Hybrid Deep Learning For Detecting Lung Diseases From X-Ray ImagesDocument14 pagesHybrid Deep Learning For Detecting Lung Diseases From X-Ray ImagesMurshedul ArifeenNo ratings yet
- Byjus Blood and Circulatory System Updated 95 2 Converted 1 48 37Document5 pagesByjus Blood and Circulatory System Updated 95 2 Converted 1 48 37ROHIT KUMAR YADAVNo ratings yet
- Resumen de La TV InglesDocument19 pagesResumen de La TV InglesIvette RamosNo ratings yet
- OMS 190807 - Prequalified - Product - ListDocument11 pagesOMS 190807 - Prequalified - Product - ListYeisy Yainira Leon Gomez100% (1)
- Defining Cognitive Reserve and Implications For Cognitive AgingDocument12 pagesDefining Cognitive Reserve and Implications For Cognitive AgingmarleimanNo ratings yet
- NSG 523 Module 10 Dissemination Grid For ProductDocument2 pagesNSG 523 Module 10 Dissemination Grid For Productapi-354069497No ratings yet
- Novita Tirodatu - 19704001 - Kelas A - Tugas Epidemiologi Kawasan PesisirDocument8 pagesNovita Tirodatu - 19704001 - Kelas A - Tugas Epidemiologi Kawasan PesisirNovita Tirodatu11No ratings yet
- Dissociative BehaviorDocument5 pagesDissociative BehaviorDump AccNo ratings yet
- Gambaran Dan Lesi Rahang Pada Radiograf: Border Periosteal ReactionDocument6 pagesGambaran Dan Lesi Rahang Pada Radiograf: Border Periosteal ReactionI Dewa Ayu SavitriNo ratings yet
- Fundamental of NursingDocument9 pagesFundamental of NursingDr-Marudhar MarudharNo ratings yet