You might also like
- Acute Coronary SyndromeDocument4 pagesAcute Coronary SyndromeHaryaman JustisiaNo ratings yet
- Unstable AnginaDocument5 pagesUnstable AnginaAria AlysisNo ratings yet
- Simulation Acute Coronary Syndrome (Learner)Document2 pagesSimulation Acute Coronary Syndrome (Learner)Wanda Nowell0% (1)
- ACS AMI FacilitatorDocument21 pagesACS AMI FacilitatorPaul Zantua57% (7)
- 440 - Med Surg HESI 2Document8 pages440 - Med Surg HESI 2Chalcey Polson87% (15)
- ST-Elevation: N N N N N N N NDocument5 pagesST-Elevation: N N N N N N N NningputNo ratings yet
- Clin Cardiology CasesDocument34 pagesClin Cardiology CasesSunny Singh0% (1)
- Medical Emergency Oral Q.docx26.docx8Document44 pagesMedical Emergency Oral Q.docx26.docx8Simina ÎntunericNo ratings yet
- Chest Pain Protocol in EDDocument3 pagesChest Pain Protocol in EDshahidchaudharyNo ratings yet
- Cast Study 1Document4 pagesCast Study 1Thelda Mae Arteche SablanNo ratings yet
- Chest Pain Care PlanDocument2 pagesChest Pain Care Planapi-545292605No ratings yet
- Chest PainDocument9 pagesChest PainIlyes FerenczNo ratings yet
- Angina PectorisDocument11 pagesAngina PectorisJohn Matley CaampuedNo ratings yet
- 2004 Core SeptDocument147 pages2004 Core SeptSana QazilbashNo ratings yet
- Roll No - BR (On) - 2, Kaung Htike San, PresentationDocument22 pagesRoll No - BR (On) - 2, Kaung Htike San, PresentationHnin Thiri SoeNo ratings yet
- Approach To TruamaDocument29 pagesApproach To TruamaIbsa ShumaNo ratings yet
- Acute Miocard InfarkDocument32 pagesAcute Miocard InfarkhansNo ratings yet
- What Symptoms Should Lead The Nurse To Suspect The Pain May Be Angina?Document5 pagesWhat Symptoms Should Lead The Nurse To Suspect The Pain May Be Angina?Dylan Angelo AndresNo ratings yet
- Surgery Task 11Document9 pagesSurgery Task 11Qmobile J5No ratings yet
- Acute Myocardial Infarction: QuestionsDocument18 pagesAcute Myocardial Infarction: QuestionsAbdul QuyyumNo ratings yet
- A Case Study of Chronic Calculous CholecystitisDocument9 pagesA Case Study of Chronic Calculous CholecystitisMeine Mheine0% (1)
- Critical Care MCI CCU AssignmentDocument14 pagesCritical Care MCI CCU AssignmentTukiminNo ratings yet
- Patient Diagnosed With Myocardial Infarct M006Document11 pagesPatient Diagnosed With Myocardial Infarct M006Kefix WritersHubNo ratings yet
- Biomarkers in The Emergency Workup of Chest Pain (CCJM 2013)Document10 pagesBiomarkers in The Emergency Workup of Chest Pain (CCJM 2013)Luis Gerardo Alcalá GonzálezNo ratings yet
- Lita SantosDocument3 pagesLita SantosMaye Arugay100% (1)
- CH 09Document71 pagesCH 09api-308826929No ratings yet
- Acute Coronary Syndrome - A Case StudyDocument11 pagesAcute Coronary Syndrome - A Case StudyRocel Devilles100% (2)
- Alteration in Cardiac Output Related To ST ElevationDocument58 pagesAlteration in Cardiac Output Related To ST Elevationapi-675533626No ratings yet
- Of The Multiply Injured PatientDocument29 pagesOf The Multiply Injured PatientAjay DherwaniNo ratings yet
- Mutt and JeffDocument8 pagesMutt and Jeffyoyo1rn100% (2)
- Case Scenario 1 - P3W1Document4 pagesCase Scenario 1 - P3W1Chaz BayanaNo ratings yet
- CADDocument2 pagesCADJessica Koch100% (1)
- Week 5 ChestPain Student HODocument8 pagesWeek 5 ChestPain Student HOVindicated ReignNo ratings yet
- Approach To Trauma: UNC Emergency Medicine Medical Student Lecture SeriesDocument54 pagesApproach To Trauma: UNC Emergency Medicine Medical Student Lecture SeriesAhmed Tawfig GamalNo ratings yet
- Assessment of Chest Pain in Primary CareDocument8 pagesAssessment of Chest Pain in Primary CareVictoria GomezNo ratings yet
- Care of Clients With Cardiovascular DisordersDocument67 pagesCare of Clients With Cardiovascular DisordersMatt Lao DionelaNo ratings yet
- Pathophysiology/Epidemiology of Acute Coronary Syndromes: 1 2 November 2019Document15 pagesPathophysiology/Epidemiology of Acute Coronary Syndromes: 1 2 November 2019anasNo ratings yet
- CVS Physio Case Files p1Document4 pagesCVS Physio Case Files p1dawnparkNo ratings yet
- 'Batangas Medical Center Case Report by PGI Carlos H. AcuñaDocument7 pages'Batangas Medical Center Case Report by PGI Carlos H. AcuñaCarlos H. AcuñaNo ratings yet
- ACLS Secondary Survey For A Patient in Respiratory Arrest: BLS Arrest Figure 1. Basic Life Support Primary SurveyDocument30 pagesACLS Secondary Survey For A Patient in Respiratory Arrest: BLS Arrest Figure 1. Basic Life Support Primary SurveyLusia NataliaNo ratings yet
- 978190medicine5635856 PDFDocument18 pages978190medicine5635856 PDFMuhammad TariqNo ratings yet
- Approach For Poly-Trauma PatientDocument63 pagesApproach For Poly-Trauma PatientvadimmadanNo ratings yet
- Acute Coronary Syndrome: Rich Derby, LT Col, USAF MGMC Family Practice ProgramDocument56 pagesAcute Coronary Syndrome: Rich Derby, LT Col, USAF MGMC Family Practice ProgramSabilul Huda100% (1)
- 062 Cerebral-Challenge 5 Update 2011 PDFDocument5 pages062 Cerebral-Challenge 5 Update 2011 PDFcignalNo ratings yet
- Acute PericarditisDocument7 pagesAcute PericarditisMirza AlfiansyahNo ratings yet
- Case Presentation RADocument6 pagesCase Presentation RAdocv526No ratings yet
- UPDATED MANAGEMENT OF HEART ATTACK AND ACS IN EMERGENCY CONDITION - Dr. Imran Khan JallaldeenDocument30 pagesUPDATED MANAGEMENT OF HEART ATTACK AND ACS IN EMERGENCY CONDITION - Dr. Imran Khan Jallaldeendrsrisubekti05No ratings yet
- Lapkas VT RevisiDocument13 pagesLapkas VT RevisiRannyNo ratings yet
- ED Approach To Trauma DR Haimanot Tessema Assistant Professor, EMCC (ST Pauls Mellinium Medical College) April, 2022Document51 pagesED Approach To Trauma DR Haimanot Tessema Assistant Professor, EMCC (ST Pauls Mellinium Medical College) April, 2022Temesgen GeletaNo ratings yet
- Topic 10 Internal Medicine Ali SaifDocument5 pagesTopic 10 Internal Medicine Ali SaifAnkit Kumar PatelNo ratings yet
- Protocol 13: Chest Pain: A&E DoctorDocument4 pagesProtocol 13: Chest Pain: A&E DoctorVanessa HermioneNo ratings yet
- QSEN Simulation Template Post CABG PatientDocument8 pagesQSEN Simulation Template Post CABG PatientMissK2216No ratings yet
- Laporan Tutorial Kelompok 1 Skenario 2Document11 pagesLaporan Tutorial Kelompok 1 Skenario 2Anita Dwi srirahayuNo ratings yet
- Cardiovascular System: AnatomyDocument19 pagesCardiovascular System: AnatomyStephanie MacVeighNo ratings yet
- Acute Coronary Syndromes AlgorithmDocument5 pagesAcute Coronary Syndromes AlgorithmLiuk IrawatiNo ratings yet
- DEFIBrilatorDocument43 pagesDEFIBrilatoranon_632568468No ratings yet
- KINE-311-4 Neuromuscular Clase 4Document40 pagesKINE-311-4 Neuromuscular Clase 4Gonzalo RetamalNo ratings yet
- Blood CoagulationDocument8 pagesBlood CoagulationJaslir MendozaNo ratings yet
- SodaPDF Merged Merging ResultDocument648 pagesSodaPDF Merged Merging ResultFaith madayagNo ratings yet
- Christopher Cheung Approach To Cardiac History Taking: Cyanosis or SyncopeDocument6 pagesChristopher Cheung Approach To Cardiac History Taking: Cyanosis or SyncopeApryl Phyllis JimenezNo ratings yet
- BFR Training Book v3 PDFDocument45 pagesBFR Training Book v3 PDFMATTHEW100% (1)
- 37 - Shock in ObstetricsDocument22 pages37 - Shock in Obstetricsdr_asaleh90% (10)
- The Fitness Fatigue Model Revisited ImplicationsDocument10 pagesThe Fitness Fatigue Model Revisited ImplicationsLucas AvellanNo ratings yet
- Hubungan Paparan Suhu Dingin Terhadap Perubahan Tekanan Darah Sebelum Dan Sesudah BekerjaDocument4 pagesHubungan Paparan Suhu Dingin Terhadap Perubahan Tekanan Darah Sebelum Dan Sesudah BekerjaRomydaQurrotinA'yuniNo ratings yet
- Drug Study Ob WardDocument7 pagesDrug Study Ob WardKc DichosoNo ratings yet
- Basic ECG ReadingDocument41 pagesBasic ECG ReadingBenj100% (4)
- Edexcel Circulary System Past Paper Questions 1Document10 pagesEdexcel Circulary System Past Paper Questions 1binura desilvaNo ratings yet
- Practice ECGStripsDocument300 pagesPractice ECGStripsrobby zayendraNo ratings yet
- Sleep Medicine Reviews: Michel Billiard, Karel SonkaDocument11 pagesSleep Medicine Reviews: Michel Billiard, Karel SonkaCharlotteGraceNusiferaNo ratings yet
- Le3sso Guide 1 Module Plan First Quarter Biology PDFDocument29 pagesLe3sso Guide 1 Module Plan First Quarter Biology PDFconstancia G, caraan100% (1)
- General Physiology PDFDocument11 pagesGeneral Physiology PDFmedpgnotes100% (4)
- Care of Clients With Physiologic and Psychosocial AlterationsDocument34 pagesCare of Clients With Physiologic and Psychosocial AlterationsChloie Marie RosalejosNo ratings yet
- Sherwood Cardiac PhysiologyDocument40 pagesSherwood Cardiac PhysiologyEvan Permana100% (2)
- Rabbit Jejunum ExperimentDocument4 pagesRabbit Jejunum ExperimentscrinNo ratings yet
- 7 Ways To Minimize Jet LagDocument5 pages7 Ways To Minimize Jet LagDivyajyoti DevaNo ratings yet
- Registar Za Akutni Koronarni Sindrom U Srbiji 2010Document127 pagesRegistar Za Akutni Koronarni Sindrom U Srbiji 2010Poledica MladenNo ratings yet
- Webinar Amal International Pedis Care FoundationDocument31 pagesWebinar Amal International Pedis Care Foundationdon rangerNo ratings yet
- Axillary MethodDocument5 pagesAxillary MethodJerica Jaz F. VergaraNo ratings yet
- Heart Failure: Diagnosis and EvaluationDocument29 pagesHeart Failure: Diagnosis and Evaluation黃昱睿No ratings yet
- Echo Report : (Abridged)Document4 pagesEcho Report : (Abridged)Ajay KarolNo ratings yet
- NSP Oec Ch30 LectureDocument63 pagesNSP Oec Ch30 LecturemaithamNo ratings yet
- Respiration Aerobic and Anaerobic Respiration 1Document17 pagesRespiration Aerobic and Anaerobic Respiration 1FOR studiesNo ratings yet
- Activity 9 Secondary Growth of Roots and StemsDocument10 pagesActivity 9 Secondary Growth of Roots and StemsGenghis SupnetNo ratings yet
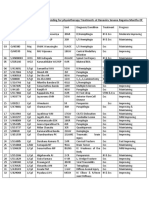
- Progress Report of Indoor Patients Attending For Physiotherapy Treatment atDocument6 pagesProgress Report of Indoor Patients Attending For Physiotherapy Treatment atIsuru DasanthaNo ratings yet
- NCM 112 Care of Clients With Problems in Oxygenation, Fluid and Electrolytes, Infectious, Inflammatory & Immunologic ReactionDocument52 pagesNCM 112 Care of Clients With Problems in Oxygenation, Fluid and Electrolytes, Infectious, Inflammatory & Immunologic ReactionJIMENEZ, TRISHA MARIE D.100% (1)
- Defibrillator Life GainDocument5 pagesDefibrillator Life GainhasyikinNo ratings yet