You might also like
- Anatomy and Blood Supply of AppendixDocument30 pagesAnatomy and Blood Supply of AppendixForam PatelNo ratings yet
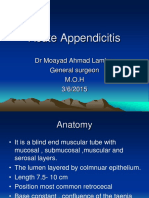
- Acute Appendicitis: M. Iqbal RivaiDocument22 pagesAcute Appendicitis: M. Iqbal Rivai2211418No ratings yet
- KP 2.4.2.3 - AppendixDocument25 pagesKP 2.4.2.3 - AppendixnadiaNo ratings yet
- Appendicitis 1Document25 pagesAppendicitis 1nelsonNo ratings yet
- Gastro Week 4Document39 pagesGastro Week 4Reynaldi FernandesNo ratings yet
- Problem 4 GITDocument94 pagesProblem 4 GITArioNo ratings yet
- I Am Sharing 'Class - 4 - GIT' With You - 240122 - 164403Document21 pagesI Am Sharing 'Class - 4 - GIT' With You - 240122 - 164403phuyalaryan666No ratings yet
- PeritonitisDocument20 pagesPeritonitisYasirNo ratings yet
- The Penis: - Phimosis: Scarring of The Prepuce Which Will Not Retract Without FissuringDocument20 pagesThe Penis: - Phimosis: Scarring of The Prepuce Which Will Not Retract Without FissuringWorku KifleNo ratings yet
- Acute Pyelonephritis IN PregnancyDocument12 pagesAcute Pyelonephritis IN PregnancyAnivasa KabirNo ratings yet
- Common Congenital Git Malformations FinDocument60 pagesCommon Congenital Git Malformations FinRuth DanielNo ratings yet
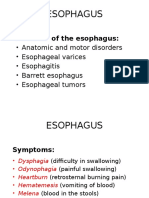
- Diseases of OesophagusDocument46 pagesDiseases of OesophagusBrother GeorgeNo ratings yet
- GIT PathologyDocument27 pagesGIT PathologyIshali NuwanjiniNo ratings yet
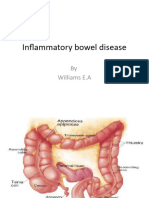
- Inflammatory Bowel DiseaseDocument52 pagesInflammatory Bowel DiseaseWilliams Emmanuel AdeyeyeNo ratings yet
- Large Bowel ObstructionDocument36 pagesLarge Bowel Obstructionpuleng matshabaNo ratings yet
- The AppendixDocument5 pagesThe AppendixAmik, Aila H.No ratings yet
- Gastrointestinal Tract (Partial Edit)Document47 pagesGastrointestinal Tract (Partial Edit)applesncoreNo ratings yet
- Male Genital SystemDocument75 pagesMale Genital Systemyaumilagus100% (1)
- Inflammatory Bowel DiseaseDocument51 pagesInflammatory Bowel DiseaseTeena Chandran100% (1)
- Appendix Part 1Document8 pagesAppendix Part 1Abdullah EssaNo ratings yet
- Esophagous Stomach Small Intestine PathologyDocument58 pagesEsophagous Stomach Small Intestine PathologytahaNo ratings yet
- AppendicitisDocument38 pagesAppendicitisEmaan Tanveer100% (1)
- Bowel Obstruction and Tumors SheetDocument19 pagesBowel Obstruction and Tumors SheetAbu Ibtihal OsmanNo ratings yet
- Kelainan Pada Usus HalusDocument28 pagesKelainan Pada Usus HalusClara Shinta AruanNo ratings yet
- Pancreatic Diseases: Dr. Norizal Mohd NoorDocument53 pagesPancreatic Diseases: Dr. Norizal Mohd NoorTower AlangNo ratings yet
- Abdominal Pain in ChildrenDocument21 pagesAbdominal Pain in ChildrenDaniel RajNo ratings yet
- Small & Large Bowel SlidesDocument17 pagesSmall & Large Bowel SlidesHunter ClontsNo ratings yet
- Lecture 9 GitDocument42 pagesLecture 9 GitWaqar Ul HaqNo ratings yet
- Ulcerative ColitisDocument63 pagesUlcerative ColitismahalakshmiNo ratings yet
- Learning Objectives in Gastrointestinal PathologyDocument15 pagesLearning Objectives in Gastrointestinal PathologyZul Azim AnuarNo ratings yet
- Esophagus: Diseases of The EsophagusDocument60 pagesEsophagus: Diseases of The EsophagusSalma NajjarNo ratings yet
- Large Intestine, PancreasDocument30 pagesLarge Intestine, PancreasElijah WoodNo ratings yet
- Intestinal ObstructionDocument56 pagesIntestinal ObstructionGiovanna AlguNo ratings yet
- Abdominal Emergencies Presentation (Recovered)Document126 pagesAbdominal Emergencies Presentation (Recovered)kityamuwesiNo ratings yet
- Perforated Peptic UlcerDocument68 pagesPerforated Peptic UlcerSaibo BoldsaikhanNo ratings yet
- Cystic FibrosisDocument15 pagesCystic FibrosisRupesh M DasNo ratings yet
- Abnormalities in Small Bowel: Dr. Iqbal Pahlevi, SPB, SpbaDocument36 pagesAbnormalities in Small Bowel: Dr. Iqbal Pahlevi, SPB, SpbafinikollinsNo ratings yet
- Colon, Rectum and AnusDocument30 pagesColon, Rectum and AnusKiara GovenderNo ratings yet
- 4.. ReproDocument61 pages4.. Reprosabin luitelNo ratings yet
- 2-Acute Abdominal PainDocument24 pages2-Acute Abdominal Painabdalmajeed alshammaryNo ratings yet
- First Problem: Erwin Budi/405130151Document42 pagesFirst Problem: Erwin Budi/405130151Rilianda SimbolonNo ratings yet
- Acute Appendic ItsDocument24 pagesAcute Appendic ItsDr-Wisam Mhmd AliNo ratings yet
- Pseudotuberculosis 191204160344Document13 pagesPseudotuberculosis 191204160344padmaNo ratings yet
- Acute Abdomin DFHCDocument72 pagesAcute Abdomin DFHCAhmed noor Ahmed noorNo ratings yet
- Summary For Acute AppendicitisDocument13 pagesSummary For Acute AppendicitisFemale calmNo ratings yet
- Patho SlidesDocument46 pagesPatho Slidesapi-400411160No ratings yet
- Jaundice: Checklist For HistoryDocument17 pagesJaundice: Checklist For HistoryMustafa H. KadhimNo ratings yet
- Esophageal DisordersDocument37 pagesEsophageal DisordersDanielle FosterNo ratings yet
- PA GI Tract Skuad Tandingan Elnineno!Document281 pagesPA GI Tract Skuad Tandingan Elnineno!Arsya AliNo ratings yet
- Appendicitis 5.9Document50 pagesAppendicitis 5.9Smart SaravanaNo ratings yet
- DiverticulitisDocument23 pagesDiverticulitisSuhanda SaputraNo ratings yet
- 07c. Non Neoplastic Disease of The Small and Large IntestineDocument49 pages07c. Non Neoplastic Disease of The Small and Large Intestine21701101016 - Juliana Ayu NugrahaNo ratings yet
- College of Medicine & Health SciencesDocument56 pagesCollege of Medicine & Health SciencesMebratu DemessNo ratings yet
- Intestinal Obstruction: MSU Medical Students. Batch 2. Group 2Document31 pagesIntestinal Obstruction: MSU Medical Students. Batch 2. Group 2Qp Nizam100% (2)
- Amoebiasis - and GiardiasisDocument59 pagesAmoebiasis - and GiardiasisSaurabh AgarwalNo ratings yet
- Antenatal Obstetric ComplicationsDocument40 pagesAntenatal Obstetric ComplicationsArhum SiddiqiNo ratings yet
- Surgry Lecture For Medical Studentes: By: Shitahun ADocument37 pagesSurgry Lecture For Medical Studentes: By: Shitahun ASisay FentaNo ratings yet
- 1.7B AppendixDocument4 pages1.7B AppendixDulce Kriselda E. FaigmaniNo ratings yet
- Colonic and Small Intestine Disorders-1Document28 pagesColonic and Small Intestine Disorders-1YIKI ISAACNo ratings yet
- What Is Your Diagnosis?: A. Inguinal HerniaDocument3 pagesWhat Is Your Diagnosis?: A. Inguinal Herniajitendra magarNo ratings yet
- Hollow Viscous PerforationDocument25 pagesHollow Viscous Perforationjitendra magarNo ratings yet
- 9.renal Stone QuizDocument27 pages9.renal Stone Quizjitendra magarNo ratings yet
- Benign Prostatic HypertrophyDocument45 pagesBenign Prostatic Hypertrophyjitendra magarNo ratings yet
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDocument37 pagesAcute Coronary Syndrome / Acute Myocardial Infarction Algorithmjitendra magarNo ratings yet
- ElectrocardiogramDocument169 pagesElectrocardiogramjitendra magarNo ratings yet
- Gestational Trophoblastic DiseaseDocument88 pagesGestational Trophoblastic Diseasejitendra magarNo ratings yet
- 1.prof Gopal Sir Book4563661704814604902Document263 pages1.prof Gopal Sir Book4563661704814604902jitendra magarNo ratings yet
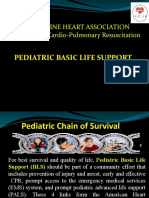
- Pediatric Basic Life Support: Philippine Heart Association Council On Cardio-Pulmonary ResuscitationDocument106 pagesPediatric Basic Life Support: Philippine Heart Association Council On Cardio-Pulmonary Resuscitationjitendra magar100% (1)
- Inguinal Hernias: Trix M. Asuncion M.D. General SurgeryDocument55 pagesInguinal Hernias: Trix M. Asuncion M.D. General Surgeryjitendra magarNo ratings yet
- 7.intest - Obstruc. QuizDocument3 pages7.intest - Obstruc. Quizjitendra magarNo ratings yet
- 11 BurnDocument31 pages11 Burnjitendra magarNo ratings yet
- 4.gall StoneDocument35 pages4.gall Stonejitendra magarNo ratings yet
- 6.head InjuryDocument37 pages6.head Injuryjitendra magarNo ratings yet
- The Role of Acute Phase Proteins in Diagnosis and ManagementDocument6 pagesThe Role of Acute Phase Proteins in Diagnosis and ManagementCabinet VeterinarNo ratings yet
- Comparison Between Prone and Supine Position Imrt For Endometrial Cancer (2007)Document5 pagesComparison Between Prone and Supine Position Imrt For Endometrial Cancer (2007)Michelle LEINo ratings yet
- Teaching-Plan-Health-Education-Plan-Diabetes Mellitus TYPE IIDocument3 pagesTeaching-Plan-Health-Education-Plan-Diabetes Mellitus TYPE IIkasjdkasNo ratings yet
- ROJoson PEP Talk: RUQ Abdominal Pain and Gallbladder DisordersDocument80 pagesROJoson PEP Talk: RUQ Abdominal Pain and Gallbladder DisordersrojosonNo ratings yet
- Periodontal DiseasesDocument47 pagesPeriodontal DiseasesPratikNo ratings yet
- The Vaccine Adverse Event Reporting System (VAERS) (2) 091621Document475 pagesThe Vaccine Adverse Event Reporting System (VAERS) (2) 091621jb_uspuNo ratings yet
- Glimepiride Prescribing InformationDocument16 pagesGlimepiride Prescribing InformationMohammed Shamiul ShahidNo ratings yet
- Drug Analysis: Submitted By: GALICINAO, Gretta Shalou GDocument9 pagesDrug Analysis: Submitted By: GALICINAO, Gretta Shalou GggalicinaoNo ratings yet
- Menstrupedia Comic: The Friendly Guide To Periods For Girls (2014), by Aditi Gupta, Tuhin Paul, and Rajat MittalDocument4 pagesMenstrupedia Comic: The Friendly Guide To Periods For Girls (2014), by Aditi Gupta, Tuhin Paul, and Rajat MittalMy Home KaviNo ratings yet
- ScoliosisDocument99 pagesScoliosismarjan dronjakNo ratings yet
- M.O.S DismantlingDocument18 pagesM.O.S DismantlingAhmed Khaled100% (1)
- Clinician - S Guide To Sleep Disorders (Watson - Vaughn, 2006) PDFDocument411 pagesClinician - S Guide To Sleep Disorders (Watson - Vaughn, 2006) PDFMarta PamolNo ratings yet
- Others Districts Others Districts Others Districts Others DistrictsDocument6 pagesOthers Districts Others Districts Others Districts Others DistrictsThulasiraman AshokkumarNo ratings yet
- S Curvy .: Lobna Hani HijliDocument4 pagesS Curvy .: Lobna Hani Hijlilobna HijliNo ratings yet
- Vestibular Function TestsDocument11 pagesVestibular Function TestsM. Arief Purnanta0% (1)
- Kenyaemr V17.3.1 Release Notes: Integration With Eid, Adt & Differential Upload DescriptionDocument3 pagesKenyaemr V17.3.1 Release Notes: Integration With Eid, Adt & Differential Upload DescriptionMigori Art DataNo ratings yet
- Janet RowleyDocument1 pageJanet RowleyANA GABRIELA PEREZ VIDALNo ratings yet
- White Tongue Causes & 10 Natural Treatments For White Tongue - Dr. AxeDocument10 pagesWhite Tongue Causes & 10 Natural Treatments For White Tongue - Dr. AxeRaghu100% (1)
- 1000 Ques & Ans File 2Document54 pages1000 Ques & Ans File 2bibin joyNo ratings yet
- Hospital MarketingDocument10 pagesHospital MarketingYogesh Parchani100% (1)
- Ebook Gabbes Obstetrics Essentials Normal Problem Pregnancies PDF Full Chapter PDFDocument67 pagesEbook Gabbes Obstetrics Essentials Normal Problem Pregnancies PDF Full Chapter PDFandre.davis379100% (27)
- D Dimer Test in VTEDocument35 pagesD Dimer Test in VTEscribmedNo ratings yet
- "The Man Who Mistook His Wife For Hat" Is ADocument9 pages"The Man Who Mistook His Wife For Hat" Is AIADT Psy50% (2)
- CN 9-12Document6 pagesCN 9-12The Real UploaderNo ratings yet
- 25 Nutritional Dermatoses PDFDocument2 pages25 Nutritional Dermatoses PDFIan Greg Sunday FootstepNo ratings yet
- Crisis Management Covid 19Document22 pagesCrisis Management Covid 19jon elleNo ratings yet
- Status EpilepticusDocument17 pagesStatus EpilepticusXavier AbrilNo ratings yet
- Collarbone Breathing TreatmentDocument4 pagesCollarbone Breathing TreatmentPatrizioNo ratings yet
- Risk For Decreased Cardiac Output: Nursing DiagnosisDocument4 pagesRisk For Decreased Cardiac Output: Nursing DiagnosisRiska RamadaniNo ratings yet
- Pathology Supplement Handout Nov 2018Document25 pagesPathology Supplement Handout Nov 2018Zak Kaz100% (2)