You might also like
- Nasha Mukt Bharat PPT For VolunteersDocument27 pagesNasha Mukt Bharat PPT For Volunteersvaishali TMU student100% (4)
- Tofacitinib: A Review in Rheumatoid ArthritisDocument15 pagesTofacitinib: A Review in Rheumatoid ArthritisPaulina Soto ValladaresNo ratings yet
- Meier 2013Document20 pagesMeier 2013James McmillanNo ratings yet
- F Fe Ea Attu Urre E: Pharmacotherapy of Rheumatoid ArthritisDocument2 pagesF Fe Ea Attu Urre E: Pharmacotherapy of Rheumatoid ArthritisMoisés PonceNo ratings yet
- Rheumatoid Arthritis: Ika Norcahyanti Fakultas Farmasi UNEJDocument59 pagesRheumatoid Arthritis: Ika Norcahyanti Fakultas Farmasi UNEJnimas putriNo ratings yet
- Biological Treatment in RADocument34 pagesBiological Treatment in RANourhanne Nagy AllamNo ratings yet
- Drug Therapy in RaDocument37 pagesDrug Therapy in Rasantosh subediNo ratings yet
- RheumatologyDocument6 pagesRheumatologyengelichtNo ratings yet
- Antirheumatic and Antigout DrugsDocument66 pagesAntirheumatic and Antigout DrugsBadri KarkiNo ratings yet
- General Principles and Overview of Management of Rheumatoid Arthritis in Adults - UpToDateDocument32 pagesGeneral Principles and Overview of Management of Rheumatoid Arthritis in Adults - UpToDateImad RifayNo ratings yet
- Rheumatoid ArthritisDocument45 pagesRheumatoid ArthritisThe AbyssinicansNo ratings yet
- Piis0025619611642572 PDFDocument6 pagesPiis0025619611642572 PDFSyifa MunawarahNo ratings yet
- Methotrexate in Rheumatoid Arthritis Efficacy and Safety 2329 6887 2 127Document4 pagesMethotrexate in Rheumatoid Arthritis Efficacy and Safety 2329 6887 2 127Saifuddin HaswareNo ratings yet
- Rheumatoid Arthritis: Pharmacological StrategiesDocument16 pagesRheumatoid Arthritis: Pharmacological StrategiesRavi Kumar NimmapatiNo ratings yet
- Dolor Articular y MuscularDocument5 pagesDolor Articular y MuscularDaniel López CastañoNo ratings yet
- Artitis ReumatoideDocument42 pagesArtitis ReumatoideMarlon Arias MadridNo ratings yet
- Will Pharmacogenetics Allow Better Prediction of MTX Toxicity and Efficacy in Patients With Rheumatoid ArthritisDocument7 pagesWill Pharmacogenetics Allow Better Prediction of MTX Toxicity and Efficacy in Patients With Rheumatoid Arthritisdoc0814No ratings yet
- MR 0779Document9 pagesMR 0779Dr-Kishna SenwarNo ratings yet
- NsaidDocument17 pagesNsaidFirst LastNo ratings yet
- Siemens Healthineers N Latex aTNFa AssayDocument8 pagesSiemens Healthineers N Latex aTNFa AssayMatej NekićNo ratings yet
- Annrheumdis 2020 January 79 1 19Document2 pagesAnnrheumdis 2020 January 79 1 19Ranindya PutriNo ratings yet
- New Drugs ArtritisDocument13 pagesNew Drugs ArtritisqfecrespoNo ratings yet
- Table 1. Indications For Initiating and Switching Nonbiologic and Biologic Dmards Disease Activity RecommendationDocument2 pagesTable 1. Indications For Initiating and Switching Nonbiologic and Biologic Dmards Disease Activity RecommendationRegina ArningsariNo ratings yet
- Therapeutic Drug Monitoring: An Overview of Commonly Monitored DrugsDocument7 pagesTherapeutic Drug Monitoring: An Overview of Commonly Monitored DrugsSerley WulandariNo ratings yet
- Disease Modifying Anti-Rheumatic Drugs DMARDsDocument8 pagesDisease Modifying Anti-Rheumatic Drugs DMARDsekoNo ratings yet
- 2016 Medical Ozone Increases Methotrexate Clinical Response and Improves Cellular Redox Balance in Patients With Rheumatoid ArthritisDocument6 pages2016 Medical Ozone Increases Methotrexate Clinical Response and Improves Cellular Redox Balance in Patients With Rheumatoid ArthritisAcupuntura de EquinosNo ratings yet
- Rheumatoid Arthritis: C. Treatment and AssessmentDocument9 pagesRheumatoid Arthritis: C. Treatment and AssessmentPerry MárquezNo ratings yet
- Comparative Tolerability Profiles of The Newer Versus Older AntidepressantsDocument29 pagesComparative Tolerability Profiles of The Newer Versus Older AntidepressantsJucas EscobarNo ratings yet
- Week 3 BiologicsDocument8 pagesWeek 3 BiologicsShree Narayan YadavNo ratings yet
- DynaMed Plus Rheumatoid ArthritisDocument20 pagesDynaMed Plus Rheumatoid ArthritisHeather Marie MathisNo ratings yet
- AR - TratamientoDocument9 pagesAR - TratamientomonseibanezbarraganNo ratings yet
- Bone and Joint Disorders RevisedDocument5 pagesBone and Joint Disorders RevisedAnthony PalladenoNo ratings yet
- CPG Rheumatic ArthritisDocument15 pagesCPG Rheumatic ArthritisCece PaduaNo ratings yet
- 583Document9 pages583Raichu Si Como NoNo ratings yet
- Rheumatoid ArthritisDocument49 pagesRheumatoid ArthritisDr.U.P.Rathnakar.MD.DIH.PGDHM100% (4)
- Drug Interaction of Methotrexate With Its AdjuvantDocument7 pagesDrug Interaction of Methotrexate With Its AdjuvantSarbjeet SinghNo ratings yet
- New Uses For Older DrugsDocument21 pagesNew Uses For Older DrugsSand JokeNo ratings yet
- Cannabis Et CancerDocument5 pagesCannabis Et CancerJoaquim MurtinhoNo ratings yet
- A Comprehensive Review of Current Treatments For Granulomatous Cheilitis (British Journal of Dermatology, Vol. 166, Issue 5) (2012)Document4 pagesA Comprehensive Review of Current Treatments For Granulomatous Cheilitis (British Journal of Dermatology, Vol. 166, Issue 5) (2012)Padmapriya SrinivasanNo ratings yet
- DMT and WBC InfectonDocument11 pagesDMT and WBC InfectonRenju KuriakoseNo ratings yet
- Clinical Case 1Document10 pagesClinical Case 1aveekumbharNo ratings yet
- Periodontology 2000 - 2019 - Golub - Periodontal Therapeutics Current Host Modulation Agents and Future DirectionsDocument19 pagesPeriodontology 2000 - 2019 - Golub - Periodontal Therapeutics Current Host Modulation Agents and Future DirectionsAdil KaukabNo ratings yet
- Adasfaadgdgadhahahadaadgda DFZF SFsaggggzsgzsggdgadhdaDocument21 pagesAdasfaadgdgadhahahadaadgda DFZF SFsaggggzsgzsggdgadhdaLili WidiantoNo ratings yet
- Personalized Medicine of Monoclonal Antibodies in in Ammatory Bowel Disease: Pharmacogenetics, Therapeutic Drug Monitoring, and BeyondDocument15 pagesPersonalized Medicine of Monoclonal Antibodies in in Ammatory Bowel Disease: Pharmacogenetics, Therapeutic Drug Monitoring, and BeyondJessica Asitimbay ZuritaNo ratings yet
- Wang 2018Document42 pagesWang 2018Erni SalehNo ratings yet
- JAK InhibitorsDocument40 pagesJAK InhibitorsMihaelaNo ratings yet
- Advancesinthetreatment Ofmultiplesclerosis: Carolyn Goldschmidt,, Marisa P. McginleyDocument13 pagesAdvancesinthetreatment Ofmultiplesclerosis: Carolyn Goldschmidt,, Marisa P. McginleyAsma Al-MahmoudNo ratings yet
- NIH Public Access: Author ManuscriptDocument19 pagesNIH Public Access: Author Manuscriptbravohr98No ratings yet
- Guidelines of Rheumatology CareDocument28 pagesGuidelines of Rheumatology Careआशिष दादाNo ratings yet
- Artritis Rematoidea PDFDocument12 pagesArtritis Rematoidea PDFJulian CipamochaNo ratings yet
- Tin Tore 2018Document6 pagesTin Tore 2018Nícolas CavalcanteNo ratings yet
- 1 Osteo and Rheumatoid ArthritisDocument62 pages1 Osteo and Rheumatoid ArthritisIbrahim BarhamNo ratings yet
- Tto Ar en QXDocument9 pagesTto Ar en QXCristobal UrreaNo ratings yet
- Immunomodulatory - Effects - of - Blood - Lettin20200723 31985 Eywblw With Cover Page v2Document14 pagesImmunomodulatory - Effects - of - Blood - Lettin20200723 31985 Eywblw With Cover Page v2Patryk StowaszewskiNo ratings yet
- Her N Ndez Rodrguez 2009Document12 pagesHer N Ndez Rodrguez 2009Gino Paul Bermeo ValcarcelNo ratings yet
- Cells: Highlights in Resistance Mechanism Pathways For Combination TherapyDocument29 pagesCells: Highlights in Resistance Mechanism Pathways For Combination TherapyHeru SigitNo ratings yet
- Department of Clinical Pharmacology Prof: Mervat EidDocument58 pagesDepartment of Clinical Pharmacology Prof: Mervat EidŇøurhąn ÂbòhašhəmNo ratings yet
- Methyl PrednisoloneDocument4 pagesMethyl PrednisoloneAnjar WijayadiNo ratings yet
- Recomendaciones para El Manejo de La Artritis Psoriásica Con Terapias FarmacológicasDocument13 pagesRecomendaciones para El Manejo de La Artritis Psoriásica Con Terapias FarmacológicasANDONIS30No ratings yet
- Dic 8 212595Document12 pagesDic 8 212595Dr-Kishna SenwarNo ratings yet
- Infusion Therapy: For Pain, Headache and Related ConditionsFrom EverandInfusion Therapy: For Pain, Headache and Related ConditionsAlaa Abd-ElsayedNo ratings yet
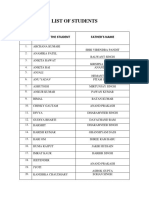
- List of Students GNM 1st (2020, 21)Document5 pagesList of Students GNM 1st (2020, 21)vaishali TMU studentNo ratings yet
- Prakash Institute of Physiotherapy Rehabilitation & Alllied Medical Sciences Master Rotation PlanDocument5 pagesPrakash Institute of Physiotherapy Rehabilitation & Alllied Medical Sciences Master Rotation Planvaishali TMU studentNo ratings yet
- Basicbscnursing 06 10 2018Document103 pagesBasicbscnursing 06 10 2018vaishali TMU studentNo ratings yet
- Breast Self ExaminationDocument24 pagesBreast Self Examinationvaishali TMU studentNo ratings yet
- B.Sc. Nursing Teerthanker Parshvnath School of NursingDocument2 pagesB.Sc. Nursing Teerthanker Parshvnath School of Nursingvaishali TMU studentNo ratings yet
- SRF No 0914400650930 Adhaar Card 7138 7999 7940Document1 pageSRF No 0914400650930 Adhaar Card 7138 7999 7940vaishali TMU studentNo ratings yet
- New Doc 2019-11-24 21.43.36Document1 pageNew Doc 2019-11-24 21.43.36vaishali TMU studentNo ratings yet
- Vaishali Singh Resume-1Document2 pagesVaishali Singh Resume-1vaishali TMU studentNo ratings yet
- Determiners GrammarDocument4 pagesDeterminers Grammarvaishali TMU studentNo ratings yet
- 51415tpnews 10312020Document60 pages51415tpnews 10312020vaishali TMU studentNo ratings yet
- Debate Grammar PDFDocument5 pagesDebate Grammar PDFvaishali TMU studentNo ratings yet
- Teerthanker Mahaveer University: Delhi Road, MoradabadDocument2 pagesTeerthanker Mahaveer University: Delhi Road, Moradabadvaishali TMU studentNo ratings yet
- Quality Control ManagementDocument4 pagesQuality Control Managementvaishali TMU studentNo ratings yet
- Joint Action For Mental Health Panel Discussion TopicDocument3 pagesJoint Action For Mental Health Panel Discussion Topicvaishali TMU studentNo ratings yet
- Calculations of Key Beneficiaries: Age Groups Percentage Formula Total Population in A Catchment Area of 5000Document2 pagesCalculations of Key Beneficiaries: Age Groups Percentage Formula Total Population in A Catchment Area of 5000vaishali TMU studentNo ratings yet
- School Healt ServicesDocument10 pagesSchool Healt Servicesvaishali TMU studentNo ratings yet
- Childhood ch-6 PoemDocument13 pagesChildhood ch-6 Poemvaishali TMU student100% (1)
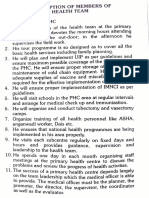
- Roles and Responsibilities of Various Health WorkersDocument7 pagesRoles and Responsibilities of Various Health Workersvaishali TMU studentNo ratings yet
- CounsellingDocument95 pagesCounsellingvaishali TMU studentNo ratings yet
- The 5 Ps of Vocal Impact in PresentationsDocument2 pagesThe 5 Ps of Vocal Impact in Presentationsvaishali TMU studentNo ratings yet
- Whooping CoughDocument9 pagesWhooping Coughvaishali TMU studentNo ratings yet
- Vaishali Evs ProjectDocument32 pagesVaishali Evs Projectvaishali TMU studentNo ratings yet
- The Five "W"S: The Keys To Planning An Effective PresentationDocument2 pagesThe Five "W"S: The Keys To Planning An Effective Presentationvaishali TMU studentNo ratings yet
- Email Writing: 1. Semi-Formal Email 2. Formal Email 3. Informal EmailDocument4 pagesEmail Writing: 1. Semi-Formal Email 2. Formal Email 3. Informal Emailvaishali TMU studentNo ratings yet
- TyphoidDocument11 pagesTyphoidvaishali TMU studentNo ratings yet