You might also like
- Taibah University Interns: Umm Al - Qura University SLE Questions 2 EditionDocument531 pagesTaibah University Interns: Umm Al - Qura University SLE Questions 2 EditionFammo MoiduNo ratings yet
- Medication - ALT-Template - Albuterol Sulfate PDFDocument1 pageMedication - ALT-Template - Albuterol Sulfate PDFNancyAmissah100% (1)
- Lanoxin (Digoxin)Document3 pagesLanoxin (Digoxin)E100% (5)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Aclindium Bromide PDFDocument15 pagesAclindium Bromide PDFddandan_2No ratings yet
- Adrenocortical AgentsDocument14 pagesAdrenocortical AgentsFredie O HadjimudinNo ratings yet
- Drug 25Document17 pagesDrug 25carol_gigliotti24100% (1)
- Antihistamine and DecongestantDocument22 pagesAntihistamine and DecongestantAngeline de GalaNo ratings yet
- Nursing Implicat: Ion: Indication: ActionDocument5 pagesNursing Implicat: Ion: Indication: ActionKrisTina KhaiZer RicoNo ratings yet
- DiphenhydramineDocument10 pagesDiphenhydramineFebry Dian SinagaNo ratings yet
- Medication - ALT-Template - AmlodipineDocument1 pageMedication - ALT-Template - AmlodipineNancyAmissahNo ratings yet
- Anemia CareplanDocument14 pagesAnemia Careplanbenardnyakundi99No ratings yet
- Adverse Drug Reaction JalpaDocument7 pagesAdverse Drug Reaction Jalpaparmar jalpabenNo ratings yet
- Intravenous Radiographic Contrast Induced Adverse Reactions - Their Causes, Prevention and Relief MeasuresDocument7 pagesIntravenous Radiographic Contrast Induced Adverse Reactions - Their Causes, Prevention and Relief MeasuresSri HariNo ratings yet
- Drug Study 7th Floor Ucmed RotationDocument6 pagesDrug Study 7th Floor Ucmed RotationVinz OñoNo ratings yet
- Drug Study QiDocument7 pagesDrug Study QiJeremiah Mauricio100% (1)
- Drug StudyDocument5 pagesDrug StudyNhadzmae Asmadul IsnainNo ratings yet
- DrugsDocument2 pagesDrugsgailannreyesNo ratings yet
- DrugsDocument2 pagesDrugsgailannreyesNo ratings yet
- Drug StudyDocument6 pagesDrug StudyArdrina SappariNo ratings yet
- Methylprednisolone (Solu-Medrol) : Emergency MedicationsDocument3 pagesMethylprednisolone (Solu-Medrol) : Emergency MedicationsKdamnzNo ratings yet
- MethylprednisoloneDocument4 pagesMethylprednisoloneadryananestesiNo ratings yet
- Anaphylactic ShockDocument9 pagesAnaphylactic Shockraghebhuda4No ratings yet
- ADR Notes KINJAL S. GAMITDocument13 pagesADR Notes KINJAL S. GAMITKinjal GamitNo ratings yet
- DIAGNOSIS AND MANAGEMENT OF ALLERGY-Dr - Dr.alvina Widhani, SpPD-KAIDocument24 pagesDIAGNOSIS AND MANAGEMENT OF ALLERGY-Dr - Dr.alvina Widhani, SpPD-KAIinhouseclinic grandhyattbaliNo ratings yet
- NalbuphineDocument5 pagesNalbuphineGab PagalilauanNo ratings yet
- ParacetamolDocument2 pagesParacetamolLegendXNo ratings yet
- Drug and NCPDocument15 pagesDrug and NCPgeelawlietNo ratings yet
- Drug Analysis 9Document6 pagesDrug Analysis 9Florante AnibanNo ratings yet
- Case Study For Advanced Pharmacotherapy: Clinical ApproachDocument4 pagesCase Study For Advanced Pharmacotherapy: Clinical ApproachAce AlbercaNo ratings yet
- HyrdrocortisoneDocument7 pagesHyrdrocortisoneRoseben SomidoNo ratings yet
- Anti Dementia Drugs: Moderator: Dr. Ramasubbareddy Sir Presenter: Dr. RavikishoreDocument26 pagesAnti Dementia Drugs: Moderator: Dr. Ramasubbareddy Sir Presenter: Dr. RavikishoreKishore SadulaNo ratings yet
- Adrenocortical AgentsDocument8 pagesAdrenocortical AgentsKarina Madriaga100% (1)
- Emergency DrugsDocument10 pagesEmergency DrugsRoland Mark Rodel LagosNo ratings yet
- 05 NCP - Drug StudyDocument23 pages05 NCP - Drug StudyRene John FranciscoNo ratings yet
- 1022 AngioedemaDocument24 pages1022 Angioedemabenitez1228No ratings yet
- Drug StudyDocument3 pagesDrug StudyGail SantosNo ratings yet
- NCMB317: RupturedDocument12 pagesNCMB317: RupturedArmand Bong Santiago100% (1)
- Adverse Drug ReactionsDocument41 pagesAdverse Drug ReactionsPopi Sopiah100% (1)
- Drug StudyDocument10 pagesDrug StudyBandana RajpootNo ratings yet
- Antihistamine Safety in Older Adult Dermatologic PatientsDocument6 pagesAntihistamine Safety in Older Adult Dermatologic PatientsHani Nur RahmawatiNo ratings yet
- 9 Drug StudyDocument11 pages9 Drug StudyJessa Mae Mauricio CastilloNo ratings yet
- Medical DrugsDocument11 pagesMedical DrugshassanyarbareachNo ratings yet
- Generic Name:: Name of The Drug Mechanism of Action Indication Contraindication Side Effects Nursing ResponsibilitiesDocument8 pagesGeneric Name:: Name of The Drug Mechanism of Action Indication Contraindication Side Effects Nursing ResponsibilitiesJennyLapitanNo ratings yet
- Product Name: New Zealand Data Sheet Apo-PrednisoneDocument13 pagesProduct Name: New Zealand Data Sheet Apo-PrednisonedomNo ratings yet
- DrugcardsDocument70 pagesDrugcards2liter100% (2)
- Adverse Drug ReactionDocument6 pagesAdverse Drug ReactionNunkoo RajNo ratings yet
- Client Profile Log Antenatal - CompleteDocument5 pagesClient Profile Log Antenatal - CompleteLinea GreeneNo ratings yet
- Bp1 Sgd1: TopicsDocument7 pagesBp1 Sgd1: TopicsAlan Joseph BaldovinoNo ratings yet
- E Kart DrugsDocument3 pagesE Kart DrugsNichole CastleNo ratings yet
- Ranitidine Tramadol Ketorolac Ampicillin Paracetamol Drug StudyDocument10 pagesRanitidine Tramadol Ketorolac Ampicillin Paracetamol Drug StudyMarco MoralesNo ratings yet
- Name of DrugDocument6 pagesName of Drug私 シャーロット100% (1)
- Pharmacogenomics Cases 1Document23 pagesPharmacogenomics Cases 1Pranita BhatNo ratings yet
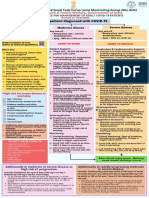
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
- Drug Ons: AdverseDocument5 pagesDrug Ons: AdverseMisty CheifNo ratings yet
- Covid19-Drug StudyDocument7 pagesCovid19-Drug StudynicoleNo ratings yet
- 1614978209sampleDocument9 pages1614978209sampleReddyNo ratings yet
- Common Antacid Medication-Ranitidine Causing A Rare Serious Adverse EffectDocument3 pagesCommon Antacid Medication-Ranitidine Causing A Rare Serious Adverse EffectL ANo ratings yet
- AzithromycinDocument10 pagesAzithromycinShaina MentangNo ratings yet
- Diagnosis & Management of Hypertension: Budi Susetyo PikirDocument51 pagesDiagnosis & Management of Hypertension: Budi Susetyo PikirFida Sonia Puspa EryantoNo ratings yet
- Family Medicine QuizletDocument28 pagesFamily Medicine QuizletNEsreNo ratings yet
- Separation and Quantification of Octahydro-1h-Indole-2-Carboxilic Acid and Its Three Isomers by HPLC Using Refractive Index DetectorDocument6 pagesSeparation and Quantification of Octahydro-1h-Indole-2-Carboxilic Acid and Its Three Isomers by HPLC Using Refractive Index DetectorSanthi KumarNo ratings yet
- Aan 204 Group Coursework: in Partial Fulfillment of The Requirements For The CourseDocument118 pagesAan 204 Group Coursework: in Partial Fulfillment of The Requirements For The CourseLucian CaelumNo ratings yet
- Dr. Esperanza Cabral ModuleDocument54 pagesDr. Esperanza Cabral ModuleNazarine TorresNo ratings yet
- Nephrology by Prof NegoDocument9 pagesNephrology by Prof NegoAbedinego MalukaNo ratings yet
- Ch-13 Drugs Used in Heart FailureDocument49 pagesCh-13 Drugs Used in Heart FailureShabrin SadikhNo ratings yet
- Heart FailureDocument41 pagesHeart FailureMatthew Jerome van HuizenNo ratings yet
- Shock CardiogenicoDocument28 pagesShock CardiogenicoIngrid Robledo100% (1)
- Case Study Hypertension 1Document11 pagesCase Study Hypertension 1Irwan 'Iw Iw' Setiawan100% (2)
- Causes and Evaluation of Hyperkalemia in AdultsDocument25 pagesCauses and Evaluation of Hyperkalemia in AdultsAnonymous iAoPnb2sNo ratings yet
- Pharmacological and Pharmaceutical Profile of Valsartan: A ReviewDocument8 pagesPharmacological and Pharmaceutical Profile of Valsartan: A ReviewWisnu Dwi AntaraNo ratings yet
- MOH, DHA and Some HAAD 2017: This Question Shared in Whatapp GroupDocument32 pagesMOH, DHA and Some HAAD 2017: This Question Shared in Whatapp GroupshahzadNo ratings yet
- Drugs Used in Cardiovascular SystemDocument57 pagesDrugs Used in Cardiovascular SystemSandeep ChaudharyNo ratings yet
- When To Restart Drugs Stopped During AKI FinalDocument2 pagesWhen To Restart Drugs Stopped During AKI FinalNoel QuintonNo ratings yet
- Pharmacology Questions CardiacDocument5 pagesPharmacology Questions CardiacAmanda SimpsonNo ratings yet
- Entres ToDocument21 pagesEntres ToJuanMarceloHelmerNo ratings yet
- Obat UperioDocument5 pagesObat UperioAnonymous Aa6VAStNo ratings yet
- Paragis C2Document9 pagesParagis C2Chitlet FrancheNo ratings yet
- List Signals Discussed Prac September 2012 - en Till 31-07-2023Document62 pagesList Signals Discussed Prac September 2012 - en Till 31-07-2023Amany HagageNo ratings yet
- Anti Hypertensive DrugsDocument40 pagesAnti Hypertensive DrugsjawadNo ratings yet
- 1 List Signals Discussed Prac September 2012 enDocument60 pages1 List Signals Discussed Prac September 2012 enAmany HagageNo ratings yet
- Sheffield Diabetes Resource PackDocument195 pagesSheffield Diabetes Resource Packhappyman1978No ratings yet
- HypertensionDocument54 pagesHypertensionBadri KarkiNo ratings yet
- RP-HPLC Method For The Simultaneous Estimation of Benazepril andDocument21 pagesRP-HPLC Method For The Simultaneous Estimation of Benazepril andPrtap Kumar PatraNo ratings yet
- Management of Hypertension in Heart Failure: Matthew R. Jonovich and John D. BisognanoDocument15 pagesManagement of Hypertension in Heart Failure: Matthew R. Jonovich and John D. BisognanojagodicamiliNo ratings yet
- Anemia 2020 - MNHU-PODINDocument32 pagesAnemia 2020 - MNHU-PODINwandaNo ratings yet
- Thesis HSF 2011 Moholisa RetsilisitsoeDocument121 pagesThesis HSF 2011 Moholisa RetsilisitsoeProudAfurakanNo ratings yet