You might also like
- Hearing Protection Safety TalkDocument13 pagesHearing Protection Safety Talkusmaniqbal15No ratings yet
- Language - NeuroDocument15 pagesLanguage - NeuroAifa Afeeqa Jamilan100% (1)
- Tplasty Cartilage Slides 080319 PDFDocument46 pagesTplasty Cartilage Slides 080319 PDFasiyazaidiaNo ratings yet
- Audiology Clinic HandbookDocument85 pagesAudiology Clinic HandbookNicoleta Letiția SchileruNo ratings yet
- Functional Correlations of Tympanic Membrane Perforation SizeDocument8 pagesFunctional Correlations of Tympanic Membrane Perforation SizeJose ManuelNo ratings yet
- Original Research Article: Amitkumar Rathi, Vinod Gite, Sameer Bhargava, Neeraj ShettyDocument8 pagesOriginal Research Article: Amitkumar Rathi, Vinod Gite, Sameer Bhargava, Neeraj ShettyAkanshaNo ratings yet
- IndianJOtol20110-1076076 025920Document6 pagesIndianJOtol20110-1076076 025920amalia primaNo ratings yet
- Evaluating Butterfly Inlay TympanoplastyDocument3 pagesEvaluating Butterfly Inlay Tympanoplastyarif sudiantoNo ratings yet
- Using Middle Ear Risk Index and ET Function As Parameters For Predicting The Outcome of TympanoplastyDocument4 pagesUsing Middle Ear Risk Index and ET Function As Parameters For Predicting The Outcome of TympanoplastysreshtamukhiNo ratings yet
- 1.fundagul Rapid Maxillary ExpansionDocument6 pages1.fundagul Rapid Maxillary ExpansionJoel TelloNo ratings yet
- Ultrasonic Determination of Gingival Thickness 1996Document8 pagesUltrasonic Determination of Gingival Thickness 1996João Carlos Bittencourt RibeiroNo ratings yet
- Systematic Review On Sucess of Narrow-Diameter Dental ImplantsDocument37 pagesSystematic Review On Sucess of Narrow-Diameter Dental ImplantsMaryGonzalesʚïɞNo ratings yet
- TM Perforation ArticleDocument3 pagesTM Perforation ArticleFaisal YousafNo ratings yet
- Jurnal Atresia KoanaDocument6 pagesJurnal Atresia KoanaArv IraNo ratings yet
- Ángulo Del Defecto Radiográfico Basal Del Defecto Intraóseo Como Indicador Pronóstico en Cirugía Periodontal Regenerativa Con Derivado de Matriz de EsmalteDocument5 pagesÁngulo Del Defecto Radiográfico Basal Del Defecto Intraóseo Como Indicador Pronóstico en Cirugía Periodontal Regenerativa Con Derivado de Matriz de EsmalteAgustin BuryakNo ratings yet
- Comparative Studies of Soft TissuesDocument9 pagesComparative Studies of Soft TissuesthieverNo ratings yet
- Tanya Jawab Membran TimpaniDocument3 pagesTanya Jawab Membran Timpanikayyis hawariNo ratings yet
- Efficacy of Tympanoplasty Without Mastoidectomy For Chronic Suppurative Otitis MediaDocument4 pagesEfficacy of Tympanoplasty Without Mastoidectomy For Chronic Suppurative Otitis Mediavikram123_us2002No ratings yet
- Minimally Invasive Surgical Technique and Enamel Matrix Derivative in Intra-Bony Defects. I - Clinical Outcomes and MorbidityDocument7 pagesMinimally Invasive Surgical Technique and Enamel Matrix Derivative in Intra-Bony Defects. I - Clinical Outcomes and MorbidityAnissa Citra UtamiNo ratings yet
- IndprewelaipdfDocument9 pagesIndprewelaipdfLimeysahni NazhoeNo ratings yet
- Hearing Research: Lingling Cai, Glenna Stomackin, Nicholas M. Perez, Xiaohui Lin, Timothy T. Jung, Wei DongDocument10 pagesHearing Research: Lingling Cai, Glenna Stomackin, Nicholas M. Perez, Xiaohui Lin, Timothy T. Jung, Wei DongJasmy FfNo ratings yet
- GMJ5201 0034 PDFDocument7 pagesGMJ5201 0034 PDFZha Zha Nurul ZahraNo ratings yet
- Medición Tomográfica de La EncíaDocument8 pagesMedición Tomográfica de La EncíaOlga Vasquez SotoNo ratings yet
- Correlation of Site and Size of Tympanic Membrane Perforation and Middle Ear Air Space Volume With Magnitude of Hearing LossDocument6 pagesCorrelation of Site and Size of Tympanic Membrane Perforation and Middle Ear Air Space Volume With Magnitude of Hearing LossYvetal GardeNo ratings yet
- Sutureless Tympanoplasty Using Acellular DermisDocument4 pagesSutureless Tympanoplasty Using Acellular DermissreshtamukhiNo ratings yet
- Mozzati2014 - Song Sieu Am Trong NH Răng 8Document4 pagesMozzati2014 - Song Sieu Am Trong NH Răng 8Hoàng VũNo ratings yet
- DownloadDocument7 pagesDownloadTaylor MillerNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument9 pagesInternational Journal of Pediatric OtorhinolaryngologyAcoet MiezarNo ratings yet
- Long-Term Effects of Rapid Maxillary Expansion Followed by Fixed AppliancesDocument5 pagesLong-Term Effects of Rapid Maxillary Expansion Followed by Fixed AppliancesFourthMolar.comNo ratings yet
- Apr 4Document10 pagesApr 4BimalKrishnaNo ratings yet
- Cone-Beam Computed Tomography Evaluation of Periodontal and Bone Support Loss in Extraction CasesDocument8 pagesCone-Beam Computed Tomography Evaluation of Periodontal and Bone Support Loss in Extraction CasesAlla MushkeyNo ratings yet
- Commonotologicsurgical Procedures: Clinical Decision-Making Pearls and The Role of ImagingDocument14 pagesCommonotologicsurgical Procedures: Clinical Decision-Making Pearls and The Role of ImagingyannecaNo ratings yet
- Assessment of Bone Dimensions in The Anterior Maxilla: A Cone Beam Computed Tomography StudyDocument8 pagesAssessment of Bone Dimensions in The Anterior Maxilla: A Cone Beam Computed Tomography Studylive your storyNo ratings yet
- Sener 2017Document9 pagesSener 2017Zachary DuongNo ratings yet
- Copy ProhibitedDocument7 pagesCopy ProhibitedMichael KronovNo ratings yet
- Application of Mouth Gag and Temporomandibular Joint Pain and Trismus in TonsillectomyDocument3 pagesApplication of Mouth Gag and Temporomandibular Joint Pain and Trismus in TonsillectomyMas YettyNo ratings yet
- Comparison of Temporal Bone ToDocument4 pagesComparison of Temporal Bone ToRais KhairuddinNo ratings yet
- Thetrigeminalnerve Injury: Arshad Kaleem,, Paul Amailuk,, Hisham Hatoum,, Ramzey TursunDocument13 pagesThetrigeminalnerve Injury: Arshad Kaleem,, Paul Amailuk,, Hisham Hatoum,, Ramzey TursunPriyanka SinhaNo ratings yet
- ContentDocument5 pagesContentOmniaNo ratings yet
- Miniscrew For Upper Incisor Intrusion EujoDocument5 pagesMiniscrew For Upper Incisor Intrusion EujoDevina YastaniNo ratings yet
- JOE - MorphologicalMeas - PulpOut BurDocument3 pagesJOE - MorphologicalMeas - PulpOut BurGabriela CiobanuNo ratings yet
- Alveolar Bone and Epithelial Attachment Status Following Two Different Closed-Eruption Surgical Techniques For Impacted Maxillary Central IncisorsDocument6 pagesAlveolar Bone and Epithelial Attachment Status Following Two Different Closed-Eruption Surgical Techniques For Impacted Maxillary Central IncisorsAndres CoboNo ratings yet
- Usd & MriDocument9 pagesUsd & MriJuhiJahan AmanullahNo ratings yet
- Positional Guidelines For Orthodontic Mini-Implant Placement in The Anterior Alveolar Region Systematic ReviewDocument10 pagesPositional Guidelines For Orthodontic Mini-Implant Placement in The Anterior Alveolar Region Systematic ReviewLarry MolinaNo ratings yet
- J Clinic Periodontology - 2015 - Yilmaz - Cone Beam Computed Tomography Evaluation of The Soft Tissue Thickness and GreaterDocument4 pagesJ Clinic Periodontology - 2015 - Yilmaz - Cone Beam Computed Tomography Evaluation of The Soft Tissue Thickness and GreaterjhynasindyNo ratings yet
- 2011 Coronectomy of The Lower Third Molar Is Safe Within The First 3 YearsDocument8 pages2011 Coronectomy of The Lower Third Molar Is Safe Within The First 3 YearskaarlaamendezNo ratings yet
- CBCT Article SandyDocument9 pagesCBCT Article Sandysandeep lachhwaniNo ratings yet
- Caninos RetenidosDocument9 pagesCaninos RetenidosNayely MiguelNo ratings yet
- Evaluation of Prognostic Factors and Middle Ear RiskDocument5 pagesEvaluation of Prognostic Factors and Middle Ear RiskKye Hoon ParkNo ratings yet
- JC 2 A RefDocument5 pagesJC 2 A RefHarish Kumar.THOTANo ratings yet
- Atm ArtDocument6 pagesAtm ArtYessyka EscalanteNo ratings yet
- Predetermination of Root Coverage: Journal of Periodontology March 2010Document9 pagesPredetermination of Root Coverage: Journal of Periodontology March 2010Zachary DuongNo ratings yet
- 10 1155@2017@3848207Document10 pages10 1155@2017@3848207hafidh akbarNo ratings yet
- Factors Of: Myringoplasty in Children: Predictive OutcomeDocument5 pagesFactors Of: Myringoplasty in Children: Predictive OutcomeAcoet MiezarNo ratings yet
- Pendahuluan: Down Mastoidectomy (CWD) - in CWU, Tympanic Cavity and Mastoid Cleared and Still MaintainDocument2 pagesPendahuluan: Down Mastoidectomy (CWD) - in CWU, Tympanic Cavity and Mastoid Cleared and Still MaintainichakhairNo ratings yet
- Study 2 Master Article s13005-015-0097-2Document5 pagesStudy 2 Master Article s13005-015-0097-2deepak sharmaNo ratings yet
- Profile Changes of Patients Treated With and Without Premolar ExtractionsDocument8 pagesProfile Changes of Patients Treated With and Without Premolar Extractionsblogger bloggerNo ratings yet
- Timpanoplastia Tipo IDocument14 pagesTimpanoplastia Tipo ILuis De jesus SolanoNo ratings yet
- Arthrocentesis A Minimally Invasive Method For TMJ Disc Disorders A Prospective StudyDocument4 pagesArthrocentesis A Minimally Invasive Method For TMJ Disc Disorders A Prospective StudyDavid NevesNo ratings yet
- Hearing Outcome After Type I Tympanoplasty: A Retrospective StudyDocument4 pagesHearing Outcome After Type I Tympanoplasty: A Retrospective Studyoperation_cloudburstNo ratings yet
- Computed Tomography-Guided Bone Block Harvesting From The Mandibular RamusDocument6 pagesComputed Tomography-Guided Bone Block Harvesting From The Mandibular Ramusfer francoNo ratings yet
- Practice-Based Clinical Evaluation of Zirconia PDFDocument12 pagesPractice-Based Clinical Evaluation of Zirconia PDFDiego Alejandro Cortés LinaresNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- Aural Toilet (Ear Cleaning) For Chronic Suppurative Otitis MediaDocument56 pagesAural Toilet (Ear Cleaning) For Chronic Suppurative Otitis MediaRuby KumarNo ratings yet
- Validity of An Illness Severity Measure For Headache in A Population Sample of Migraine SufferersDocument11 pagesValidity of An Illness Severity Measure For Headache in A Population Sample of Migraine SufferersRuby KumarNo ratings yet
- Mayoclinproc 84 5 007Document14 pagesMayoclinproc 84 5 007Ruby KumarNo ratings yet
- Ahmadieh 2007Document7 pagesAhmadieh 2007Ruby KumarNo ratings yet
- Chronic Suppurative Otitis Media CSOM EtiologicalDocument5 pagesChronic Suppurative Otitis Media CSOM EtiologicalRuby KumarNo ratings yet
- Hyaluronic Acid Fat Graft Myringoplasty: How We Do It: 610 CorrespondenceDocument5 pagesHyaluronic Acid Fat Graft Myringoplasty: How We Do It: 610 CorrespondenceRuby KumarNo ratings yet
- Ldnio y Xo Productos 4Document50 pagesLdnio y Xo Productos 4DAVID AVILANo ratings yet
- Hearing ProtectionDocument8 pagesHearing ProtectionteboviNo ratings yet
- ND50OSDocument2 pagesND50OSSaad ZiaNo ratings yet
- Noise PollutionDocument3 pagesNoise PollutionChie MendozaNo ratings yet
- Symptom Conductive Hearing Loss.3Document3 pagesSymptom Conductive Hearing Loss.3Muhammad Pringgo ArifiantoNo ratings yet
- Ent 03Document20 pagesEnt 03Sandra SNo ratings yet
- V 4 I 5 CognitiveDocument3 pagesV 4 I 5 CognitiveSusana Ruiz Losada BeainNo ratings yet
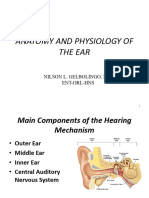
- Anatomy and Physiology of The EarDocument196 pagesAnatomy and Physiology of The EarChalsey Jene LorestoNo ratings yet
- Fitness and Health 2015Document6 pagesFitness and Health 2015cn_cadillacmiNo ratings yet
- Irwan Triansyah 87 95Document9 pagesIrwan Triansyah 87 95M. Ridho Bagus PratamaNo ratings yet
- Audiometer PaperforPGCON110519 FinalDocument6 pagesAudiometer PaperforPGCON110519 FinalAshok DhingraNo ratings yet
- Acoustic - Stapedius - Reflexes PDFDocument6 pagesAcoustic - Stapedius - Reflexes PDFSOFTMERCURYNo ratings yet
- Anatomy of The EarDocument24 pagesAnatomy of The EarVirya WijayatiNo ratings yet
- OtosclerosisDocument49 pagesOtosclerosisSaujanya SaravanakumarNo ratings yet
- Short Increment Sensitivity Index Test (SISI)Document2 pagesShort Increment Sensitivity Index Test (SISI)Anish RajNo ratings yet
- PHD Thesis Eth 29409 01Document4 pagesPHD Thesis Eth 29409 01iibtrihNo ratings yet
- The History of ASLDocument3 pagesThe History of ASLDonnette Davis100% (1)
- Grade 12 Life Science The Ear PDFDocument5 pagesGrade 12 Life Science The Ear PDFLethabo Mngomezulu100% (2)
- DDocument4 pagesDPraveenaslp EddulaNo ratings yet
- Auditory Nerve: Bavashika PrakashDocument14 pagesAuditory Nerve: Bavashika PrakashBavashiNo ratings yet
- Uswatun Hasanah-195037-2a Rmik (KKPMT)Document4 pagesUswatun Hasanah-195037-2a Rmik (KKPMT)Uswatun HasanahNo ratings yet
- Catálogo Otorrinolaringología 2023 3Document7 pagesCatálogo Otorrinolaringología 2023 3Erick ValdiviaNo ratings yet
- Procedure of Performing Ear IrrigationDocument17 pagesProcedure of Performing Ear Irrigationinoka sandamali AriyarathneNo ratings yet
- Science Milestone 2 Revision Worksheet - 1444701519118077954.SD - PDFDocument3 pagesScience Milestone 2 Revision Worksheet - 1444701519118077954.SD - PDFinfo.karunaentNo ratings yet
- TRANS 4 - Audiology 2021 Dr. DalandagDocument9 pagesTRANS 4 - Audiology 2021 Dr. DalandagNestle NgoNo ratings yet
- 4 PTA and TympanometryDocument22 pages4 PTA and TympanometryMariam QaisNo ratings yet
- Audiology & Hearing Aid Center - Tamilnadu - DatabaseDocument2 pagesAudiology & Hearing Aid Center - Tamilnadu - Databasekichu sNo ratings yet