You might also like
- Agent Source/Mot IP POC S/S Therapeutic MGMT Complications Nurisng ConsiderationsDocument13 pagesAgent Source/Mot IP POC S/S Therapeutic MGMT Complications Nurisng ConsiderationsKuennie SabalNo ratings yet
- Common Communicable DiseasesDocument13 pagesCommon Communicable DiseasesSanthosh.S.U100% (1)
- Scarlet FeverDocument4 pagesScarlet FeverLadyAnilin Regalado CorpuzNo ratings yet
- 4i4 (L@pq2b50ya1ku4Document16 pages4i4 (L@pq2b50ya1ku4Kristel AnneNo ratings yet
- Whooping CoughDocument72 pagesWhooping Coughwengie100% (1)
- MumpsDocument11 pagesMumpsamirahaliNo ratings yet
- Oxygenation ReviewerDocument8 pagesOxygenation ReviewerDamie FernandezNo ratings yet
- Polio: Bacteria Clostridium TetaniDocument6 pagesPolio: Bacteria Clostridium TetaniLovelyn Joy Abubo CortezNo ratings yet
- 6 Human Diseases That Cause by VirusesDocument7 pages6 Human Diseases That Cause by VirusesJefry JapNo ratings yet
- Systemic: Acne VulgarisDocument12 pagesSystemic: Acne VulgarisAnonymous DNoPgxTONo ratings yet
- MEASLES Case DiscussionDocument21 pagesMEASLES Case DiscussionjuiceNo ratings yet
- Rashes and FeversDocument36 pagesRashes and FeversLucykeshNo ratings yet
- NCM109 - Reviewer-Lp-1-To-Lp-4Document54 pagesNCM109 - Reviewer-Lp-1-To-Lp-4princessNo ratings yet
- Upper Respiratory Tract InfectionsDocument26 pagesUpper Respiratory Tract InfectionsZyrene RiveraNo ratings yet
- Common Disorde Rs in ChildrenDocument172 pagesCommon Disorde Rs in Childrenblacklilha100% (1)
- Common Health Problems of Infancy PowptDocument78 pagesCommon Health Problems of Infancy PowptCiella Dela CruzNo ratings yet
- Communicable DiseasesDocument7 pagesCommunicable DiseasesRaisa Robelle Quicho100% (1)
- Acute Upper Respiratory Tract InfectionsMB, BSDocument33 pagesAcute Upper Respiratory Tract InfectionsMB, BSibnbasheer83% (6)
- Nursing Care of A Child With Respiratory DisorderDocument69 pagesNursing Care of A Child With Respiratory DisorderTamil Villardo100% (1)
- UrticariaDocument12 pagesUrticariaMaka MegrelishviliNo ratings yet
- Measles: SynonymsDocument5 pagesMeasles: SynonymsAelora JullienneNo ratings yet
- Communicable Diseases CETRADocument22 pagesCommunicable Diseases CETRAACERET, IVAN LAURENTINE G.No ratings yet
- Care of Clients With Integumentary ProblemsDocument26 pagesCare of Clients With Integumentary ProblemsjeshemaNo ratings yet
- Kiara Denise Tamayo - MeaslesDocument3 pagesKiara Denise Tamayo - MeaslesKiara Denise TamayoNo ratings yet
- Respiratory Tract Infection Pharmacotherapy RevisedDocument82 pagesRespiratory Tract Infection Pharmacotherapy Revisedchuye alemayehuNo ratings yet
- Fever and Rash Mar 2016Document30 pagesFever and Rash Mar 2016almiraerickaiNo ratings yet
- Childhood Diseaases 21Document18 pagesChildhood Diseaases 21CHONANo ratings yet
- Report DraftDocument8 pagesReport DraftJeremel MalanumNo ratings yet
- M13 v2 Dermatology & STI - LO5Document6 pagesM13 v2 Dermatology & STI - LO5medipro clinicNo ratings yet
- MeaslesDocument17 pagesMeaslesFrances Rose Cabrera SalongaNo ratings yet
- Diseases in Children Word FileDocument12 pagesDiseases in Children Word FileLezrae Chescka Javier IlumbaNo ratings yet
- Viral Exanthems: Sahara Tuazan AbonawasDocument75 pagesViral Exanthems: Sahara Tuazan AbonawasMarlon Cenabre Turaja100% (1)
- Top 10Document3 pagesTop 10Raime Jean EntierroNo ratings yet
- Nursing Care of The Child With Respiratory DysfunctionDocument54 pagesNursing Care of The Child With Respiratory DysfunctionAlexis Coronado100% (1)
- NCM 102 (Pedia) Respi and GastroDocument252 pagesNCM 102 (Pedia) Respi and GastroMika Samson0% (1)
- Pediatric Viral ExanthemsDocument85 pagesPediatric Viral ExanthemsJohn Christopher LucesNo ratings yet
- Measles (Rubeola Morbilli 7 Days Fever)Document3 pagesMeasles (Rubeola Morbilli 7 Days Fever)Cedric BautistaNo ratings yet
- Nursing NotesDocument3 pagesNursing NotesMaria Clara IdaNo ratings yet
- IMCI Technical UpdatesDocument3 pagesIMCI Technical Updatesmikaela_pascuaNo ratings yet
- URTIDocument41 pagesURTIGetaneh LiknawNo ratings yet
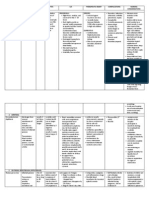
- Disease/Infection Etiologic Agent Incubatio N Period Rash Pattern/ Occurence Assoc. S/S TreatmentDocument10 pagesDisease/Infection Etiologic Agent Incubatio N Period Rash Pattern/ Occurence Assoc. S/S TreatmentmmmalcampoNo ratings yet
- Measles Management Guidelines - 091222-1Document14 pagesMeasles Management Guidelines - 091222-1Tushar AmbedareNo ratings yet
- 19 - VIRAL INFECTIONS - FinalDocument55 pages19 - VIRAL INFECTIONS - FinalMohammed GamalNo ratings yet
- Table of Communicable Diseases: Disease Signs & Symptoms Incubation Prevention Chicken PoxDocument10 pagesTable of Communicable Diseases: Disease Signs & Symptoms Incubation Prevention Chicken PoxKristel_Ramall_6985No ratings yet
- Mumps and Red Tide PoisoningDocument4 pagesMumps and Red Tide PoisoningBex LavurghNo ratings yet
- History of IllnessDocument1 pageHistory of IllnessFeyre LunaNo ratings yet
- Dermatology Videos by DR RihamDocument31 pagesDermatology Videos by DR Rihamengr_shazzNo ratings yet
- Health PoliciesDocument3 pagesHealth Policiesdongpc1No ratings yet
- Whooping Cough: Dr. MwendwaDocument39 pagesWhooping Cough: Dr. MwendwaAlvin OmondiNo ratings yet
- Communicable DiseasesDocument14 pagesCommunicable DiseasesGerald AlNo ratings yet
- Childhood Sicknesses1111Document17 pagesChildhood Sicknesses1111abdulrahmanbelewa96No ratings yet
- Prepared By: Ulfat Amin MSC Pediatric NursingDocument25 pagesPrepared By: Ulfat Amin MSC Pediatric NursingAngelic khanNo ratings yet
- Sinusitis in ChildDocument14 pagesSinusitis in ChildKin molikaNo ratings yet
- Upper RespiratoryDocument37 pagesUpper RespiratoryENKELI VALDECANTOSNo ratings yet
- Week 12 Learning ObjectivesDocument10 pagesWeek 12 Learning ObjectivesCamryn NewellNo ratings yet
- Acute Pharyngitis: MODULE 2A: Nursing Care To Patients With Problems in Oxygenation-VentilationDocument2 pagesAcute Pharyngitis: MODULE 2A: Nursing Care To Patients With Problems in Oxygenation-VentilationLalaine NadulpitNo ratings yet
- Common Cold Presentation - 2Document22 pagesCommon Cold Presentation - 2Muhammad naveedNo ratings yet
- L1tojl Ophcu) bq8fDocument31 pagesL1tojl Ophcu) bq8fKristel AnneNo ratings yet
- CN112B (Graded Discussion 3 - Evangelista, Allysa Joi M.)Document3 pagesCN112B (Graded Discussion 3 - Evangelista, Allysa Joi M.)Camille SanguyoNo ratings yet
- Anaphylaxis: A Practical GuideFrom EverandAnaphylaxis: A Practical GuideAnne K. EllisNo ratings yet
- Nursing Care Plan #1 Mental HealthDocument13 pagesNursing Care Plan #1 Mental HealthNursyNurseNo ratings yet
- Mental Status Assessment#2Document5 pagesMental Status Assessment#2NursyNurseNo ratings yet
- Online Connect Verbatim Report (Sample)Document5 pagesOnline Connect Verbatim Report (Sample)NursyNurseNo ratings yet
- Skin Pediatric NotesDocument8 pagesSkin Pediatric NotesNursyNurseNo ratings yet
- Verbatim 1Document10 pagesVerbatim 1NursyNurseNo ratings yet
- Dosage Calculation Review Part 2 - Medication DosagesDocument2 pagesDosage Calculation Review Part 2 - Medication DosagesNursyNurseNo ratings yet
- 3 Chapter 29 Practice Questions CardioDocument17 pages3 Chapter 29 Practice Questions CardioNursyNurseNo ratings yet
- Pedi Math Packet 2016-2017-1Document26 pagesPedi Math Packet 2016-2017-1NursyNurseNo ratings yet
- Dosage Calculation Review Part 3 - Flow Rate CalculationsDocument3 pagesDosage Calculation Review Part 3 - Flow Rate CalculationsNursyNurseNo ratings yet
- Dosage Titration PresentationDocument17 pagesDosage Titration PresentationNursyNurseNo ratings yet
- Dosage Calculation Review Part 1 - ConversionsDocument4 pagesDosage Calculation Review Part 1 - ConversionsNursyNurseNo ratings yet
- Dosage by Weight Exercises and AnswersDocument3 pagesDosage by Weight Exercises and AnswersNursyNurseNo ratings yet
- Common Subcutaneous Medications Check Off - Details - Kahoot!Document9 pagesCommon Subcutaneous Medications Check Off - Details - Kahoot!NursyNurseNo ratings yet
- Procedure Checklist Chapter 37, Skill 37-01: Reconstituting and Withdrawing Medication From A VialDocument2 pagesProcedure Checklist Chapter 37, Skill 37-01: Reconstituting and Withdrawing Medication From A VialNursyNurseNo ratings yet
- Procedure Checklist Chapter 26, Skill 26-04: Obtaining A Wound CultureDocument1 pageProcedure Checklist Chapter 26, Skill 26-04: Obtaining A Wound CultureNursyNurseNo ratings yet
- Antidiuretic Hormone: Manifestations of Dehydration-ElderlyDocument15 pagesAntidiuretic Hormone: Manifestations of Dehydration-ElderlyNursyNurseNo ratings yet
- Procedure Checklist Chapter 34, Skill 34-02: Performing VenipunctureDocument3 pagesProcedure Checklist Chapter 34, Skill 34-02: Performing VenipunctureNursyNurseNo ratings yet
- Exam 1 Slides APDocument13 pagesExam 1 Slides APNursyNurseNo ratings yet
- Procedure Checklist Chapter 38, Skill 38-01: Administering IV Medication Via PRN Lock or IV LineDocument2 pagesProcedure Checklist Chapter 38, Skill 38-01: Administering IV Medication Via PRN Lock or IV LineNursyNurseNo ratings yet
- BNS Exam 4 2021 - Details - Kahoot!Document6 pagesBNS Exam 4 2021 - Details - Kahoot!NursyNurseNo ratings yet
- BNS Exam 4 CH 31 Book Review Questions, Questions Taken From Key Points, and Within Book - Details - Kahoot!Document32 pagesBNS Exam 4 CH 31 Book Review Questions, Questions Taken From Key Points, and Within Book - Details - Kahoot!NursyNurseNo ratings yet
- BNS Insulins & Other Meds We Covered - Details - Kahoot!Document22 pagesBNS Insulins & Other Meds We Covered - Details - Kahoot!NursyNurseNo ratings yet
- Important Slides Nutrition ch5Document18 pagesImportant Slides Nutrition ch5NursyNurseNo ratings yet
- Sensititre Plate Guide Booklet EN PDFDocument62 pagesSensititre Plate Guide Booklet EN PDFXuân Tài NguyễnNo ratings yet
- Pressure Sore: GradingDocument2 pagesPressure Sore: GradingAnusha VergheseNo ratings yet
- 3 - Physical Examination of UrineDocument6 pages3 - Physical Examination of UrineKunware TropaNo ratings yet
- 22 February 2022 Academic Reading TestDocument17 pages22 February 2022 Academic Reading TestMin MaxNo ratings yet
- BPC-157 - Scientific Review On Usage, Dosage, Side Effects - ExamineDocument10 pagesBPC-157 - Scientific Review On Usage, Dosage, Side Effects - Examineozman blooriNo ratings yet
- ACUTE STRESS DISORDER and POSTTRAUMATIC STRESS DISORDERDocument16 pagesACUTE STRESS DISORDER and POSTTRAUMATIC STRESS DISORDERumibrahimNo ratings yet
- 9375 X PER3 Therapy Lamp ManualDocument26 pages9375 X PER3 Therapy Lamp ManualAmicus79No ratings yet
- Family Planning (Teaching Plan) Ana AlcasabasDocument6 pagesFamily Planning (Teaching Plan) Ana Alcasabasiammerbinpransisko75% (4)
- EpidemiologiDocument7 pagesEpidemiologiazzaNo ratings yet
- Ch14 3Document4 pagesCh14 3hervatt50% (2)
- Lhea's Case StudyDocument14 pagesLhea's Case StudyMelody B. MiguelNo ratings yet
- M G University M.SC Applied Microbiology SyllabusDocument52 pagesM G University M.SC Applied Microbiology SyllabusHermann AtangaNo ratings yet
- ParanoiaDocument16 pagesParanoiathe SkulptorNo ratings yet
- Unilag MSC FINANCE Past Questions PDFDocument2 pagesUnilag MSC FINANCE Past Questions PDFbdianNo ratings yet
- Distinct Spectrum of CFTR Gene MutationsDocument13 pagesDistinct Spectrum of CFTR Gene Mutationsapi-3742014No ratings yet
- Rds CaseDocument42 pagesRds Casegebby puspitaNo ratings yet
- NCM 3114 Acid Base Imbalance-2Document13 pagesNCM 3114 Acid Base Imbalance-2Fayeh Harah PadrillanNo ratings yet
- Effect of Organic Manure On Growth and Yield of Strawberry: January 2014Document5 pagesEffect of Organic Manure On Growth and Yield of Strawberry: January 2014LekhonVlogsNo ratings yet
- DNA Replication Study Guide - Biology101Document4 pagesDNA Replication Study Guide - Biology101nandi_scrNo ratings yet
- Toxic and Safe Plants PDFDocument31 pagesToxic and Safe Plants PDFAbad Masoud KittaniNo ratings yet
- Ho Lester OlllDocument6 pagesHo Lester OlllVlad VladNo ratings yet
- III Bds II Internal 2023Document5 pagesIII Bds II Internal 2023Sourab KumarNo ratings yet
- Prolapsed Intervertebral Disc: By: Diksha Solanki Bot 4 YearDocument37 pagesProlapsed Intervertebral Disc: By: Diksha Solanki Bot 4 YearISIC IRS100% (1)
- Hemophilia and Its Treatment: Brief ReviewDocument7 pagesHemophilia and Its Treatment: Brief ReviewSalsa BillaNo ratings yet
- The Conditions of The Small-Scale Miners in Barangay Bukal, Nabunturan Compostela Valley ProvinceDocument24 pagesThe Conditions of The Small-Scale Miners in Barangay Bukal, Nabunturan Compostela Valley Provincexenos19No ratings yet
- Study Guide 1 Case Studies 1 and 2 Gutierrez, W.Document3 pagesStudy Guide 1 Case Studies 1 and 2 Gutierrez, W.Winell Gutierrez100% (1)
- Acute Asthma Paed WaniDocument16 pagesAcute Asthma Paed WaniNurul Syazwani RamliNo ratings yet
- Surgical Treatment For Mammary TumorsDocument5 pagesSurgical Treatment For Mammary Tumorsgrace joNo ratings yet
- Acute-Phase ProteinDocument17 pagesAcute-Phase ProteinAbhijith S. PNo ratings yet
- The Central Nervous SystemDocument7 pagesThe Central Nervous Systemjoeywap29No ratings yet