You might also like
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- NURSING CARE OF ADULTS I: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS I: Passbooks Study GuideNo ratings yet
- Nursing Diagnosis List for Basic Human NeedsDocument28 pagesNursing Diagnosis List for Basic Human NeedsAmit MartinNo ratings yet
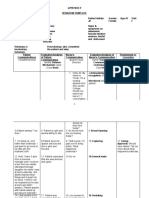
- Nursing Diagnosis TemplateDocument6 pagesNursing Diagnosis Templatesdk6972No ratings yet
- Head, Mouth, Nose, Throat, Neck and Regional Lymph Nodes: Kristin Clephane, MSN, RN, CPNDocument44 pagesHead, Mouth, Nose, Throat, Neck and Regional Lymph Nodes: Kristin Clephane, MSN, RN, CPNMike100% (1)
- What To Know On The Exam: Mania - 7 QuestionsDocument11 pagesWhat To Know On The Exam: Mania - 7 QuestionsNyein Nu WinnNo ratings yet
- ETOH Case StudyDocument5 pagesETOH Case StudyCharme Jean RaygonNo ratings yet
- Bipolar Depression/Mania: SKINNY ReasoningDocument9 pagesBipolar Depression/Mania: SKINNY ReasoningSharon TanveerNo ratings yet
- Part I: Emergency Department (ED) : SKINNY ReasoningDocument6 pagesPart I: Emergency Department (ED) : SKINNY ReasoningUzumaki KNo ratings yet
- Week 4 - The Nursing ProcessDocument10 pagesWeek 4 - The Nursing ProcessMiss VinaNo ratings yet
- Nursing ProcessDocument12 pagesNursing Processgrey26No ratings yet
- Nursing Interview Guide To Collect Subjective Data From The Client Questions RationaleDocument19 pagesNursing Interview Guide To Collect Subjective Data From The Client Questions RationaleKent Rebong100% (1)
- EvalDocument3 pagesEvalapi-433857993No ratings yet
- IVY TECH NURSING LAB INFORMATIONDocument7 pagesIVY TECH NURSING LAB INFORMATIONSethNo ratings yet
- Clinical Replacement Student PacketDocument12 pagesClinical Replacement Student PacketLivan MartellNo ratings yet
- Examine the EyeDocument12 pagesExamine the EyeiuytrerNo ratings yet
- Neurologic Assessment Physiologic Changes With AgingDocument4 pagesNeurologic Assessment Physiologic Changes With AgingDarl Dacdac100% (1)
- Bsn-Rs-Careplan 2Document9 pagesBsn-Rs-Careplan 2api-520841770No ratings yet
- ATI Medication Template RanitidineDocument1 pageATI Medication Template RanitidineSharee HaywoodNo ratings yet
- Ati Medication Template VasopressinDocument1 pageAti Medication Template VasopressinSharee HaywoodNo ratings yet
- Nursing Concept MapDocument2 pagesNursing Concept MapMary MannNo ratings yet
- Psychotropic Medication Roles and Nursing ProcessDocument9 pagesPsychotropic Medication Roles and Nursing ProcessGina GiammalvoNo ratings yet
- Mental Capital SummaryDocument52 pagesMental Capital SummaryaguzzzNo ratings yet
- Chapter 22 - Transition To ParenthoodDocument16 pagesChapter 22 - Transition To ParenthoodJill HillNo ratings yet
- Pediatric Case 4: Sabina Vasquez (Complex) : Documentation AssignmentsDocument1 pagePediatric Case 4: Sabina Vasquez (Complex) : Documentation AssignmentsRose Nirwana Handayani0% (1)
- Ati Medication Template CodeineDocument1 pageAti Medication Template CodeineSharee HaywoodNo ratings yet
- Acute Myocardial Infarction (AMI) Signs, Diagnosis, TreatmentDocument10 pagesAcute Myocardial Infarction (AMI) Signs, Diagnosis, TreatmentBianca Watanabe - RatillaNo ratings yet
- MH NotesDocument28 pagesMH NotesNyein Nu Winn100% (2)
- Thinking Like A NurseDocument3 pagesThinking Like A Nurseapi-519359726No ratings yet
- Ati Medication Template KetorolacDocument1 pageAti Medication Template KetorolacSharee HaywoodNo ratings yet
- Ch35 CardiovascularDocument11 pagesCh35 CardiovascularJessie Jennings100% (3)
- Learning Plans EportfolioDocument2 pagesLearning Plans Eportfolioapi-345810410No ratings yet
- Sena, Zyrus Reoder ADocument4 pagesSena, Zyrus Reoder AAkoSiIngridNo ratings yet
- Care of Older Adult Full Notes For Next Weeks QuizDocument14 pagesCare of Older Adult Full Notes For Next Weeks QuizMercy Anne EcatNo ratings yet
- Reflective Journal Med Surg Clinical April 14thDocument3 pagesReflective Journal Med Surg Clinical April 14thapi-238869728No ratings yet
- Draft: Jurisprudence Learning Module & ExaminationDocument45 pagesDraft: Jurisprudence Learning Module & ExaminationDeepanshi RajputNo ratings yet
- Problem/PICOT/Evidence Search (PPE) Worksheet: Chamberlain College of NursingDocument3 pagesProblem/PICOT/Evidence Search (PPE) Worksheet: Chamberlain College of NursingWeke-sir CollinsNo ratings yet
- Nurse Sam Nursing School Study Kits, Courses, and Merch! - The Nurse SamDocument6 pagesNurse Sam Nursing School Study Kits, Courses, and Merch! - The Nurse SamRrg0% (1)
- Nursing Care for Loss, Grief and DeathDocument4 pagesNursing Care for Loss, Grief and DeathNina Anne ParacadNo ratings yet
- Completed Concept MapDocument4 pagesCompleted Concept Mapapi-607361848No ratings yet
- Nursing Care Plan For Subarachnoid HemorrhagicDocument2 pagesNursing Care Plan For Subarachnoid HemorrhagicAshram Smart100% (1)
- Nursing Process Overview: Health Assessment NotesDocument40 pagesNursing Process Overview: Health Assessment NotesEliakim III InsongNo ratings yet
- NURS 4369 Preceptor Packet Core 2013Document11 pagesNURS 4369 Preceptor Packet Core 2013Aruna Chezhian100% (1)
- Chapter 3 Module The Therapeutic Nurse-Patient RelationshipDocument2 pagesChapter 3 Module The Therapeutic Nurse-Patient RelationshipJaylord VerazonNo ratings yet
- Health Assessment Term 3Document3 pagesHealth Assessment Term 3api-254275284No ratings yet
- LPN EditedDocument5 pagesLPN EditedMoses MwangiNo ratings yet
- Ati Medication Template HydrocortisoneDocument1 pageAti Medication Template HydrocortisoneSharee HaywoodNo ratings yet
- Medsurg 2007Document15 pagesMedsurg 2007WisdomIsMisery100% (1)
- Ineffective Coping - Nursing Diagnosis & Care Plan - NurseslabsDocument13 pagesIneffective Coping - Nursing Diagnosis & Care Plan - NurseslabsLester MooreNo ratings yet
- Mental Health - PsychopharmacologyDocument4 pagesMental Health - PsychopharmacologyRenetria DrakeNo ratings yet
- Managing Diabetes Sick DaysDocument14 pagesManaging Diabetes Sick DaysJake Yvan DizonNo ratings yet
- NFDN 2005 Professional PortfolioDocument2 pagesNFDN 2005 Professional PortfolioTiffany MartellsNo ratings yet
- Acetaminophen PDFDocument1 pageAcetaminophen PDFmp1757No ratings yet
- Lowdermilk: Maternity & Women's Health Care, 10th EditionDocument12 pagesLowdermilk: Maternity & Women's Health Care, 10th Editionvanassa johnson100% (1)
- Metoprolol Teaching PlanDocument18 pagesMetoprolol Teaching Planapi-419091662No ratings yet
- Most Question That The "Psychiatrist" Would Ask?Document1 pageMost Question That The "Psychiatrist" Would Ask?Chayantorn NimmanwathanaNo ratings yet
- Nursing AssessmentDocument16 pagesNursing AssessmentJihan Novita100% (1)
- Cardiovascular ADocument3 pagesCardiovascular AAutumn AllisonNo ratings yet
- Life and DeathDocument23 pagesLife and DeathJea Joel MendozaNo ratings yet
- 3 Cerebral Dysfunction Practice QuestionsDocument13 pages3 Cerebral Dysfunction Practice QuestionsNursyNurseNo ratings yet
- Mental Status Assessment#2Document5 pagesMental Status Assessment#2NursyNurseNo ratings yet
- Online Connect Verbatim Report (Sample)Document5 pagesOnline Connect Verbatim Report (Sample)NursyNurseNo ratings yet
- Test1PPT Chapter 01Document33 pagesTest1PPT Chapter 01Sandra brownNo ratings yet
- 3 Chapter 29 Practice Questions CardioDocument17 pages3 Chapter 29 Practice Questions CardioNursyNurseNo ratings yet
- 3 Communicable Diseases NotesDocument3 pages3 Communicable Diseases NotesNursyNurseNo ratings yet
- Dosage Calculation Review Part 1 - ConversionsDocument4 pagesDosage Calculation Review Part 1 - ConversionsNursyNurseNo ratings yet
- Dosage Calculation Review Part 2 - Medication DosagesDocument2 pagesDosage Calculation Review Part 2 - Medication DosagesNursyNurseNo ratings yet
- Verbatim 1Document10 pagesVerbatim 1NursyNurseNo ratings yet
- Dosage Titration PresentationDocument17 pagesDosage Titration PresentationNursyNurseNo ratings yet
- Dosage Calculation Review Part 4 - TitrationsDocument6 pagesDosage Calculation Review Part 4 - TitrationsNursyNurseNo ratings yet
- Skin Pediatric NotesDocument8 pagesSkin Pediatric NotesNursyNurseNo ratings yet
- Pedi Dosage Calculation ConceptsDocument3 pagesPedi Dosage Calculation ConceptsNursyNurseNo ratings yet
- Dosage Calculation Review Part 3 - Flow Rate CalculationsDocument3 pagesDosage Calculation Review Part 3 - Flow Rate CalculationsNursyNurseNo ratings yet
- Dosage by Weight Exercises and AnswersDocument3 pagesDosage by Weight Exercises and AnswersNursyNurseNo ratings yet
- Antidiuretic Hormone: Manifestations of Dehydration-ElderlyDocument15 pagesAntidiuretic Hormone: Manifestations of Dehydration-ElderlyNursyNurseNo ratings yet
- Procedure Checklist Chapter 30, Skill 30-02: Obtaining A Stool Specimen For Culture, and Ova and ParasitesDocument1 pageProcedure Checklist Chapter 30, Skill 30-02: Obtaining A Stool Specimen For Culture, and Ova and ParasitesNursyNurseNo ratings yet
- Pedi Math Packet 2016-2017-1Document26 pagesPedi Math Packet 2016-2017-1NursyNurseNo ratings yet
- Procedure Checklist Chapter 22, Skill 22-01: Setting Up A Sterile Field, Opening Sterile Packs, and Pouring Sterile LiquidsDocument1 pageProcedure Checklist Chapter 22, Skill 22-01: Setting Up A Sterile Field, Opening Sterile Packs, and Pouring Sterile LiquidsNursyNurseNo ratings yet
- Procedure Checklist Chapter 26, Skill 26-07: Changing A Negative Pressure Wound Therapy Dressing (Wound VAC)Document2 pagesProcedure Checklist Chapter 26, Skill 26-07: Changing A Negative Pressure Wound Therapy Dressing (Wound VAC)NursyNurseNo ratings yet
- Safe Dosage Calculation For Pediatric Patients QuizDocument2 pagesSafe Dosage Calculation For Pediatric Patients QuizNursyNurseNo ratings yet
- Procedure Checklist Chapter 31, Skill 31-06: Obtaining A Urine Specimen From An Indwelling CatheterDocument1 pageProcedure Checklist Chapter 31, Skill 31-06: Obtaining A Urine Specimen From An Indwelling CatheterNursyNurseNo ratings yet
- Procedure Checklist Chapter 28, Skill 28-01: Obtaining A Sputum SpecimenDocument1 pageProcedure Checklist Chapter 28, Skill 28-01: Obtaining A Sputum SpecimenNursyNurseNo ratings yet
- Procedure Checklist Chapter 28, Skill 28-09: Maintaining Chest TubesDocument2 pagesProcedure Checklist Chapter 28, Skill 28-09: Maintaining Chest TubesNursyNurseNo ratings yet
- Procedure Checklist Chapter 38, Skill 38-01: Administering IV Medication Via PRN Lock or IV LineDocument2 pagesProcedure Checklist Chapter 38, Skill 38-01: Administering IV Medication Via PRN Lock or IV LineNursyNurseNo ratings yet
- Procedure Checklist Chapter 31, Skill 31-08: Performing Continuous Bladder IrrigationDocument1 pageProcedure Checklist Chapter 31, Skill 31-08: Performing Continuous Bladder IrrigationNursyNurseNo ratings yet
- Procedure Checklist Chapter 26, Skill 26-04: Obtaining A Wound CultureDocument1 pageProcedure Checklist Chapter 26, Skill 26-04: Obtaining A Wound CultureNursyNurseNo ratings yet
- Procedure Checklist Chapter 34, Skill 34-02: Performing VenipunctureDocument3 pagesProcedure Checklist Chapter 34, Skill 34-02: Performing VenipunctureNursyNurseNo ratings yet
- Procedures Checklist Chapter 37, Skill 37-04: Combining and Administering Insulin SubcutaneouslyDocument2 pagesProcedures Checklist Chapter 37, Skill 37-04: Combining and Administering Insulin SubcutaneouslyNursyNurseNo ratings yet
- The Prevention and Management of Violence (2nd Edition)Document414 pagesThe Prevention and Management of Violence (2nd Edition)OmarNo ratings yet
- Goffman's Theory of Stigmatization and Its Impact on HealthDocument10 pagesGoffman's Theory of Stigmatization and Its Impact on HealthNaomi100% (1)
- Upd - IDocument12 pagesUpd - INandini MajumdarNo ratings yet
- Identifying Anxiety-Igniting Thoughts PDFDocument11 pagesIdentifying Anxiety-Igniting Thoughts PDFmizbigspendaNo ratings yet
- Licensing Exam Practice QuestionsDocument5 pagesLicensing Exam Practice QuestionsSabahat KanwalNo ratings yet
- Two Factor Theory of LearningDocument6 pagesTwo Factor Theory of LearningJose DavidNo ratings yet
- America 2022 in Charts: An Economic Opportunity Snapshot: December 2021Document11 pagesAmerica 2022 in Charts: An Economic Opportunity Snapshot: December 2021Corival Alves Do CarmoNo ratings yet
- Bipolar Disorder Case StudyDocument14 pagesBipolar Disorder Case StudyValiant Baybay67% (3)
- Articel About Mental HealthDocument10 pagesArticel About Mental HealthDimas Febriansyah MuhsinNo ratings yet
- Garratt PaperDocument17 pagesGarratt PaperCarla HortaNo ratings yet
- Low Self Esteem: A Map of The Territory: Early ExperienceDocument1 pageLow Self Esteem: A Map of The Territory: Early ExperiencenoradeenNo ratings yet
- Distress Tolerance Worksheet PDFDocument5 pagesDistress Tolerance Worksheet PDFUnoduetre Stella50% (2)
- 468 U N I T 4: Nursing Care of Clients With Alterations in Psychosocial AdaptationDocument1 page468 U N I T 4: Nursing Care of Clients With Alterations in Psychosocial AdaptationMercy JacobNo ratings yet
- Coping With Grief and LossDocument5 pagesCoping With Grief and LossIoan DraghiciNo ratings yet
- Facing Homelessness: A Study of Homelessness in Chicago and The SuburbsDocument11 pagesFacing Homelessness: A Study of Homelessness in Chicago and The SuburbsSocial IMPACT Research Center at Heartland Alliance for Human Needs and Human RightsNo ratings yet
- Crim 3 Lesson 2Document4 pagesCrim 3 Lesson 2JEAH REDOBLE100% (1)
- Research Dossier Final DraftDocument7 pagesResearch Dossier Final Draftapi-579839747No ratings yet
- Self Hypnosis Course, Lesson 1-7 T.wattSDocument16 pagesSelf Hypnosis Course, Lesson 1-7 T.wattSNiky Giaccio100% (3)
- Essay 5Document13 pagesEssay 5api-549025764No ratings yet
- Autism: Asperger Syndrome The Prevalence of Anxiety and Mood Problems Among Children With Autism andDocument17 pagesAutism: Asperger Syndrome The Prevalence of Anxiety and Mood Problems Among Children With Autism andDiana Petronela AbabeiNo ratings yet
- Case Pres-Banag Laum SuperfinaleDocument46 pagesCase Pres-Banag Laum SuperfinaleAyen FornollesNo ratings yet
- Conquering Anger: Problem We Can Work Through Together? What Do You Think Would Happen If The TablesDocument1 pageConquering Anger: Problem We Can Work Through Together? What Do You Think Would Happen If The TablesNiel PetersNo ratings yet
- Important Ted Barber On HypnosisDocument5 pagesImportant Ted Barber On HypnosisblackharmonicaNo ratings yet
- Child Mental Health Dissertation IdeasDocument4 pagesChild Mental Health Dissertation IdeasPaySomeoneToWriteYourPaperSingapore100% (1)
- 2017 - Scielo Cie 11Document9 pages2017 - Scielo Cie 11MarysabelNo ratings yet
- MN - 2019 08 20Document24 pagesMN - 2019 08 20mooraboolNo ratings yet
- Module 1 of CA2: Non-Institutional CorrectionDocument8 pagesModule 1 of CA2: Non-Institutional CorrectionMut4nt TVNo ratings yet
- Antisocial and Borderline Personality Traits and Childhood TraumaDocument10 pagesAntisocial and Borderline Personality Traits and Childhood TraumaTara aNo ratings yet
- Major Psychological InterventionsDocument230 pagesMajor Psychological InterventionsJules Exequiel Pescante Suico100% (2)
- SBAR - Major DepressionDocument3 pagesSBAR - Major DepressionTonya PhelpsNo ratings yet