Alternative Thinking about Business and Technology
HP/Crossflo Health Information Solution webinar Q&A
Recently, HP and Crossflo Systems held a webinar to introduce the HP/Crossflo Health Information Solution. Attendee interest was high, and many questions were posed and answered. Following are some of those questions and their respective answers.
A2) It is true that incurring variable costs creates revenue, but only to a point. It is equally true that when physicians create excessive variable costs by ordering excessive tests and treatments for their patients that creates losses for the hospital. The question then becomes, what are excessive Q) If a practice is interested in virtually integrating and appropriate resource consumptions and with the hospital, how would an independent office who determines the differences. In general go about requesting this initiative with the hospital? terms, hospital administrators control the charges for all inpatient tests and treatments (variable A) A single-office virtual integration with the hospital costs), but only physicians control the number of would be problematic as you would not be able tests and treatments that are deployed for each to move patients records to your colleagues. I patient. Most hospital administrators have already would try to find other like-minded physicians removed excess full time equivalents (fixed and approach the hospital with the request. Most costs) from their staffs, maintaining the minimum physicians who wish to form a Virtual Medical personnel necessary to deliver the number of tests Group with their hospital are associated in and treatments ordered by physicians. some type of IPA or medical staff with common goals. The practical reality is that the costs of On the reimbursement side, hospital the integrated hardware and software necessary administrators have even less control. The majority for exchanging patients records between offices of hospitalized patients are reimbursed under and the hospital are sufficiently large that the DRGs or some form of predetermined dollars hospital would want to see many physicians for treating each patient. Indigent patients are involved in the initiative. That being said, the reimbursed at $0.00, Medicaid somewhat hospitals and physicians who understand the more and Medicare even more, but still often significant improvements in medical quality and inadequate. The remaining patients are insured patient satisfaction that accrue from such a project in various ways. Several years ago, these insured will recoup their costs many times over by the patients were the best reimbursed patients. But physicians engaging with the hospital in clinical gone are the days when creating higher patient quality improvement activities. charges to insurance companies yield greater net income because the reimbursements for insured Q) Can we contact the physician that is speaking? cases are basically predetermined as well. A) Yes, Bill Mohlenbrock can be contacted at 858.724.2216 ext 246 or bmohlenbrock@crossflo.com. Q1) How do we determine severity in our data systems? Q2) How are the cost savings calculated? Fixed cost is sunk, so without incurring variable cost theres no revenue created or cost avoided. A1) The data used to calculate inpatient severity are those contained in the hospitals medical records database [The Uniform Hospital Discharge Data Set (UHDDS)]. These data are routinely gathered on each patient at the time of discharge therefore, no data needs to be manually abstracted. To calculate each patients severity levels requires the hospital to contract with an outside service, such as Iameter or 3M. Iameter uses the Acuity Index Method, which sub-divides the MS-DRGs into 5 levels of acuity and is the acuity method one demonstrated during the webcast. 3M subdivides its own proprietary DRG system, the All Payer Refined DRGs (APR-DRGs). Either severity system is acceptable for use as the basis of physiciandirected, clinical quality improvement initiatives. For these reasons, hospital administrations are now asking themselves how they can assist their physicians in the control of variable costs. When the administration supports physicians with clinical quality improvement initiatives, the hospital prospers. The goal of quality improvement is to decrease morbidities and reduce variations in resource consumption to only those tests, treatments and hospital days that the physicians, NOT the insurance companies, determine to be appropriate. The premise of physician-directed, clinical quality improvement is that good doctors, given good clinical data will modify their practices to improve quality and efficiencies. As physicians identify those tests and treatments that have historically given their patients the highest quality and most efficient outcomes, they significantly reduce the deployment of variable costs. Over time, these reductions will make it possible for the administration to manage their staffing levels to reduce fixed costs as well. In short, if the physicians are provided the tools to determine which processes and resources objectively produced the best outcomes of mortality, morbidity, shorter LOS and fewer charges, and they deploy these processes through clinical pathways, the hospital will lose fewer dollars or even make money on each case.
Given the tremendous variations in quality and costs between hospitals within the same community or geographic region, healthcare purchasers (businesses and patients) are seeking to reward those hospitals and their medical staffs who are willing to demonstrate the value (quality and price) of their medical care. Q) Any idea/suggestion on how to get physicians to overcome the barrier of participating & submitting quality data for the CMS initiatives? A) Yes, there are a couple of very powerful incentives for your physicians to consider as they contemplate their assisting the hospital with CMS quality initiatives. For the first time in Medicares history, hospitals and physicians individual quality outcomes are both determined by data contained in each hospitals Medicare claims database. Hospitals are now being reimbursed more for improved quality and economically punished for poor quality, by CMS not paying for specific complications and by having CMS dollars recovered by arbitrary decisions through RACs. Physicians have no similar, direct economic ties to qualityyet. However, they now have quality ties to the hospitals claims database because in 2007 a federal judge ruled that physicians names and their quality outcomes can be published in public news outlets. Many cardiac surgeons have realized this, too late, when their names appeared in their local papers as having unacceptably high mortality rates. Physicians who understand these issues will assist the hospital in making the hospitals medical records and CMS National Hospital Quality Measures (NHQM) databases as accurate and robust as possible. I spend a significant amount of time discussing these issues with physicians because the message is often easier for a physician from outside the hospital to deliver than someone from the medical staff or administration. Q) Your framework seems tightly related to case management approaches, but you seem not to focus on single patients, what is your business model?
A) Physician-directed, clinical quality improvement initiatives are focused not on individual patients, but on physicians identifying those processes which have historically given their patients the highest quality and most cost efficient outcomes in their own hospitals. These processes are associated with patients having acceptable mortality and morbidity rates and with lower lengths of stay and fewer resource consumptions (charges). (The patients whose outcomes were from the right upper-hand quadrant as demonstrated on the four quadrant graphs.) The model is based on the principle that good physicians, given good clinical data, will make sound clinical decisions that continuously improve quality and cost efficiencies. When physicians are presented with their own, risk-adjusted clinical outcomes that reveal significant outcomes variations, and are given the tools to identify which of their processes yielded the best outcomes or mortality, morbidity, lower LOS and fewer resources, they almost always become willing to construct clinical pathways around those superior outcomes. Experience has shown that physicians do not mind making improvements on their own processes, but they are reluctant to make changes based on other hospitals data. Every doctor reads the medical literature to determine superior evidence-based protocols for treating patients. But those evidencebased processes allow for tremendous variations in practice patterns from hospital to hospital. Using their own data seems to make all the difference to physicians perceptions of how they should approach process and quality improvement. To keep the process on a path of constant improvement, each clinical services outcomes data are fed back to the doctors every six months to demonstrate where outcomes are improving and which process and outcomes need further improvement. It is a continuous clinical process improvement cycle that requires a commitment on the part of both the hospital and physicians
Q) Observation: This is a very thorough presentation with practical examples. A) Thank you. We would like to know if you have experienced similar successes that you would be willing to share. We are concerned that unless a significant number of US hospitals and physicians are willing to control their costs and variations and then be willing to publicly demonstrate the quality and cost efficiencies of their medical care to local businesses and patients, that the US will lose our excellent healthcare system as we know it. Q) Ive had to take a few calls during the presentation. Will this be available for playback? A) The white paper and presentation that describes the risk-adjusted data and quality improvement process can be downloaded from either the HP or Crossflo websites. Additionally, the webinar can be downloaded from the same sites. Q1) Issues with this distributed image analysis is fine but how about patient data privacy protection? HIPAA has regulation on this. Can the speaker elaborate a bit on patient data protection issues? Q2) Who is in charge for the physician purchasing pattern within the hospital environment? And how do they enforce this policy? Q3) For the AMI Mortality Rates by Gender slide, what is the sample size (i.e. population size or number of patients used for this graph)? A1) All the data presented during the webcast were derived using hospitals medical records data. The analyses of those data are performed by hospital quality and utilization management personnel for inpatient quality improvement activities and as such, are subject to the same hospital quality assurance HIPAA regulations as any other quality improvement activities. Patient data protection issues arise when moving patients medical records to the point of care is entirely different matter, as your question implies. The HP-Crossflo data sharing solution that was discussed is designed for intra-hospital, interhospital as well as inter-agency data sharing where patient privacy is a critical matter. These agencies were speaking about include public health, state HHS and Department of Homeland Securityany agency associated with firstresponders. These data require encryption to insure patient privacy. It is the only means by which the National Health Information Network can be implemented. The Crossflo CDX3 software discussed for this integrated health system is routinely used for data sharing in highly secure environments including Department of Defense, Department of Homeland Security
and the FBI. Security and therefore encryption is very important to these agencies just as it is in healthcare. Using CDX, encryption can be performed at every level of the data files that are transmitted, such as at the individual field level or the entire document. A2) The question of physicians consumptions of hospital resources is not really a physician purchasing pattern issue. Physicians choose the various tests and treatments for their patients based on the clinical presentations of those patients. Physician-directed clinical process improvement insures that the physicians themselves are responsible for the quantities and types of resources that are used to manage patients. It is the medical staff members who determine what resources are deployed on which patients and the key is that all decisions are data-driven.
A3) Try as we might, we were unable to identify the hospital where the slide originated. However, this is a fairly common quality issue so I have included two, more recent hospital evaluations and their data. Example 1: Hospital A with 420 patients last year with Acute Myocardial Infarction (AMI) and an overall Mortality Rate of 13%.
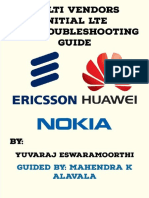
Expected Rate is not engaged so gets set to the most ideal target of 0. The Lower and Upper Limit define the 95% confidence intervals. Hospital A AMI Mortality Rates By Genderoverall AMI Mortality 13%. The women with AMI have a higher mortality rate then the men. The confidence intervals between the women and men almost overlap but do not and thus there is a significant difference in the female vs male rates.
The charts show the overall AMI population for a facility along with the breakdown by gender. The table at the bottom of each graph shows the statistics used. The Population column shows the number of AMI cases and the Indicator Cases column shows the number of AMI cases with mortality. The Indicator Cases divided by the Population defines the Actual Rate. Improvement is measured by a decrease in rate. The Expected Rate shows a comparison rate generated from regional model data and the Delta Rate shows the difference between the facilitys Actual Rate and the regional Expected Rate. In both of these charts the
Hospital B with 522 patients with AMI and an overall Mortality Rate of about 7%:
If the confidence intervals overlap there is not a statistical difference between the men and women. An even better example may be found in facility Hospital B AMI Mortality Rates By Gender. The overall AMI Mortality Rate is around 7% and the Female Rate is around 1 and the Male Rate is 1% around 3%. The confidence intervals are very far apart showing a significant difference in the female population and it is contributing greatly to the overall rate. Focusing improvement efforts on the AMI female population to bring in line with the male population could save 8 or more lives. Q) I am an ED director buying an information system for our medical records. However, the hospital system McKesson requires an ADT interface to be able to use it only to get the demographics. Cost $8K!
A) I assume you are asking if CDX3 can be used to interface between an ED information system that you are going to purchase and your hospitals McKesson ADT system in order to share clinical data in addition to patient demographics. Crossflo has a software solution that can share data between your ED systems irrespective of the ones you have [or choose], and the hospitals McKesson system; that is what CDX3 is designed to do. The difference would be that the CDX solution would share clinical, financial or any other information as well as demographic data.
Q) Do you have any additional information that can be emailed or sent to the participants? A) The white paper and presentation that describes the risk-adjusted data and quality improvement process can be downloaded from either the HP or Crossflo websites. Also, the webinar can also be downloaded from the same sites. If additional information is needed, please email me (Bill Mohlenbrock) and Ill try to answer your question. (Phone858.724.2216 ext 246 or bmohlenbrock@crossflo.com) Q) How would you suggest that a county could select a clinical indicator to track across time and measure improvement? A) A county has limited choices. Without a riskadjustment methodology, your best bet would be to use the publicly available National Hospital Quality Measures (NHQM) tool. It contains Mortalities, some process outcomes as well as patient satisfaction outcomes. The problem is its lack of sensitivity in being able to differentiate significant differences in hospitals outcomes. But, its a start. Q1) Why hasnt Iameter methodology been more broadly accepted since its formulation in the mid 80? Q2) Why will it be accepted now? A1) This is a good but complex question. Iameters clinical process improvement methodology has been used in 300 plus hospitals over the years, which is less than 5% of hospitals; not a large penetration as you point out. Iameters deployment by hospitals has been limited for several reasons; first of all it represents change, plus it requires extra work on the part of hospital personnel and physicians. It necessitates them working together to analyze data and create clinical pathways based on the physicians best-demonstrated process and outcomes. Even though the efficiency improvements more than makes up for the additional expense, few hospital administrations apparently have wished to engage the physicians in this wayhence the continued wide variations in clinical practices and resource consumptions.
Second, when hospitals have a positive bottom line, they see little reason to engage in a process that might upset the medical staff. Finally, most hospitals already feel they are doing an excellent job, so why subject themselves to scrutiny, especially when they are not being reimbursed for improving quality. This last point leads to your second question which is why will clinical quality improvement be accepted now? A2) Here is why HP and Iameter feel that the time is right for quality improvement. The difference in the medical environment now, compared to previous years, is the fact that hospitals and physicians have incentives that have been aligned by Medicare and are based on their quality outcomes. At this time, they do not have aligned financial incentives, only quality incentives. Iameters experience is that most physicians do not as yet appreciate this fact. For the first time in Medicares history, hospitals and physicians individual quality outcomes are both determined by data contained in each hospitals Medicare claims database. Hospitals are now being reimbursed more for improved quality and economically punished for poor quality, by CMS not paying for specific complications and by having CMS dollars recovered by arbitrary decisions through RACs. Physicians have no similar direct economic ties to qualityyet. However they now have quality ties to the hospitals claims database because in 2007 a federal judge ruled that physicians names and their quality outcomes can be published in public news outlets. Many cardiac surgeons have realized this too late; when their names appeared in their local papers as having unacceptably high mortality rates. Physicians who understand these issues will assist the hospital in making the hospitals medical records and CMS National Hospital Quality Measures (NHQM) databases as accurate and robust as possible. I spend a significant amount of time discussing these issues with physicians because this message is often easier for an outsider to deliver than someone from the hospital staff or administration.
Q) How great might the financial impact be on hospitals of the RACs when they are expanded from the pilot program to the rest of the country? A) The RAC pilot program has already netted tens of millions of dollars for Medicare in only a few hospitals. A country-wide RAC implementation will probably net hundreds of millions of dollars for Medicare and will undoubtedly be seen to be very positive from their standpoint. No one can predict what the expanded program will do to hospitals, but with hospital margins already being stretched thin, the RACs may have devastating results. Q) Integrating data between disparate sources is an expensive and difficult effort. You say that Crossflo can make it happen much faster and easier. Can you please explain? A) The time and cost savings, as well as ease of deployment, is due to Crossflos CDX software being able to share data without the need for custom programming. CDXs Services Oriented Architecture and JAVA/J2EE server platform makes it agnostic to platforms, server applications, databases and applications in secure environments. Moreover, it is able to harmonize all published data sharing standards such as HL7, GJXDM and NIEM for maximum cross-facility and cross-agency information exchanges. The technology maintains database vendor neutrality by leveraging web services, XML, and Java. Moreover, DataExchange employs a hub-andspoke architecture to minimize deployment costs. As part of the hub-and-spoke architecture, the exchange of data is orchestrated using a publish and subscribe data sharing model whose queries support federated, scheduled and event-triggered schemes. CDX creates an interoperable information infrastructure that is able to facilitate the exchange of data between disparate data sources and across multiple platforms to support basically any type of medical information integration applications. In short, its easy, fast and relatively inexpensive especially when deployed with a physiciandirected, clinical process improvement initiative as we discussed on the webinar. Q1) How is the ease of use problem being answered?
Q2) Is this system using the CCR (Continuity Care Record)? A1) The time and cost savings, as well as ease of deployment and ongoing use, is due to Crossflos CDX software being able to share data without the need for custom programming. CDXs Services Oriented Architecture and JAVA/J2EE server platform makes it agnostic to platforms, server applications, databases and applications in secure environments. Moreover, it is able to harmonize all published data sharing standards such as HL7, GJXDM and NIEM for maximum cross-facility and cross-agency information exchanges. The technology maintains database vendor neutrality by leveraging web services, XML, and Java. Moreover, DataExchange employs a hub-and-spoke architecture to minimize deployment costs. As part of the huband-spoke architecture, the exchange of data is orchestrated using a publish and subscribe data sharing model whose queries support federated, scheduled and event-triggered schemes. CDX creates an interoperable information infrastructure that is able to facilitate the exchange of data between disparate data sources and across multiple platforms to support basically any type of medical information integration applications. For these reasons, the ease of use is maximized irrespective of the type of medical information contained in the records being exchanged. In short, its easy, fast and relatively inexpensive especially when deployed with a physiciandirected, clinical process improvement initiative as we discussed on the webinar. A2) The Continuity Care Record is a logical data set to be shared among clinicians since the types of information are standardized. However, the CDX software is able to exchange other and varied types of medical data as well. Crossflos CDX is designed to utilize standards for all data sharing. As you probably know, the ANSI Continuity of Care Document (CCD) standard is the improvement to the HL7 Clinical Document Architecture (CDA) and the ASTM Continuity of Care Record (CCR) standards. The CCD is essentially a CCR mapped into a HL7 CDA. CCHIT 2008 requires EHRs to be CCD compatible. CDX3 is HL7 compliant and has no problem working with EHRs that meet this standard or in helping EHRs meet this need.
Q1) Is the Crossflo software CCHIT certified? Q2) Does the software utilize industry Standards CCD for the EHR/PHR information exchange between point of care? Q3) Also, does it provide interoperability with Health Information Exchanges external to the hospital/ physician provider? A1) CCHIT Certified? No, because as Im sure you know, vendors such as Crossflo are not certifiable at this time. However, CDX3 supports the industry standards that are part of the criteria for CCHIT certification. To quote the Certification Handbook, CCHIT certification will be offered to organizations that are legally responsible for the oversight, management, and delivery of services for exchanges of health information and at this point in time, CCHIT is not certifying vendor or consulting organizations that provide, software hardware, network, and other services to health information exchanges. A2) CCD for EHR/PHR?Yes. Crossflos CDX is designed to utilize standards for all data sharing. As you probably also know, the ANSI Continuity of Care Document (CCD) standard is the improvement to the HL7 Clinical Document Architecture (CDA) and the ASTM Continuity of Care Record (CCR) standards. The CCD is essentially a CCR mapped into a HL7 CDA. CCHIT 2008 requires EHRs to be CCD compatible. CDX3 is HL7 compliant and has no problem working with EHRs that meet this standard or in helping EHRs meet this need.
A3) Interoperability? Yes, it provides interoperability with Health Information Exchanges external to the hospital/physician providers and in fact is extensively used by public safety agencies such as state police and FBI for just that reason. CDXs Services Oriented Architecture and JAVA/J2EE server platform make it agnostic to platforms, server applications, databases and applications in secure environments. Moreover, DataExchange employs a hub-andspoke architecture to minimize deployment costs. As part of the hub-and-spoke architecture, the exchange of data is orchestrated using a publish and subscribe data sharing model whose queries support federated, scheduled and event-triggered schemes. CDX creates an interoperable information infrastructure that is able to facilitate the exchange of data between disparate data sources and across multiple platforms to support basically any type of medical information integration applications. For these reasons, the ease of use is maximized irrespective of the type of medical information contained in the records being exchanged, whether internal or external to the hospital/physician provider enterprise.
Learn more today To view the webinar on-demand, please visit www.healthcareitnews.com/hpcf.
To get more information or answers to questions you may have, please talk to your HP representative.
2009 Hewlett-Packard Development Company, L.P. The information contained herein is subject to change without notice. The only warranties for HP products and services are set forth in the express warranty statements accompanying such products and services. Nothing herein should be construed as constituting an additional warranty. HP shall not be liable for technical or editorial errors or omissions contained herein
9 9
You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Electromagnetic Energy May Hold The KeyDocument13 pagesElectromagnetic Energy May Hold The KeyAlex SmithNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Pre-Contract Scope Review - Event GuideDocument12 pagesPre-Contract Scope Review - Event GuideAlex SmithNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- PowerChart Inpatient Agenda TTTDocument4 pagesPowerChart Inpatient Agenda TTTAlex SmithNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Lewis, R.D. (2005) - When Cultures Collide - Chapter 11 ExcerptDocument9 pagesLewis, R.D. (2005) - When Cultures Collide - Chapter 11 ExcerptAlex SmithNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Richest Cities PDFDocument9 pagesRichest Cities PDFZerohedgeNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Design and Implementation of Oinline Course Registration and Result SystemDocument77 pagesDesign and Implementation of Oinline Course Registration and Result SystemAdams jamiu67% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- VfsBook Eng by Moshe Shemesh Ver071 SampleDocument36 pagesVfsBook Eng by Moshe Shemesh Ver071 SampleArina BorovikovaNo ratings yet
- E. B. Magalona National High School Summative Test in CSS 10 Quarter 1 Week 1 Multiple Choice. Choose The Letter of The Correct AnswerDocument2 pagesE. B. Magalona National High School Summative Test in CSS 10 Quarter 1 Week 1 Multiple Choice. Choose The Letter of The Correct Answerric jason pedralNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Quick Start: Issue DateDocument15 pagesQuick Start: Issue DatebqbertNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Probability and Stochastic Processes: A Friendly Introduction For Electrical and Computer Engineers Roy D. Yates and David J. GoodmanDocument2 pagesProbability and Stochastic Processes: A Friendly Introduction For Electrical and Computer Engineers Roy D. Yates and David J. GoodmantariqrazaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- 08 Russwurm Dirk On Site - Partial PDFDocument11 pages08 Russwurm Dirk On Site - Partial PDFzomglolzscribdNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- OSPF Protocol OutlineDocument18 pagesOSPF Protocol OutlinehiNo ratings yet
- NGT Transceiver Reference Manual - ENDocument427 pagesNGT Transceiver Reference Manual - ENMarcus0% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Estimate Distance Measurement Using Nodemcu Esp8266 Based On Rssi TechniqueDocument5 pagesEstimate Distance Measurement Using Nodemcu Esp8266 Based On Rssi TechniqueBrendo JustinoNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Etas Etk-S4.2 Emulator Probe For Infineon Tricore Tc17Xx: User GuideDocument93 pagesEtas Etk-S4.2 Emulator Probe For Infineon Tricore Tc17Xx: User GuideAmine HerbacheNo ratings yet
- CTI Technical Manual PDFDocument40 pagesCTI Technical Manual PDFYashveer Takoory100% (4)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Safe use and storage of toolsDocument4 pagesSafe use and storage of toolsMM Ayehsa Allian SchückNo ratings yet
- Nems Lock Server InstallationDocument27 pagesNems Lock Server InstallationbathcolNo ratings yet
- MuJava Supporting DocumentationDocument22 pagesMuJava Supporting DocumentationKhushboo KhannaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 9399PLC5UMDocument542 pages9399PLC5UMneoflashNo ratings yet
- EE311 Lecture OneDocument18 pagesEE311 Lecture OneĤmăđę HmNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Jim Highsmith, Linda Luu, David Robinson - EDGE - Value-Driven Digital Transformation-Addison-Wesley Professional (2019)Document254 pagesJim Highsmith, Linda Luu, David Robinson - EDGE - Value-Driven Digital Transformation-Addison-Wesley Professional (2019)gangadhar krishnamoorthyNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Apple's Change Management Strategies Driving InnovationDocument14 pagesApple's Change Management Strategies Driving InnovationjshfgshjfgNo ratings yet
- Effectiveness of Personal Interaction in A Learner-Centered Paradigm Distance Education Class Based On Student SatisfactionDocument2 pagesEffectiveness of Personal Interaction in A Learner-Centered Paradigm Distance Education Class Based On Student SatisfactionAlthea Mae GelacioNo ratings yet
- Use of Computers in PSychological TestingDocument18 pagesUse of Computers in PSychological TestingEder DolendoNo ratings yet
- Jawaban Pertanyaan Forum B.Inggris Simple Present Dan Present ContinuousDocument3 pagesJawaban Pertanyaan Forum B.Inggris Simple Present Dan Present ContinuousTirza NaomiNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- VP Interactive Media Digital in Los Angeles CA Resume Paul JoffeDocument2 pagesVP Interactive Media Digital in Los Angeles CA Resume Paul JoffePaulJoffeNo ratings yet
- Big Data AnalyticsDocument85 pagesBig Data AnalyticsFaiq Ghawash100% (1)
- Chapter 4 - Ethics in The MarketplaceDocument21 pagesChapter 4 - Ethics in The MarketplaceTina Mariano Dy100% (1)
- Detector Multigas ALTAIR 4X PDFDocument1,420 pagesDetector Multigas ALTAIR 4X PDFjollamorNo ratings yet
- 024943Document5 pages024943samon samvannak100% (2)
- SpaceClaim DocumentationDocument1,291 pagesSpaceClaim DocumentationV CafNo ratings yet
- All Basic Python Programs:: # Vowels ListDocument6 pagesAll Basic Python Programs:: # Vowels ListBHANU REKHA CHUNDUNo ratings yet
- Education AfghanistanDocument15 pagesEducation AfghanistanAnonymous EFcqzrdNo ratings yet
- Errfree 803004 09.22Document5 pagesErrfree 803004 09.22Mariana PerezNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)