Professional Documents
Culture Documents
Art 3 Sexual Behaviours HIV Testing and The Proportion of Men at Risk of Transmitting
Art 3 Sexual Behaviours HIV Testing and The Proportion of Men at Risk of Transmitting
Uploaded by
Juan Carlos Riveros MedinaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Art 3 Sexual Behaviours HIV Testing and The Proportion of Men at Risk of Transmitting
Art 3 Sexual Behaviours HIV Testing and The Proportion of Men at Risk of Transmitting
Uploaded by
Juan Carlos Riveros MedinaCopyright:
Available Formats
Articles
Sexual behaviours, HIV testing, and the proportion of men
at risk of transmitting and acquiring HIV in London, UK,
2000–13: a serial cross-sectional study
Adamma Aghaizu*, Sonali Wayal*, Anthony Nardone, Victoria Parsons, Andrew Copas, Danielle Mercey, Graham Hart, Richard Gilson,
Anne M Johnson
Summary
Background HIV incidence in men who have sex with men (MSM) in the UK has remained unchanged over the past Lancet HIV 2016; 3: e431–40
decade despite increases in HIV testing and antiretroviral therapy (ART) coverage. In this study, we examine trends Published Online
in sexual behaviours and HIV testing in MSM and explore the risk of transmitting and acquiring HIV. July 14, 2016
http://dx.doi.org/10.1016/
S2352-3018(16)30037-6
Methods In this serial cross-sectional study, we obtained data from ten cross-sectional surveys done between
See Comment page e400
2000 and 2013, consisting of anonymous self-administered questionnaires and oral HIV antibody testing in MSM
*Contributed equally
recruited in gay social venues in London, UK. Data were collected between October and January for all survey years up to
HIV and STI Department,
2008 and between February and August thereafter. All men older than 16 years were eligible to take part and fieldworkers National Infection Service,
attempted to approach all MSM in each venue and recorded refusal rates. Data were collected on demographic and sexual Public Health England, London,
behavioural characteristics. We analysed trends over time using linear, logistic, and quantile regression. UK (A Aghaizu MSc,
A Nardone PhD); and Centre for
Sexual Health and HIV
Findings Of 13 861 questionnaires collected between 2000 and 2013, we excluded 1985 (124 had completed the survey Research, University College
previously or were heterosexual reporting no anal intercourse in the past year, and 1861 did not provide samples for London, London, UK
antibody testing). Of the 11 876 eligible MSM recruited, 1512 (13%) were HIV positive, with no significant trend in HIV (S Wayal PhD, V Parsons MSc,
positivity over time. 35% (531 of 1505) of HIV-positive MSM had undiagnosed infection, which decreased non-linearly A Copas PhD, D Mercey FRCP,
Prof G Hart PhD, R Gilson FRCP,
over time from 34% (45 of 131) to 24% (25 of 106; p=0·01), while recent HIV testing (ie, in the past year) increased from Prof A M Johnson MD)
26% (263 of 997) to 60% (467 of 777; p<0·0001). The increase in recent testing in undiagnosed men (from 29% to 67%, Correspondence to:
p<0·0001) and HIV-negative men (from 26% to 62%, p<0·0001) suggests that undiagnosed infection might increasingly Prof Anne M Johnson, Centre for
be recently acquired infection. The proportion of MSM reporting unprotected anal intercourse (UAI) in the past year Sexual Health and HIV Research,
increased from 43% (513 of 1187) to 53% (394 of 749; p<0·0001) and serosorting (exclusively) increased from 18% University College London,
London WC1E 6JB, UK
(207 of 1132) to 28% (177 of 6369; p<0·0001). 268 (2%) of 11 570 participants had undiagnosed HIV and reported UAI in Anne.Johnson@ucl.ac.uk
the past year were at risk of transmitting HIV. Additionally 259 (2%) had diagnosed infection and reported UAI and
non-exclusive serosorting in the past year. Although we did not collect data on antiretroviral therapy or viral load,
surveillance data suggests that a small proportion of men with diagnosed infection will have detectable viral load and
hence might also be at risk of transmitting HIV. 2633 (25%) of 10 364 participants were at high risk of acquiring HIV
(defined as HIV-negative MSM either reporting one or more casual UAI partners in the past year or not exclusively
serosorting). The proportions of MSM at risk of transmission or acquisition changed little over time (p=0·96 for MSM
potentially at risk of transmission and p=0·275 for MSM at high risk of acquiring HIV). Undiagnosed men reporting
UAI and diagnosed men not exclusively serosorting had consistently higher partner numbers than did other MSM over
the period (median ranged from one to three across surveys in undiagnosed men reporting UAI, two to ten in diagnosed
men not exclusively serosorting, and none to two in other men).
Interpretation An increasing proportion of undiagnosed HIV infections in MSM in London might have been recently
acquired, which is when people are likely to be most infectious. High UAI partner numbers of MSM at risk of transmitting
HIV and the absence of a significant decrease in the proportion of men at high risk of acquiring the infection might
explain the sustained HIV incidence. Implementation of combination prevention interventions comprising both
behavioural and biological interventions to reduce community-wide risk is crucial to move towards eradication of HIV.
Funding Public Health England.
Introduction annual number of new HIV diagnoses (2800 new
In the UK, men who have sex with men (MSM) are at the infections estimated in 2013).3,4 One study3 used a back-
highest risk of acquiring HIV. The annual number of calculation approach based on CD4 cell count at
new HIV diagnoses in MSM has increased from 1830 in diagnosis; the other study is a dynamic model of sexual
2000 to 3270 in 2013.1,2 Two studies have shown that behaviours.4 Given the greatly increased uptake of HIV
estimated HIV incidence over this period remained testing and antiretroviral therapy (ART) in the past
stable (increasing slightly), and is now similar to the decade, which should reduce transmission by reducing
www.thelancet.com/hiv Vol 3 September 2016 e431
Articles
Research in context
Evidence before this study Added value of this study
We searched PubMed for articles published in English up to Our data indicate changes in sexual risk behaviours with
May 3, 2016, with the terms “sexual behaviour”, “MSM”, increasing rates of UAI and serosorting, with serosorting
“homosexuality or male”, “trends”, “HIV”, “HIV infections” or considered to be a risk reduction strategy. Our findings
“HIV antibodies” or “HIV seropositivity” or “saliva” or “incidence” emphasise the importance of core groups in the epidemiology
or “prevalence”, “UK”, and “Great Britain”. Only one other study and control of HIV infection in MSM in the UK, with one in
has examined trends in sexual behaviours in UK men who have 20 MSM identified as being potentially at risk of transmitting
sex with men (MSM; recruited from gyms across London) HIV and one in four at risk of acquiring HIV. An increasing
between 1998 and 2008, which found lower rates of MSM proportion of MSM with undiagnosed HIV infection might
reporting unprotected anal intercourse (UAI) overall than in this have a recently acquired infection (ie, acquired within the past
study, but also an increase in the proportion of men reporting UAI 12 months) during which the individual is most infectious.
and to serosort. No studies reported trends in sexual behaviours This finding, coupled with the high partner numbers of a core
in the UK in more recent years and none showed trends in group of MSM potentially at risk of transmitting HIV, and the
numbers of sexual partners in this population. One cross- sustained proportion at men at risk of acquiring the infection,
sectional study in HIV-positive MSM recruited from HIV clinics could explain the persistent HIV incidence in the UK, despite
between 2011 and 2012 showed a lower prevalence of UAI (38%) increases in HIV testing and antiretroviral therapy coverage.
and serosorting (28%). Another cross-sectional study in 2008
Implications of all the available evidence
also found a lower prevalence of serosorting and strategic
Growing evidence shows that test-and-treat interventions
positioning during UAI in MSM in Scotland with 11% in
alone are not sufficient to reduce HIV incidence at the
HIV-positive and 13% in HIV-negative MSM. Three modelling
population level. Combination prevention interventions will be
studies that used multiple national surveillance databases show
crucial for countries with similar epidemics in MSM.
no reduction in undiagnosed HIV infection and an increase in
HIV testing. Additionally, similar patterns were found in
community-based surveys done in England and Scotland.
viral load, sustained HIV incidence supports the notion have been described in detail elsewhere.9,10 Briefly, from
that risk behaviours have increased over this period.5 2000 to 2013, ten surveys were done. For each survey,
Since the introduction of ART in the mid-1990s, studies fieldworkers visited 38–58 bars, clubs, and saunas across
suggest the prevalence of high-risk sexual behaviours in London, UK, over 3 months inviting MSM to self-complete
MSM is increasing (at least partly) because of treatment short, anonymous questionnaires on demographic and
optimism, relating both to the greatly reduced morbidity sexual behaviour characteristics and to provide oral fluid
and mortality associated with the infection, and the specimens for HIV antibody testing (OraSure Technologies,
reduced risk of transmission from a positive partner Bethlehem, PA, USA). Participants were recruited between
(which was discovered after 2011).6,7 Few behavioural October and January for all survey years up to 2008 and
studies are able to explore trends in sexual behaviours in between February and August in 2011 and 2013. A barcode
detail, in particular examining seroadaptive behaviours linked specimens to the corresponding questionnaire.
relating to confirmed versus perceived HIV status. Participants were informed that the specimens would be
Guidelines suggest that MSM should test for HIV once a tested for research purposes only and results would not be
year and at least every 3 months if having unprotected returned to them. All participants were advised to attend a
anal intercourse (UAI) with new or casual partners.1,8 In health-care setting for a named HIV test if they wanted to
this Article, we examine trends in both sexual risk and know their status. All men aged 16 years and older in the
HIV testing behaviours against a background of targeted study venues were eligible to take part and fieldworkers
prevention and testing initiatives in MSM recruited from attempted to approach as many people as possible and
community venues in London over the past 14 years. recorded refusal rates. Ethical approval was granted each
With half of all new HIV diagnoses in the UK occurring year by the UCL research ethics committee (00/0158).
in London, these trends can be used to understand the Verbal consent for anonymous saliva samples and self-
role of behavioural change and testing in driving completion of questionnaires was obtained to ensure
continued HIV transmission. anonymity of all participants.
Methods Procedures
Study population and data collection Oral fluid samples, collected with the OraSure kit, were
In this serial cross-sectional study, we obtained data from tested for HIV-1 antibody at Public Health England
the Gay Men’s Sexual Health Survey—a regular com- (London) with GACELISA (Abbott Laboratories,
munity-based survey done since 1996. The survey methods Maidenhead, UK). All samples were tested for total
e432 www.thelancet.com/hiv Vol 3 September 2016
Articles
immunoglobulin (IgG) to assess the specimen quality, implications of the absence of these data for the
apart from samples collected in 2011, when a two-stage interpretation of our findings later. We defined MSM at
approach was used: first screening with a modified high risk of acquiring HIV as men who were HIV
enzyme immunoassay then by rescreening positive negative and reported one or more casual UAI partners or
specimens with an enzyme immunoassay and a were not exclusively serosorting in the past year. All other
western blot (HIV blot 2.2; Genelabs, Redwood City, HIV-negative men were regarded as being at lower risk of
CA, USA). acquiring HIV than men at high risk.
We defined undiagnosed infection as a participant who
had a positive OraSure specimen and reported that they Statistical analysis
had never had an HIV test, or they perceived themselves We analysed data using Stata (version 13.0). Analyses were
to be negative or didn’t know, or the result of their last stratified by HIV status. We examined the significance of
test was negative. We defined a casual partner as a trends over time using linear, logistic, and quantile
partner with whom UAI (condomless) was reported once regression, adjusted for age, with survey year modelled as
only and defined a regular partner as a partner with a linear term. For trends in HIV testing, overall HIV
whom the participant had had UAI more than once in positivity, and undiagnosed HIV, we also adjusted for
the past year. Exclusively serosorting was defined as education, employment, and ethnicity, and assessed
having UAI only with partners of presumed same HIV linearity with a likelihood ratio test relative to a model with
status in the past year. Status is referred to as presumed survey year as a categorical variable. Characteristics of
because the HIV status of partners was self-reported by MSM at potential risk of transmitting and at high risk of
respondents, as established with the question, “In the acquiring HIV were explored with a multivariable model
past year, how many men that you had active/passive controlling for the year of survey as a linear term (odds
anal intercourse without a condom did you know had the ratios [OR] for year not shown). Factors significant to
same HIV status as you?” p<0·05 in univariable analyses were included in the
MSM potentially at risk of transmitting HIV were multivariable model.
defined as men with undiagnosed HIV reporting UAI in
the past year or with diagnosed HIV reporting UAI and Role of the funding source
not exclusively serosorting in the past year. In the latter The funder contributed to the study design, data
group, most men might have had undetectable viral load collection, data analysis, data interpretation, and writing
as a result of ART and might therefore not have been at of the report. The corresponding author had full access
risk of transmitting, but information on ART and viral to all the data in the study and had final responsibility for
load were not collected in this study. We discuss the the decision to submit for publication.
Total Year p value*
2000 2001 2002 2003 2004 2005 2006 2008 2011 2013
HIV positive
All MSM 13% 11% 11% 12% 12% 13% 13% 17% 15% 8% 14% p<0·001†
(1512/11 876) (132/1206) (150/1309) (126/1043) (177/1432) (177/1377) (195/1503) (200/1153) (167/1106) (82/965) (106/782)
HIV positive, 35% 34% 49% 33% 44% 41% 29% 35% 28% 29% 24% p=0·01†
undiagnosed (531/1505) (45/131) (74/150) (42/126) (78/177) (73/177) (56/193) (68/197) (46/166) (24/82) (25/106)
Tested for HIV (ever)
All MSM 79% 63% 69% 76% 78% 78% 80% 83% 89% 90% 91% p<0·004
(9184/11 568) (629/997) (900/1297) (788/1035) (1112/1420) (1065/1363) (1195/1487) (952/1142) (972/1092) (862/958) (709/777)
HIV negative 78% 62% 67% 75% 77% 76% 79% 81% 87% 89% 90% p<0·0001
(7886/10 161) (567/920) (770/1150) (683/912) (955/1248) (904/1189) (1024/1303) (770/950) (818/935) (787/880) (608/674)
HIV positive, 79% 57% 77% 57% 80% 82% 77% 85% 93% 88% 92% p<0·0001
undiagnosed (408/517) (20/35) (57/74) (24/42) (61/76) (60/73) (43/56) (58/68) (42/45) (21/24) (22/24)
% tested for HIV (in the past year)
All MSM 42% 26% 32% 36% 39% 42% 43% 44% 51% 56% 60% p<0·0001
(4891/11 568) (263/997) (421/1297) (375/1035) (550/1420) (576/1363) (634/1487) (504/1142) (560/1092) (532/958) (467/777)
HIV negative 42% 26% 32% 37% 39% 42% 43% 44% 52% 57% 62% p<0·0001
(4312/10 161) (241/920) (370/1150) (334/912) (482/1248) (498/1198) (563/1303) (422/950) (485/935) (501/880) (416/674)
HIV positive, 43% 29% 30% 21% 46% 49% 39% 56% 53% 50% 67% p<0·0001
undiagnosed (224/517) (10/35) (22/74) (9/42) (35/76) (36/73) (22/56) (38/68) (24/45) (12/24) (16/24)
Data are % (n/N), unless otherwise specified. Denominators vary because of incomplete data on all variables. Percentages might not add up to totals because of rounding. MSM=men who have sex with men.
*Adjusted for age, education, ethnicity, and employment. †p value for association between outcome and survey year (categorical) because data showed evidence of departure from linearity.
Table 1: HIV status and HIV testing in MSM in London, 2001–13
www.thelancet.com/hiv Vol 3 September 2016 e433
e434
Articles
Total Year p value*
2000 2001 2002 2003 2004 2005 2006 2008 2011 2013
UAI in the past year
HIV negative 46% 42% 45% 42% 46% 43% 49% 46% 47% 50% 51% p<0·0001
(4651/10 139) (448/1058) (510/1138) (378/907) (567/1235) (502/1173) (633/1291) (431/927) (430/920) (423/843) (329/647)
HIV positive, diagnosed 60% 49% 47% 58% 62% 66% 54% 66% 64% 62% 64% p=0·002
(556/934) (41/84) (35/74) (46/79) (58/94) (65/98) (70/129) (82/125) (74/116) (34/55) (51/80)
HIV positive, undiagnosed 54% 53% 59% 54% 44% 57% 62% 56% 43% 52% 64% p=0·93
(268/497) (24/45) (42/71) (21/39) (33/75) (38/67) (32/52) (35/63) (18/42) (11/21) (14/22)
All 47% 43% 46% 43% 47% 45% 50% 49% 48% 51% 53% p<0·0001
(5475/11 570) (513/1187) (587/1283) (445/1025) (658/1404) (605/1338) (735/1472) (548/1115) (522/1078) (468/919) (394/749)
Exclusively serosorted in the past year
HIV negative 21% 18% 18% 17% 21% 19% 23% 23% 24% 27% 27% p<0·0001
(1942/9166) (181/1007) (178/1015) (143/844) (242/1144) (198/1067) (271/1155) (186/817) (200/838) (193/725) (150/554)
HIV positive, diagnosed 26% 22% 19% 21% 30% 30% 24% 27% 30% 23% 30% p=0·06
(225/862) (18/83) (13/68) (15/72) (26/88) (28/92) (30/124) (31/114) (32/105) (11/47) (21/69)
HIV positive, undiagnosed 15% 19% 9% 9% 12% 10% 20% 13% 21% 18% 38% p=0·033
(64/438) (8/42) (6/64) (3/34) (8/67) (6/60) (9/46) (7/53) (8/39) (3/17) (6/16)
All 21% 18% 17% 17% 21% 19% 23% 23% 24% 26% 28% p<0·0001
(2231/10 466) (207/1132) (197/1147) (161/950) (267/1299) (232/1219) (310/1325) (224/984) (240/982) (207/789) (177/639)
Reported UAI with partners of unknown or discordant HIV status in the past year
HIV negative 19% 22% 21% 21% 21% 19% 20% 17% 18% 16% 16% p<0·0001
(1748/9166) (218/1007) (211/1015) (173/844) (235/1114) (200/1067) (229/1155) (136/817) (148/838) (112/725) (86/554)
HIV positive, diagnosed 30% 27% 24% 33% 30% 34% 28% 35% 30% 32% 28% p=0·433
(259/862) (22/83) (16/68) (24/72) (26/88) (31/92) (35/124) (40/114) (31/105) (15/47) (19/69)
HIV positive, undiagnosed 33% 31% 45% 38% 25% 43% 37% 34% 18% 24% 13% p=0·012
(146/438) (13/42) (29/64) (13/34) (17/67) (26/60) (17/46) (18/53) (7/39) (4/17) (2/16)
All 21% 22% 22% 22% 21% 21% 21% 20% 19% 17% 17% p<0·0001
(2153/10 466) (253/1132) (256/1147) (210/950) (278/1299) (257/1219) (281/1325) (194/984) (186/982) (131/789) (107/639)
Number of UAI partners in the past year
HIV negative 1·4 (6·8) 0·9 (3·2) 1·6 (5·9) 1·2 (5·0) 1·4 (4·9) 1·3 (7·1) 1·7 (11) 1·3 (4·3) 1·3 (4·6) 1·4 (3·6) 1·9 (12·5) p=0·073
0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1)
HIV positive, diagnosed 9·2 (30·7) 4·7 (12·8) 4·6 (14·7) 8·3 (24·9) 7·9 (22·5) 7·1 (15·6) 9·3 (45·0) 13·5 (36·8) 11·8 (42·1) 12·6 (31·8) 9·7 (22·5) p=0·008
1 (0–5) 0 (0–2) 0 (0–2) 1 (0–7) 1 (0–4) 2 (0–5) 1 (0–5) 1 (0–5) 1 (0–5) 1 (0–11) 1 (0–10)
HIV positive, undiagnosed 4·1 (17·5) 1·6 (3·5) 3·8 (6·5) 2·9 (8·4) 5·3 (34·6) 6·5 (22·4) 4·5 (7·8) 4·0 (13·9) 1·5 (3·3) 1·2 (2·2) 7·4 (13·9) p=0·77
1 (0–2) 1 (0–1) 1 (0–3) 1 (0–1) 0 (0–2) 1 (0–2) 1 (0–4·5) 1 (0–2) 0 (0–2) 1 (0–1) 1 (0–5)
All 2·1 (11·6) 1·2 (4·7) 1·9 (6·9) 1·8 (8·7) 2·0 (11·0) 2·0 (9·5) 2·5 (17·0) 2·8 (13·8) 2·4 (14·8) 2·0 (8·9) 2·9 (14·2) p=0·0001
0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 0 (0–1) 1 (0–1) 1 (0–1)
Data are % (n/N), mean (SD), or median (IQR), unless otherwise reported. Denominators vary because of incomplete data on all variables. Percentages might not add up to totals because of rounding. MSM=men who have sex with men.
UAI=unprotected anal intercourse. *Adjusted for age.
Table 2: Sexual behaviour in MSM by HIV status, 2000–13
www.thelancet.com/hiv Vol 3 September 2016
Articles
Results (18 of 653) of men who perceived themselves to be HIV
13 861 questionnaires were collected between 2000 and negative had undiagnosed HIV in 2013, with no
2013. The proportion of MSM who responded ranged significant trend over time (data not shown).
between 50% and 70% each year. Venue data were The proportion of men reporting UAI with partners of
missing for 930 participants (two participants in 2002, unknown or discordant status decreased from 22% in
three participants in 2008, and all 925 participants 2000 to 17% in 2013 overall, from 22% to 16% in HIV-
in 2013). In the 12 931 participants for whom data were negative men, and from 31% to 13% in HIV-positive,
available, 10 578 (82%) were recruited from bars, 1636 (13%) undiagnosed men. In HIV-positive, diagnosed men the
from clubs, and 717 (6%) from saunas. We excluded changes were not significant.
124 questionnaires from men who completed the survey Over the 14 years of study, the mean number of sexual
previously or were heterosexual reporting no anal partners in the past year was consistently highest in
intercourse in the past year, leaving 13 737 questionnaires. diagnosed HIV-positive MSM and increased significantly
Additionally, questionnaires from 1861 men (13%) were from 4·7 (SD 12·8) partners in 2000 to 9·7 (22·5) in 2013,
excluded because they did not provide samples for having peaked at 13·5 (36·8) in 2006.
antibody testing, resulting in 11 876 questionnaires. Men Between 2000 and 2013, 259 diagnosed MSM reported
who did and did not give samples were similar in age, UAI (table 3) and were not exclusively serosorting, some
education, and employment status (data not shown), but of whom might have been at risk of transmitting HIV.
differed slightly by ethnic origin: 105 (6%) of 1856 men A further 268 undiagnosed HIV-positive MSM reported
who did not provide a sample were black compared with UAI (table 3). Together, they represented 5% of MSM
374 (3%) of 11 841 men who did. The demographic overall (table 3). The overall proportion of MSM
characteristics of 11 876 men included were similar in potentially at risk of transmitting HIV remained stable
each of the ten surveys (data not shown). Overall, the over the 14 year period, as did the proportion of men in
median age was 33 years (range 16–82 years) and this group who were diagnosed and undiagnosed. Both
10 201 (86%) of 11 841 men were white. diagnosed and undiagnosed MSM potentially at risk of
Across all study years, 1512 (13%) of 11 876 of transmitting HIV had consistently higher numbers of
participants were HIV positive, the proportion ranged UAI partners than did all other MSM, but the mean
from 8% in 2011 to 17% in 2006 (table 1). 35% of number of partners increased over time for all groups.
HIV-positive MSM (4% of the entire sample) were In 2013, undiagnosed men at risk of transmitting
undiagnosed, which decreased (non-linearly) over the reported a mean of 11·6 UAI partners (SD 16·1) and
period from 34% in 2000 to 24% in 2013. During this median of 2·5 (IQR 1–20) UAI partners in the past year;
period, recent HIV testing (in the past year) in all men diagnosed MSM, of whom some might be at risk of
increased from 26% to 60%. Recent testing increased in transmitting, reported a mean of 22·4 UAI partners
undiagnosed MSM at a similar rate, from 29% to 67%. (SD 30·0) and median of ten UAI partners (IQR 2–28)
The proportion of MSM ever having had an HIV test compared with other MSM with 2·2 UAI partners
increased from 63% in 2000 to 91% in 2013. HIV (SD 13·1) and one UAI partner (IQR 0–1). This shows
positivity varied by recruitment venue type with a similar
prevalence in MSM in bars (8% [740 of 9100] diagnosed,
2000 2013
4% [387 of 9100] undiagnosed) and clubs (6% [89 of 1375] 0·7% 1·9% 0·8% 4·0%
diagnosed, 5% [62 of 1375] undiagnosed), and the highest 1·3% 1·1%
1·5% 2·8%
prevalence in saunas (12% [71 of 617] diagnosed, 9%
[57 of 617] undiagnosed).
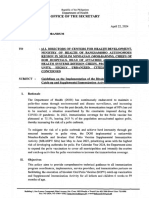
The proportion of MSM reporting UAI in the past year
increased from 43% in 2000 to 53% in 2013 (table 2, 22·5%
figure). This increase was significant in HIV-negative 23·9%
47·4%
56·8%
MSM, increasing from 42% to 51% and in HIV-positive,
diagnosed MSM, increasing from 49% to 64%. Numbers 15·2%
in undiagnosed MSM were small and no clear change 20·0%
was recorded (table 2); prevalence of UAI in undiagnosed
MSM varied between 43% and 64%.
No unprotected anal intercourse
The proportion of MSM who exclusively serosorted Diagnosed (exclusively serosorting)
increased overall from 18% in 2000 to 28% in 2013; in Undiagnosed (exclusively serosorting with presumed negative partners)
HIV-negative men (with other presumed HIV-negative Diagnosed (not exclusively serosorting)
Undiagnosed (not exclusively serosorting with presumed negative partners)
men) this increased from 18% to 27%. In HIV-positive, HIV–negative MSM (exclusively serosorting)
diagnosed men and in HIV-positive undiagnosed men HIV–negative MSM (not exclusively serosorting)
(who reported UAI with presumed HIV-negative men) Figure: Population prevalence of unprotected anal intercourse and
the numbers were small and changes in the proportion serosorting by HIV status in MSM in London, 2000 and 2013
serosorting were not significant (table 2). Notably, 3% MSM=men who have sex with men.
www.thelancet.com/hiv Vol 3 September 2016 e435
Articles
Total Year p value*
2000 2001 2002 2003 2004 2005 2006 2008 2011 2013
Potentially at risk of transmitting HIV†
Undiagnosed HIV-positive MSM reporting UAI in the past year
All MSM 2% 2% 3% 2% 2% 3% 2% 3% 2% 1% 2% 0·09
(268/11 570) (24/1187) (42/1283) (21/1025) (33/1404) (38/1338) (32/1472) (35/1115) (18/1078) (11/919) (14/749)
MSM reporting UAI 5% 5% 7% 5% 5% 6% 4% 6% 3% 2% 4% 0·005
(268/5475) (24/513) (42/587) (21/445) (33/658) (38/605) (32/735) (35/548) (18/522) (11/468) (14/394)
Mean (SD) number 7·6 3 6·5 5·5 12 11·4 7·4 7·1 3·5 2·4 11·6 0·62
of UAI partners‡ (23·2) (4·4) (10·2) (11·0) (51·8) (28·9) (8·9) (18·2) (4·4) (2·7) (16·1)
Median (IQR) of UAI 2 1 3 1 2 2 3 2 2 1 3 1·0
partners‡ (1–5) (1–2) (1–10) (1–5) (1–4) (1–3) (1–10) (1–4) (1–4) (1–3) (1–20)
Diagnosed MSM reporting UAI and not exclusively serosorting in the past year§
All MSM 2% 2% 1% 2% 2% 2% 2% 4% 3% 2% 3% 0·07
(259/11 570) (22/1187) (16/1283) (24/1025) (26/1404) (31/1338) (35/1472) (40/1115) (31/1078) (15/919) (19/749)
MSM reporting UAI 5% 4% 3% 5% 4% 5% 5% 7% 6% 3% 5% 0·47
(259/5475) (22/513) (16/587) (24/445) (26/658) (31/605) (35/735) (40/548) (31/522) (15/468) (19/394)
Mean (SD) number 17·8 13·4 16·1 13·8 13·9 12 9·5 28·8 24·0 22·7 22·4 0·05
of UAI partners‡ (39·5) (21·3) (27·6) (17·4) (23·4) (23·0) (11·5) (56·0) (71·5) (51·6) (30·0)
Median (IQR) of UAI 5 7 4 7 4 4 5 5 5 2 10 0·45
partners‡ (2–15) (2–15) (1–14) (3–16) (2–8) (2–15) (2–10) (2–16) (2–15) (1–20) (2–28)
Total
All MSM 5% 4% 5% 4% 4% 5% 5% 7% 5% 3% 4% 0·96
(527/11 570) (46/1187) (58/1283) (45/1025) (59/1404) (69/1338) (67/1472) (75/1115) (49/1078) (26/919) (33/749)
No reported risk of transmitting HIV¶
All MSM 95% 96% 95% 96% 96% 95% 95% 93% 95% 97% 96% 0·96
(11 043/11 570) (1141/1187) (1225/1283) (980/1025) (1345/1404) (1269/1338) (1405/1472) (1040/1115) (1029/1078) (893/919) (716/749)
MSM reporting UAI 90% 91% 90% 90% 91% 89% 91% 86% 91% 94% 92% 0·13
(4948/5475) (467/513) (529/587) (400/445) (599/658) (536/605) (668/735) (473/548) (473/522) (442/468) (361/394)
Mean (SD) number of 1·6 1·0 1·5 1·4 1·5 1·5 2·2 1·7 1·7 1·7 2·2 0·004
UAI partners‡ (9·2) (3·3) (5·8) (8·1) (6·9) (7·3) (17·2) (7·0) (8·1) (5·6) (13·1)
Median (IQR) of UAI 0 0 0 0 0 0 0 0 0 0 1 1·0
partners‡ (0–1) (0–1) (0–1) (0–1) (0–1) (0–1) (0–1) (0–1) (0–1) (0–1) (0–1)
At high risk of acquiring HIV||
All MSM 23% 24% 23% 23% 24% 22% 26% 19% 22% 22% 21% 0·275
(2633/11 570) (280/1187) (299/1283) (236/1025) (341/1404) (288/1338) (377/1472) (217/1115) (238/1078) (203/919) (154/749)
All HIV-negative MSM 25% 26% 26% 26% 27% 24% 29% 23% 25% 23% 23% 0·16
(2633/10 364) (280/1074) (299/1159) (236/917) (341/1255) (288/1200) (377/1308) (217/953) (238/939) (203/883) (154/676)
Mean (SD) of UAI 4·2 2·8 5·1 3·4 3·8 4·5 4·8 4·2 3·7 3·8 6·1 0·252
partners‡ (12·8) (5·7) (10·8) (9·0) (8·2) (13·9) (20·0) (8·1) (8·4) (6·0) (25·2)
Median (IQR) of UAI 2 2 2 1 1 2 2 2 2 2 2 1·0
partners‡ (1–3) (1–2) (1–4) (1–3) (1–3) (1–3) (1–4) (1–3) (1–3) (1–3) (1–4)
Tested for HIV in the 50% 34% 37% 44% 47% 50% 53% 51% 58% 70% 73% <0·001
past year (1288/2573) (79/234) (108/297) (102/234) (157/337) (141/284) (199/376) (110/217) (138/238) (143/203) (111/153)
Data are % (n/N), mean (SD), or median (IQR), unless otherwise specified. Denominators vary because of incomplete data on all variables. Percentages might not add up to totals because of rounding.
MSM=men who have sex with men. UAI=unprotected anal intercourse. *Adjusted for age. †MSM with undiagnosed HIV who reported UAI in the past year or MSM with diagnosed HIV who reported UAI and
not exclusively serosorting. ‡In the past year. §Data on antiretroviral therapy or viral load not available, so we were unable to ascertain if men in this group were on treatment and had undetectable viral loads
and therefore not at risk of transmitting HIV. ¶All MSM not including those who were potentially at risk of transmitting HIV who provided information on number of UAI partners. ||HIV-negative MSM
reporting one or more casual UAI partner or not exclusively serosorting in the past year.
Table 3: Proportion of MSM potentially at risk of transmitting and acquiring HIV, the number of UAI partners in the past year, and recent testing (in the past year) in men at high risk of
acquiring HIV, 2000–13
the skewed distribution of partner numbers, with no that MSM were more likely to be at risk of transmitting
increase over time for most men (medians largely HIV (than were all other MSM) if they were older, of
unchanged), but an increase in partners for the black ethnic origin, had a higher number of casual UAI
proportion at the upper end of the distribution, which partners in the past year, or had attended a genitourinary
increased the mean. Multivariable analyses revealed medicine clinic during the past year (table 4).
e436 www.thelancet.com/hiv Vol 3 September 2016
Articles
HIV-negative MSM were considered at high risk of (particularly undiagnosed) MSM reporting behaviours
HIV if they reported UAI with one or more casual conducive to transmission. These data will be useful in
partners or reported not exclusively serosorting in the modelling studies, because we are able to provide key
past year. Overall, 25% of HIV-negative men were at high variables such as rate of partner change and the
risk (table 3). HIV testing in the past year increased in proportion of the population at risk.
MSM in this group (table 3). Men at higher risk of One limitation of the study is that we had no
acquiring HIV were more likely to have had a higher information on the timing of infection in relation to
number of casual partners or have been diagnosed with a contact with sexual partners, or how many diagnosed
sexually transmitted infection in the past year than other individuals were on treatment and had undetectable viral
HIV-negative MSM (table 4). load for MSM at risk of transmitting HIV. In HIV
diagnosed men potentially at risk of transmitting, the
Discussion proportion diagnosed with a sexually transmitted
We report that the prevalence of HIV remains high at infection in the past year was double that of other MSM
13% in MSM in our London surveys. The uptake of HIV (39% vs 17%), which might have increased their risk of
testing increased substantially in the period 2000–13, and transmission. Second, the increase in recent testing in
the proportion of HIV that is undiagnosed decreased undiagnosed MSM is only suggestive of undiagnosed
concomitantly. Despite these changes, which might have infection being increasingly recently acquired, because
been expected, combined with improved uptake of we do not know the length of infection in men that were
treatment to reduce transmission, HIV incidence not tested.
remains high and unchanged.3,4 Our data show that Third, the surveys were convenience samples and might
irrespective of the positive changes in testing uptake, risk not be generalisable, comparable or both, over time. This
behaviour has increased over this period characterised by might also have restricted the ability to detect trends over
increased UAI and increasing numbers of sexual time. Response rates varied between 50% and 70% and we
partners, particularly in HIV-positive men and men who are unable to say how non-responders differed in risk. The
are at risk of transmission. Serosorting, which has demographic characteristics of the 13% of men who
increased substantially over the past 14 years, is a risky refused a test were broadly the same as men who did take
practice, particularly in HIV-negative men, because 3% a test, although we are unable to infer differences in HIV
(in 2013) of men who perceive themselves to be status. Also, the self-reported behaviour and testing data
HIV negative are HIV positive, inadvertently putting could be subject to recall bias. Furthermore, new web-
others at risk. We have identified and characterised a based or app-based methods to meet partners have become
subgroup at risk of transmitting infection, particularly increasingly popular,12 and MSM who use these services
undiagnosed men reporting UAI (one in 43 MSM) and a could differ from individuals visiting bars, clubs, and
larger group at risk of acquiring infection (one in five saunas. A study comparing MSM recruited to online and
HIV-negative MSM) in whom maintenance of the offline behavioural surveillance studies showed that
epidemic could be occurring. Because not all diagnosed individuals using web-based methods were younger, less
MSM are on treatment (69% in 2000 [Yin Z, Public likely to identify as gay, less likely to use condoms with
Health England, personal communication], 90% in 20132) casual partners, and less likely to be tested for HIV.13
and not all men on treatment have undetectable viral Additionally, London-based MSM might not be
loads (94% in 2013),2 a proportion of individuals representative of MSM in the UK; the estimated HIV
diagnosed reporting UAI and not exclusively serosorting prevalence in London is one in 11 MSM compared with
are also likely to be at risk of transmission. Furthermore, one in 28 in England and Wales outside London.14 However,
increased uptake of recent testing (in the past year), because of the low MSM population prevalence, it is not
combined with evidence of undiagnosed HIV-positive feasible to obtain a true probability sample. Unlike many
men who have recently tested negative, suggest that an convenience samples or internet samples, we did have a
increasing proportion of the undiagnosed men might clear sampling frame and calculated a response rate. Data
have been recently infected and could pose a high risk of from the National Survey of Sexual Attitudes and Lifestyles
transmission. (NATSAL) show that in 2000, 61·6% (95% CI 52·8–69·7)
This study examined long-term trends in undiagnosed of MSM had attended a gay club or bar in the past year, and
HIV, testing, UAI, serosorting, and partner numbers by in 2010, the proportion was 55% (44·7–64·9; Mercer C,
HIV status in MSM in London. We report on the changes UCL, personal communication). 77·5% (64·3–86·8) of gay
in behaviours and testing alongside other available MSM, had attended such venues in the past year.
information on testing and ART uptake.1,2 Some Comparison of data from MSM in convenience sample
HIV-positive individuals have been reported to change surveys and the 2010 NATSAL show that convenience
their behaviour shortly after diagnosis11 and we have sample surveys are likely to overestimate rates of sexually
presented differences in behaviour by HIV infection transmitted infection diagnoses and HIV testing, but that
status and further explore a large group of undiagnosed these differences are smaller in MSM who identify
MSM. Additionally, we were able to identify HIV-positive themselves as gay,15 which suggests that our findings
www.thelancet.com/hiv Vol 3 September 2016 e437
Articles
MSM potentially at risk of transmitting HIV* MSM at higher risk of acquiring HIV†
% (n/N)‡ OR (95% CI)§ AOR (95% CI)¶ % (n/N)‡ OR (95% CI)§ AOR (95% CI)¶
Age, years
16–24 3% (40/1583) 1 1 30% (469/1554) 1 1
25–34 5% (217/4735) 1·85 (1·32–2·60) 2·11 (1·45–3·08) 27% (1146/4317) 0·84 (0·74–0·95) 0·94 (0·79–1·12)
35–44 5% (195/3635) 2·19 (1·55–3·09) 2·67 (1·82–3·92) 24% (745/3090) 0·74 (0·64–0·85) 0·83 (0·69–1·00)
45–64 5% (70/1455) 1·94 (1·31–2·89) 2·55 (1·64–3·97) 20% (250/1245) 0·59 (0·49–0·70) 0·62 (0·49–0·80)
≥65 1% (1/82) 0·48 (0·06–3·50) 0·89 (0·11–7·21) 11% (9/80) 0·30 (14·6–59·6) 0·39 (0·15–1·04)
p value ·· 0·0002 <0·0001 ·· <0·0001 0·003
Ethnic origin
White 4% (434/9973) 1 1 25% (2269/8912) 1 ··
Black 12% (41/356) 2·86 (2·04–4·01) 2·60 (1·73–3·90) 26% (76/287) 1·06 (0·81–1·38) ··
Asian 3% (10/314) 0·72 (0·38–1·37) 0·83 (0·43–1·64) 24% (73/310) 0·90 (0·69–1·18) ··
Southeast Asian 2% (5/204) 0·55 (0·23–1·35) 0·71 (0·28–1·81) 18% (36/197) 0·65 (0·45–0·94) ··
Mixed/other 5% (36/689) 1·21 (0·85–1·71) 1·21 (0·82–1·79) 27% (168/628) 1·09 (0·90–1·31) ··
p value ·· <0·0001 0·0001 ·· 0·14 ··
Years education after age 16 years
None 5% (69/1325) 1 1 28% (314/1116) 1 1
Up to 2 years 6% (119/1888) 1·22 (0·90–1·66) 1·32 (0·94–1·85) 28% (459/1648) 0·99 (0·84–1·17) 0·91 (0·72–1·13)
3 years or more 4% (306/7459) 0·77 (0·59–1·01) 0·91 (0·68–1·23) 24% (1637/6741) 0·83 (0·72–0·95) 0·82 (0·68–0·99)
Still in full-time education 4% (30/820) 0·69 (0·44–1·06) 0·99 (0·60–1·63) 27% (213/779) 0·97 (0·79–1·19) 0·85 (0·64–1·14)
p value ·· 0·0002 0·03 ·· 0·003 0·18
Employed
No 6% (87/1508) 1 1 27% (342/1247) 1 1
Yes 4% (437/10 021) 0·75 (0·59–0·95) 0·97 (0·74–1·27) 25% (2289/9091) 0·89 (0·78–1·02) 1·02 (0·84–1·24)
p value ·· 0·011 0·81 ·· 0·09 0·96
Age at first anal intercourse <16 years
No 4% (410/9393) 1 1 26% (2176/8429) 1 1
Yes 8% (110/1463) 1·78 (1·43–2·22) 1·27 (1·00–1·63) 33% (406/1218) 1·44 (1·26–1·64) 1·11 (0·94–1·33)
p value ·· <0·0001 0·054 ·· <0·0001 0·42
Casual UAI partners in the past year
<2 2% (168/9264) 1 1 15% (1227/8380) ·· 1
2–5 11% (180/1633) 6·73 (5·42–8·37) 5·50 (4·37–6·91) 77% (1046/1360) 19·7 (17·1–22·7) 17·9 (15·4–20·9)
6–10 19% (64/343) 12·49 (9·15–17·06) 9·83 (7·08–13·64) 89% (218/245) 48·0 (32·0–71·9) 54·4 (33·3–88·8)
>10 35% (115/330) 29·29 (22·26–38·51) 21·77 (16·23–29·19) 92% (142/154) 70·2 (38·8–127·0) 69·8 (35·3–138·2)
p value ·· <0·0001 <0·0001 ·· <0·0001 <0·0001
Sexually transmitted infection in the past year
No 3% (321/9391) 1 1 23% (1938/8610) 1 1
Yes 10% (202/2083) 3·05 (2·54–3·67) 1·24 (0·99–1·55) 40% (671/1661) 2·32 (2·08–2·59) 1·43 (1·22–1·68)
p value ·· <0·0001 0·058 ·· <0·0001 <0·0001
Attended a genitourinary medicine clinic in the past year
No 2% (154/6199) 1 1 21% (1275/5937) 1 1
Yes 7% (367/5256) 2·97 (2·45–3·60) 1·81 (1·45–2·26) 31% (1330/4327) 1·65 (1·50–1·80) 1·10 (0·97–1·25)
p value ·· <0·0001 <0·0001 ·· <0·0001 0·12
Percentages might not add up to totals because of rounding. MSM=men who have sex with men. UAI=unprotected anal intercourse. OR=odds ratio. AOR=adjusted odds ratio. NA=not applicable. *Includes MSM
with undiagnosed HIV who reported UAI in the past year and MSM with diagnosed HIV who reported UAI and not exclusively serosorting in the past year, compared with all other MSM. †Includes HIV-negative
MSM who either report one or more UAI casual partners or not exclusively serosorting in the past year, compared with all other HIV-negative MSM. ‡Denominators vary because of incomplete data on all
variables. §Adjusted for age and year of survey. ¶Multivariable model includes variables that were significant (ie, p<0·05) in the univariable analysis.
Table 4: Factors associated with potential risk of transmitting and high risk of acquiring HIV in MSM, 2000–13 data combined
might be generalisable to MSM who identify as gay. By disclosed their status, which could potentially have inflated
obtaining trends from similar venues over an extended our estimate of undiagnosed participants. However, we
timeframe, we were able to make comparisons over time. believe non-disclosure was kept to a minimum because
Lastly, some participants might not have accurately the self-completed survey was entirely anonymous.
e438 www.thelancet.com/hiv Vol 3 September 2016
Articles
To our knowledge, few UK studies exist that examine Community-level interventions in settings such as bars,
trends in sexual behaviours in MSM in the community clubs, and saunas have been shown to be successful.25
by HIV status, and none that have reported trends in Furthermore, self-sampling and self-testing are
MSM partner numbers in detail by HIV transmission acceptable to MSM26 and now available in the UK, which
risk. Most are cross-sectional data from earlier rounds could promote testing at more regular intervals, and
of surveys included in this study.10,16,17 In a study of would be important in earlier detection of infection to
sexual behaviour of gay men who used gyms in London reduce transmission, particularly in men who do not
between 1998 and 2008, Lattimore and colleagues18 attend sexual health clinics often. Anecdotal evidence
found a lower proportion of MSM reporting UAI (37%) suggests that an increase in new diagnoses and infections
than we did (50% in 2008), but also an increase in UAI in London1 could also partly be attributable to other
with partners of the same status, particularly in behaviours not studied here, such as an increase in
HIV-negative MSM, from 12% in 1998 to 21% in 2008. recreational drug use.27 MSM attending the central
A study by McDaid and colleagues19 on serosorting and London CODE clinic (a clinic that specialises in sexual
strategic positioning during UAI in MSM in Scotland health for men who use drugs for sex—chemsex) prefer
found that, although these behaviours were occurring to use internet sites and apps that specialise in
(in 11% of HIV-positive and 13% of negative MSM in barebacking (the common term for UAI) to find partners,
2008), they were inconsistently performed. Both of with an average of five partners per encounter.27 Further
these studies found increased HIV testing (ever and work is needed to design interventions that reach the
recent) in MSM. Continuing high levels of undiagnosed users of these sites.
infection in MSM in the community have also been Although HIV testing is increasing1 and the coverage
reported in Scotland—25% of HIV-positive MSM in of ART is high in people diagnosed, the prevalence of
Scotland were undiagnosed in 2011.20 Notably, the high-risk behaviours in MSM visiting gay social venues
characteristics of HIV epidemics in MSM in several remains high. Treatment as prevention strategies alone
other countries are similar to that in the UK. For are unlikely to have a substantial effect on HIV incidence
example, reports show that despite increases in ART in the UK because of transmission from men with
coverage and testing, transmission in France and the primary infection and undiagnosed cases.28 We have
USA is sustained at a high level,21,22 probably because of shown here that a large proportion of undiagnosed
increased risk behaviours similar to those shown in infections are now recently acquired infections and
this study. some of these infections are probably primary infections.
This study emphasises the importance of core groups Additionally, modelling studies have found the
in the epidemiology and control of HIV infection in the epidemiological effect of earlier diagnosis and treatment
MSM community in the UK. The data show changes in to be offset by increases in risk behaviours.29,30 Pre-
sexual risk behaviours of MSM in London over the past exposure prophylaxis (PrEP) might help prevent
14 years with more reporting UAI and an increase in outbreaks. However, PrEP relies on MSM perceiving
serosorting as a risk reduction strategy. As expected, themselves at risk and choosing to test. In our study, a
distinct differences in risk behaviours of MSM by HIV third of undiagnosed MSM had not been tested in the
status exist, with HIV-positive men describing the past year. Finally, serosorting, in which the status of the
highest risk. A subgroup of these men are infectious, partner is presumed, is unsafe because of incorrect
particularly those who are undiagnosed. Coupled with perception of serostatus. Thus, public health authorities
high partner numbers and the one in five HIV-negative urgently need to focus on implementing and evaluating
men at high risk of acquisition, this subgroup of men are combined behavioural and biomedical interventions
likely to disproportionately be the drivers of the sustained (such as test-and-treat and PrEP programmes) that focus
incidence over the past decade. The benefits of on the group of men potentially at risk of HIV
serosorting might be outweighed by increased partner transmission and HIV-negative men with behavioural
numbers, inconsistent practice, and incorrect perceived patterns that put them at high risk of acquisition. The
serostatus, as shown by the high proportion of social and cultural mixing of these groups will need to
undiagnosed men who incorrectly perceive their HIV be considered as part of the design of risk reduction
status as negative. Additionally, the rise in testing rates strategies (eg, targeting of younger MSM who might be
in undiagnosed men suggests these infections are less aware of the risks and less able to protect
increasingly recently acquired, when people might be themselves). The findings presented in this Article are
most infectious. an important contribution to the growing evidence that
Modelling studies have shown that reducing the testing and treatment strategies alone are not sufficient
number of undiagnosed infections and subsequently to reduce HIV incidence at the population level.
treating these individuals will have the greatest effect on Combination prevention working closely with affected
HIV incidence.23,24 Undiagnosed HIV infection is communities to reduce community-wide risk by both
prevalent in the MSM community, particularly in saunas behavioural and biological interventions is crucial if we
where nearly one in ten men were undiagnosed. are to move towards eradication of HIV.
www.thelancet.com/hiv Vol 3 September 2016 e439
Articles
Contributors 15 Prah P, Hickson F, Bonell C, et al. Men who have sex with men in
All authors contributed to the design of the study. AA and SW analysed Great Britain: comparing methods and estimates from probability
the data and drafted the manuscript. All authors commented on drafts of and convenience sample surveys. Sex Transm Infect 2016; published
the manuscript and approved the final version. online March 10. DOI:10.1136/sextrans-2015-052389.
16 Dodds JP, Johnson AM, Parry JV, Mercey DE. A tale of three cities:
Declaration of interests persisting high HIV prevalence, risk behaviour and undiagnosed
We declare no competing interests. infection in community samples of men who have sex with men.
Sex Transm Infect 2014; 83: 392–96.
Acknowledgments
This study was funded by Public Health England. We thank 17 Williamson LM, Dood JP, Mercey DE, Johnson AM, Hart GJ.
Increases in HIV-related sexual risk behavior among community
Gary Murphy and Bharati Patel for doing the laboratory testing,
samples of gay men in London and Glasgow: how do they compare?
Catherine Mercer for providing the NATSAL statistics, Zheng Yin for
J Acquir Immune Defic Syndr 2006; 42: 238–41.
providing data on proportion of diagnosed men on antiretroviral therapy
18 Lattimore S, Thornton A, Delpech V, Elford J. Changing patterns of
with detectable viral load in 2000, and all participants for their valuable
sexual risk behavior among London gay men: 1998–2008.
contributions. Sex Transm Dis 2011; 38: 221–29.
References 19 McDaid LM, Hart GJ. Serosorting and strategic positioning during
1 Aghaizu A, Brown AE, Nardone A, et al. HIV in the United Kingdom unprotected anal intercourse: are risk reduction strategies being
2013 report: data to end 2012. London: Public Health England, 2013. employed by gay and bisexual men in Scotland? Sex Transm Dis
2 Public Health England. National HIV surveillance data tables. 2013; 39: 735–38.
London: Public Health England, 2013. 20 Wallace LA, Li J, McDaid LM. HIV prevalence and undiagnosed
3 Birrell PJ, Gill ON, Delpech VC, et al. HIV incidence in men who infection among a community sample of gay and bisexual men in
have sex with men in England and Wales 2001–10: a nationwide Scotland, 2005–2011: implications for HIV testing policy and
population study. Lancet Infect Dis 2013; 13: 313–18. prevention. PLoS One 2014; 9: e90805.
4 Phillips AN, Cambiano V, Nakagawa F, et al. Increased HIV 21 Prejean J, Song R, Hernandez A, et al. Estimated HIV incidence in
incidence in men who have sex with men despite high levels of the United States, 2006–2009. PLoS One 2011; 6: e17502.
ART-Induced viral suppression: analysis of an extensively 22 Le Vu S, Le Strat Y, Barin F, et al. Population-based HIV-1 incidence
documented epidemic. PLoS One 2013; 8: e55312. in France, 2003–08: a modelling analysis. Lancet Infect Dis 2010;
5 Elford J. Changing patterns of sexual behaviour in the era of highly 10: 682–87.
active antiretroviral therapy. Curr Opin Infect Dis 2006; 19: 26–32. 23 Marks G, Crepaz N, Janssen RS. Estimating sexual transmission of
6 Crepaz N, Hart TA, Marks G. Highly active antiretroviral therapy HIV from persons aware and unaware that they are infected with
and sexual risk behavior: a meta-analytic review. JAMA 2004; the virus in the USA. AIDS 2006; 26: 1447–50.
292: 224–36. 24 Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG.
7 Elford J. HIV treatment optimism and high-risk sexual behaviour Universal voluntary HIV testing with immediate antiretroviral
among gay men: the attributable population risk. AIDS 2016; therapy as a strategy for elimination of HIV transmission:
18: 2216–17. a mathematical model. Lancet 2009; 373: 48–57.
8 British HIV Association, British Association of Sexual Health and 25 Godin G, Naccache H, Cote F, Leclerc R, Frechette M, Alary M.
HIV, British Infection Society. UK national guidelines for HIV Promotion of safe sex: evaluation of a community-level intervention
testing 2008. London: British HIV Association, 2008. programme in gay bars, saunas and sex shops. Health Educ Res
2008; 23: 287–97.
9 Aghaizu A, Mercey D, Copas A, et al. Who would use PrEP?
Factors associated with intention to use among MSM in London: 26 Wayal S, Llewellyn C, Smith H, et al. Self-sampling for
a community survey. Sex Transm Infect 2013; 89: 207–11. oropharyngeal and rectal specimens to screen for sexually
transmitted infections: acceptability among men who have sex with
10 Dodds JP, Mercey DE, Parry JV, Johnson AM. Increasing risk
men. Sex Transm Infect 2015; 85: 60–64.
behaviour and high levels of undiagnosed HIV infection in a
community sample of homosexual men. Sex Transm Infect 2004; 27 Kirby T, Thornber-Dunwell M. High-risk drug practices tighten grip
80: 236–40. on London gay scene. Lancet 2013; 381: 101–02.
11 Fox J, White PJ, MacDonald N, et al. Reductions in HIV 28 Brown AE, Nardone A, Delpech VC. WHO “Treatment as
transmission risk behaviour following diagnosis of primary HIV Prevention” guidelines are unlikely to decrease HIV transmission
infection: a cohort of high-risk men who have sex with men. in the UK unless undiagnosed HIV infections are reduced.
HIV Med 2009; 17: 432–38. AIDS 2014; 28: 281–83.
12 Bolding G, Davis M, Hart G, Sherr L, Elford J. Where young MSM 29 van Sighem A, Vidondo B, Glass T, et al. Resurgence of HIV
meet their first sexual partner: the role of the Internet. AIDS Behav infection among men who have sex with men in switzerland:
2007; 11: 522–26. mathematical modelling study. PLoS One 2012; 7: e44819.
13 Saxton P, Dickson N, Hughes A. Who is omitted from repeated 30 Bezemer D, de Wolf F, Boerlijst MC, et al. 27 years of the HIV
offline HIV behavioural surveillance among MSM? Implications for epidemic amongst men having sex with men in the Netherlands: an in
interpreting trends. AIDS Behav 2013; 17: 3133–44. depth mathematical model-based analysis. Epidemics 2010; 2: 66–79.
14 Skingsley A, Yin Z, Kirwan P, et al. HIV in the UK: situation report
2015. Incidence, prevalence and prevention. London: Public Health
England, 2015.
e440 www.thelancet.com/hiv Vol 3 September 2016
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Efficacyand Safetyof Propranololvs Atenololin Infants With Problematic Infantile Hemangiomas ARandomized Clinical TrialDocument10 pagesEfficacyand Safetyof Propranololvs Atenololin Infants With Problematic Infantile Hemangiomas ARandomized Clinical TrialJuan Carlos Riveros MedinaNo ratings yet
- Noninferiority and Safety of Nadolol Vs PropranoloDocument8 pagesNoninferiority and Safety of Nadolol Vs PropranoloJuan Carlos Riveros MedinaNo ratings yet
- Jamadermatology Kim 2017 Oi 170008Document8 pagesJamadermatology Kim 2017 Oi 170008Juan Carlos Riveros MedinaNo ratings yet
- IM2C Sample Problem EvacuatingDocument2 pagesIM2C Sample Problem EvacuatingJuan Carlos Riveros MedinaNo ratings yet
- BOPV SIA2024 OrientationDocument36 pagesBOPV SIA2024 OrientationFranz SalazarNo ratings yet
- 6 Public Health Issues To Know in 2023 + Jobs Tackling Them - CourseraDocument6 pages6 Public Health Issues To Know in 2023 + Jobs Tackling Them - CourseraUdaai NairNo ratings yet
- Comprehensive Review Of Infectious Diseases 1St Edition Andrej Spec full chapter pdf docxDocument69 pagesComprehensive Review Of Infectious Diseases 1St Edition Andrej Spec full chapter pdf docxjeydeltaive100% (5)
- HIV Self Testing Register - CF 002Document1 pageHIV Self Testing Register - CF 002leon FrankNo ratings yet
- Artikel History: Literature Review: Evaluasi Ragam Metode PerawatanDocument13 pagesArtikel History: Literature Review: Evaluasi Ragam Metode PerawatanFanny VenezuelaNo ratings yet
- Mycoplasma GallicepticumDocument18 pagesMycoplasma GallicepticumRoni FaturrahmanNo ratings yet
- Molluscum Contagiosum An Update and Review of Prespectives Etiology, Diagnosis, and Treatment PDFDocument9 pagesMolluscum Contagiosum An Update and Review of Prespectives Etiology, Diagnosis, and Treatment PDFLaras KinasihNo ratings yet
- Aids 2022Document27 pagesAids 2022Nikhil BijuNo ratings yet
- Jurnal Hiv Aids 2Document10 pagesJurnal Hiv Aids 2Anonymous j0xAgHs3No ratings yet
- Chirorab Prescribing InformationDocument2 pagesChirorab Prescribing Informationsr bNo ratings yet
- Intravenous ImmunoglobulinDocument5 pagesIntravenous ImmunoglobulinTeslim RajiNo ratings yet
- Development and Validation of A Sociodemographic ADocument14 pagesDevelopment and Validation of A Sociodemographic AvusNo ratings yet
- Overview of Global HIVDocument27 pagesOverview of Global HIVAhmed AdemNo ratings yet
- ICD-10-CM For Physicians 2018 Chapter Guidelines and Examples PDFDocument48 pagesICD-10-CM For Physicians 2018 Chapter Guidelines and Examples PDFRachelle AbuzoNo ratings yet
- Health 8 DEPED PDFDocument74 pagesHealth 8 DEPED PDFRuel LaguitanNo ratings yet
- UNIT 1 - PathophysiologyDocument8 pagesUNIT 1 - PathophysiologyEricBuguinaNo ratings yet
- DR Siobhan Crowley Paediatric & Family HIV Care World Heath Organization, Email: Crowleys@who - IntDocument17 pagesDR Siobhan Crowley Paediatric & Family HIV Care World Heath Organization, Email: Crowleys@who - IntYabetsNo ratings yet
- Kendigs Disorders of The Respiratory Tract in Children 9Th Edition Robert W Wilmott Full ChapterDocument50 pagesKendigs Disorders of The Respiratory Tract in Children 9Th Edition Robert W Wilmott Full Chapterernest.guzman635100% (6)
- Blueprints - Pediatric Infectious Diseases PDFDocument140 pagesBlueprints - Pediatric Infectious Diseases PDFHabu John Kocu100% (1)
- 6 - Immune Deficiency Diseases 2Document8 pages6 - Immune Deficiency Diseases 2Belle Galao GepteNo ratings yet
- Prevalence of Hypoalbuminemia in Outpatients With HIV/AIDS: ArticleDocument5 pagesPrevalence of Hypoalbuminemia in Outpatients With HIV/AIDS: ArticleMUHAMMAD BAGIR ALJUFRINo ratings yet
- Activities: Republic The PhilippinesDocument13 pagesActivities: Republic The Philippineseijul0708No ratings yet
- Survey DesignDocument66 pagesSurvey DesignAbdul HadiNo ratings yet
- Essential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinDocument54 pagesEssential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinYostesara Maurena SantosaNo ratings yet
- Hiv Testing in The Era of Prep:: When The Tests Are DiscordantDocument17 pagesHiv Testing in The Era of Prep:: When The Tests Are DiscordantAldren GilanaNo ratings yet
- Sudan ProfileDocument19 pagesSudan ProfileTsaalits MuharrorohNo ratings yet
- Pastors GB 20041Document70 pagesPastors GB 20041shedzaNo ratings yet
- HIV and AIDS NOTESDocument4 pagesHIV and AIDS NOTESTariro TaringaNo ratings yet
- Apartheid Study Guide-1Document9 pagesApartheid Study Guide-1api-233191821No ratings yet
- Life Cycle of Leishmania SPDocument3 pagesLife Cycle of Leishmania SPUttam Kr PatraNo ratings yet