You might also like
- Reality Therapy: A New Approach to PsychiatryFrom EverandReality Therapy: A New Approach to PsychiatryRating: 3.5 out of 5 stars3.5/5 (31)
- Astm D 2979 PDFDocument3 pagesAstm D 2979 PDFMiftahulArifNo ratings yet
- INCOMPATIBILITIESDocument27 pagesINCOMPATIBILITIESArk Olfato Parojinog100% (1)
- Diagnosis - Reflective EssayDocument3 pagesDiagnosis - Reflective EssayConnor JefferiesNo ratings yet
- Classroom of The Elite Vol. 8Document244 pagesClassroom of The Elite Vol. 8Rahul Lakra85% (13)
- Aggressivity, Narcissism, and Self-Destructiveness in The Psychotherapeutic Relationship - Otto KernbergDocument27 pagesAggressivity, Narcissism, and Self-Destructiveness in The Psychotherapeutic Relationship - Otto Kernbergvgimbe100% (1)
- Research Paper Antisocial Personality DisorderDocument4 pagesResearch Paper Antisocial Personality Disorderhpdqjkwgf100% (1)
- Classification of Behaviour and Experience in Relation To Functional Psychiatric Diagnoses-Time For A Paradigm ShiftDocument12 pagesClassification of Behaviour and Experience in Relation To Functional Psychiatric Diagnoses-Time For A Paradigm ShiftJaime Iván Hernández España100% (2)
- Psychodynamic Diagnostic Manual 2nd Edition PDDocument3 pagesPsychodynamic Diagnostic Manual 2nd Edition PDgustiNo ratings yet
- Personality DisorderDocument33 pagesPersonality DisorderIulia Moldovan100% (1)
- PCS-9613S X DataSheet en Overseas General X R1.10Document57 pagesPCS-9613S X DataSheet en Overseas General X R1.10parveen115No ratings yet
- CAPE Unit 2 Pure Maths NotesDocument103 pagesCAPE Unit 2 Pure Maths NotesAltrupassionate girlNo ratings yet
- Quantitative School of ManagementDocument3 pagesQuantitative School of ManagementVAIBHAV JAIN100% (1)
- Experiment 5: Resistors in Series and Parallel CircuitsDocument2 pagesExperiment 5: Resistors in Series and Parallel CircuitsVictoria De GuzmanNo ratings yet
- A Level Pure Unit 7 Parametric Equations QPDocument2 pagesA Level Pure Unit 7 Parametric Equations QPsaNo ratings yet
- Week 3 Forecasting HomeworkDocument4 pagesWeek 3 Forecasting HomeworkMargot LaGrandNo ratings yet
- YR7 Revision Sheet - Working ScietificallyDocument6 pagesYR7 Revision Sheet - Working ScietificallyNisha zehra100% (1)
- Subjectivity and Intersubjectivity in Psuchiatric Diagnosis - FUCHSDocument7 pagesSubjectivity and Intersubjectivity in Psuchiatric Diagnosis - FUCHSmariana puchivailoNo ratings yet
- Examples of Antisocial Personality Disorder Research PaperDocument7 pagesExamples of Antisocial Personality Disorder Research Paperefeq3hd0No ratings yet
- VienproofsDocument22 pagesVienproofsAlfredo Martin Blasco CabreraNo ratings yet
- Categorical and Dimensional Models of Pathological Narcissism, The Case ofDocument11 pagesCategorical and Dimensional Models of Pathological Narcissism, The Case ofjuaromerNo ratings yet
- Preserving The Person in Contemporary Psychiatry: Glen O. GabbardDocument9 pagesPreserving The Person in Contemporary Psychiatry: Glen O. GabbardmkecikNo ratings yet
- Contemporary Psychiatry 2018 PDFDocument9 pagesContemporary Psychiatry 2018 PDFDhino Armand Quispe SánchezNo ratings yet
- 20th Anniversary Issue: Can Psychopathology and Neuroscience Coexist in Psychiatric Classifications?Document7 pages20th Anniversary Issue: Can Psychopathology and Neuroscience Coexist in Psychiatric Classifications?Sahâmia MartinsNo ratings yet
- Skee M Backgr Paper 12Document14 pagesSkee M Backgr Paper 12GERMÁN ANDRÉS GUEVARANo ratings yet
- Psychotherapy For Borderline Personality FocusingDocument3 pagesPsychotherapy For Borderline Personality FocusingjoannaNo ratings yet
- Diagnosing PsychopathyDocument27 pagesDiagnosing PsychopathyAnas HamamNo ratings yet
- Antisocial Personality Disorder Research Paper OutlineDocument7 pagesAntisocial Personality Disorder Research Paper OutlinetozvnfvndNo ratings yet
- Taking Subjectivity Seriously: Towards A Uni Fication of Phenomenology, Psychiatry, and NeuroscienceDocument7 pagesTaking Subjectivity Seriously: Towards A Uni Fication of Phenomenology, Psychiatry, and NeurosciencealexandracastellanosgoNo ratings yet
- Jorge Arthur Brinkely, 2001Document18 pagesJorge Arthur Brinkely, 2001Deivson Filipe BarrosNo ratings yet
- A CritiqueDocument9 pagesA Critiquewangarichristine12No ratings yet
- The Role of Identity in The DSM-5 Classification of Personality DisordersDocument11 pagesThe Role of Identity in The DSM-5 Classification of Personality DisordersJosé Ignacio SáezNo ratings yet
- An Object-Relations Based Model For The Assessment of Borderline PsychopathologyDocument17 pagesAn Object-Relations Based Model For The Assessment of Borderline Psychopathologyracm89No ratings yet
- Otto Kemberg - Diagnóstico Estructural de La PersonalidadDocument13 pagesOtto Kemberg - Diagnóstico Estructural de La PersonalidadEfecto AlmaNo ratings yet
- Integrating Clinical Staging and Phenomenological Psychopathology To Add Depth, Nuance and Utility To Clinical Phenotyping: A Heuristic ChallengeDocument20 pagesIntegrating Clinical Staging and Phenomenological Psychopathology To Add Depth, Nuance and Utility To Clinical Phenotyping: A Heuristic ChallengeAnastasiya PlohihNo ratings yet
- Psychopathy: Theory, Measurement, and TreatmentDocument20 pagesPsychopathy: Theory, Measurement, and TreatmentMira MNo ratings yet
- Deconstructing PsychosisDocument8 pagesDeconstructing PsychosisEvets DesouzaNo ratings yet
- The Psychodynamic Diagnostic ManualDocument3 pagesThe Psychodynamic Diagnostic ManualJrtabletsmsHopeNo ratings yet
- The Durand Adaptive Psychopathic Traits Questionnaire Development and ValidationDocument11 pagesThe Durand Adaptive Psychopathic Traits Questionnaire Development and ValidationKusuma PutriNo ratings yet
- Can We Predict Psychosis Outside The Clinical High-Risk State? A Systematic Review of Non-Psychotic Risk Syndromes For Mental DisordersDocument10 pagesCan We Predict Psychosis Outside The Clinical High-Risk State? A Systematic Review of Non-Psychotic Risk Syndromes For Mental DisordersRubiNo ratings yet
- PDF 65750 81433Document13 pagesPDF 65750 81433Viktor NassifNo ratings yet
- Hopwood 2018 Interpersonal Dynamics in Personality and Personality DisordersDocument26 pagesHopwood 2018 Interpersonal Dynamics in Personality and Personality Disordersbramantika.oktaviantiNo ratings yet
- Ruggero Ea (2019) HiTOP in Clinical Practice. JrnConsClinPsycDocument30 pagesRuggero Ea (2019) HiTOP in Clinical Practice. JrnConsClinPsycFeras ZidiNo ratings yet
- 10 1111@inm 12737Document10 pages10 1111@inm 12737Joaquin OlivaresNo ratings yet
- Skeem Et Al (2011) Psychopathy ReviewDocument68 pagesSkeem Et Al (2011) Psychopathy ReviewJulian KorfineNo ratings yet
- A Broader View of PsychopathyDocument9 pagesA Broader View of PsychopathyMAN HIM HONo ratings yet
- Kanfer 1965Document10 pagesKanfer 1965Erika Lorena Soto PadillaNo ratings yet
- An Overview of The DSM-5 Alternative Model of Personality DisordersDocument7 pagesAn Overview of The DSM-5 Alternative Model of Personality DisordersJosé Ignacio SáezNo ratings yet
- Psychiatrization of Society A Conceptual FrameworkDocument11 pagesPsychiatrization of Society A Conceptual Frameworkcoletivo peripatetikosNo ratings yet
- Psychiatry Research: Kate Allsopp, John Read, Rhiannon Corcoran, Peter Kinderman TDocument8 pagesPsychiatry Research: Kate Allsopp, John Read, Rhiannon Corcoran, Peter Kinderman TMaria Mendez RodriguezNo ratings yet
- The Treatment of Schizoid Personality Disorder Using Psychodynamic MethodsDocument25 pagesThe Treatment of Schizoid Personality Disorder Using Psychodynamic MethodsnikhilNo ratings yet
- Modul CLPDocument80 pagesModul CLPAndrio PalayukanNo ratings yet
- Waugh 2017Document22 pagesWaugh 2017Stella ÁgostonNo ratings yet
- tmp4D8B TMPDocument2 pagestmp4D8B TMPFrontiersNo ratings yet
- 1 s2.0 S0140673612612689 MainDocument3 pages1 s2.0 S0140673612612689 MainOana OrosNo ratings yet
- Phylosophy of Clinical Psychopharmacology PDFDocument7 pagesPhylosophy of Clinical Psychopharmacology PDFAvengingBrainNo ratings yet
- Otto Kernberg Aggresivity Narcissism PDFDocument27 pagesOtto Kernberg Aggresivity Narcissism PDFNillintheblanks100% (2)
- Psychology - Syllabus and Keynotes of Psychopathology For PG 2nd Semester Session 2018-20Document13 pagesPsychology - Syllabus and Keynotes of Psychopathology For PG 2nd Semester Session 2018-20abhi_kr84No ratings yet
- Clarifying The Heterogeneity in Psychopathic Samples Towards A New CoDocument120 pagesClarifying The Heterogeneity in Psychopathic Samples Towards A New CoMarli LimaNo ratings yet
- Clinical Research: Patient-Reported Outcomes in Borderline Personality DisorderDocument12 pagesClinical Research: Patient-Reported Outcomes in Borderline Personality DisorderMomeneo NeoNo ratings yet
- Disfunkcionalna Uverenja I Ant PLDocument12 pagesDisfunkcionalna Uverenja I Ant PLNađa FilipovićNo ratings yet
- The Psychopath MagnetizedDocument9 pagesThe Psychopath MagnetizedAvengingBrainNo ratings yet
- Hierarchical Taxonomy of Psychopathology (HiTOP) - Kotov, 2018Document2 pagesHierarchical Taxonomy of Psychopathology (HiTOP) - Kotov, 2018Hugo UrquinaNo ratings yet
- Texto Psicopatía 1Document9 pagesTexto Psicopatía 1Gonzalo Araya GómezNo ratings yet
- Diagnosis in PsychoanalysisDocument14 pagesDiagnosis in PsychoanalysisFrancesca Bonfanti CasareggioNo ratings yet
- World Psychiatry - 2022 - Stein - Psychiatric Diagnosis and Treatment in The 21st Century Paradigm Shifts VersusDocument22 pagesWorld Psychiatry - 2022 - Stein - Psychiatric Diagnosis and Treatment in The 21st Century Paradigm Shifts VersusLucas DistelNo ratings yet
- Depression Conceptualization and Treatment: Dialogues from Psychodynamic and Cognitive Behavioral PerspectivesFrom EverandDepression Conceptualization and Treatment: Dialogues from Psychodynamic and Cognitive Behavioral PerspectivesChristos CharisNo ratings yet
- Dimensional PsychopathologyFrom EverandDimensional PsychopathologyMassimo BiondiNo ratings yet
- Somatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy PerspectivesFrom EverandSomatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy PerspectivesChristos CharisNo ratings yet
- Temperament Traits and Personality Disorders. Predictors For Personality DisordersDocument12 pagesTemperament Traits and Personality Disorders. Predictors For Personality DisordersDiyan ayu SalsabelaNo ratings yet
- Antisocial Personality Disorder: November 2019Document9 pagesAntisocial Personality Disorder: November 2019Diyan ayu SalsabelaNo ratings yet
- Pain Management in Trauma: A Review Study: Journal of Injury & Violence Research July 2016Document11 pagesPain Management in Trauma: A Review Study: Journal of Injury & Violence Research July 2016Diyan ayu SalsabelaNo ratings yet
- Pain Management in Trauma Patients Affected by The.98341Document41 pagesPain Management in Trauma Patients Affected by The.98341Diyan ayu SalsabelaNo ratings yet
- Genomic and CDNA LibrariesDocument15 pagesGenomic and CDNA LibrariesPrabhleen KaurNo ratings yet
- Engineering Physics - PHY 1701 N. Punithavelan, Assistant Professor, Physics Division, VIT-ChennaiDocument6 pagesEngineering Physics - PHY 1701 N. Punithavelan, Assistant Professor, Physics Division, VIT-ChennaiRamyasai MunnangiNo ratings yet
- VedicReport7 25 20213 48 52PMDocument55 pagesVedicReport7 25 20213 48 52PMAbhishek BiswalNo ratings yet
- LEPTOSPIRADocument31 pagesLEPTOSPIRADinar NastitiNo ratings yet
- AaaaaDocument3 pagesAaaaaAnonymous C3BD7OdNo ratings yet
- Afa 7&8Document11 pagesAfa 7&8APMNo ratings yet
- Topic 2.9 WorksheetDocument3 pagesTopic 2.9 WorksheethaniaNo ratings yet
- Humanistic TheoryDocument28 pagesHumanistic TheoryNano KaNo ratings yet
- Chapter 2 PDFDocument21 pagesChapter 2 PDFMahdi BanjakNo ratings yet
- English Solved SP3Document6 pagesEnglish Solved SP3Prem PatelNo ratings yet
- Split Valuation SAPDocument7 pagesSplit Valuation SAPPramod ShettyNo ratings yet
- I Learned Chapter 8-The Power of GuidanceDocument1 pageI Learned Chapter 8-The Power of Guidanceapi-295870335No ratings yet
- Heat Transfer in Internal Combustion Engines: 85-WA/HT-23Document7 pagesHeat Transfer in Internal Combustion Engines: 85-WA/HT-23muhammad basitNo ratings yet
- One-Dimensional Unconstrained Optimization: Example 1 Golden Section MethodDocument5 pagesOne-Dimensional Unconstrained Optimization: Example 1 Golden Section MethodMohamed MuayidNo ratings yet
- A Summary of The Theories or Concepts About Child Development From Piaget, Vygotsky, Brunner, and Gardner-Zahra Warda Mufidah 183221217Document16 pagesA Summary of The Theories or Concepts About Child Development From Piaget, Vygotsky, Brunner, and Gardner-Zahra Warda Mufidah 183221217Fida100% (1)
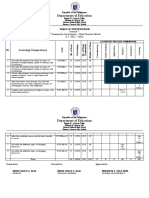
- Department of Education: Learning CompetencyDocument2 pagesDepartment of Education: Learning CompetencyShaira May Tangonan CaragNo ratings yet
- Engineering Thought Intelligence Fictional Intellectual Behave Exercise 1 ComputationDocument4 pagesEngineering Thought Intelligence Fictional Intellectual Behave Exercise 1 Computationposgas aceNo ratings yet
- Rosela Rowell, Carlos Rodriguez, Mark Salpeter, Chet Michals, Sarah KiddDocument5 pagesRosela Rowell, Carlos Rodriguez, Mark Salpeter, Chet Michals, Sarah KiddRosela De Jesus RowellNo ratings yet
- Presentation by SHIVAM SHAHDocument23 pagesPresentation by SHIVAM SHAHmikojiNo ratings yet
- Generative NLP Robert Dilts PDFDocument11 pagesGenerative NLP Robert Dilts PDFCristina LorinczNo ratings yet