You might also like
- Concept Map of CellulitisDocument8 pagesConcept Map of CellulitisReese Anne100% (1)
- Full Download Basic Immunology Functions and Disorders of The Immune System 4th Edition Abbas Test BankDocument36 pagesFull Download Basic Immunology Functions and Disorders of The Immune System 4th Edition Abbas Test Bankpasakazinum100% (34)
- Mock Outbreak Exercise: M. Serra Biol 2420 Lab Report 11 Student NameDocument3 pagesMock Outbreak Exercise: M. Serra Biol 2420 Lab Report 11 Student NameDennis MuthusiNo ratings yet
- Aflds White Paper: Covid-19: Experimental Vaccine CandidatesDocument35 pagesAflds White Paper: Covid-19: Experimental Vaccine CandidatesfabioNo ratings yet
- Hla TypingDocument23 pagesHla Typingandri perdanaNo ratings yet
- Sesi 1 - DR - Umi - Imunologi Transfusi DarahDocument46 pagesSesi 1 - DR - Umi - Imunologi Transfusi DarahWanda RyNo ratings yet
- Spring 2023 Lesson 28 The Immune System IIDocument38 pagesSpring 2023 Lesson 28 The Immune System IIClive AnnanNo ratings yet
- Glossary of Immunology Terms: Study Online atDocument12 pagesGlossary of Immunology Terms: Study Online atKurdii LaraNo ratings yet
- Linfocitos B y T-DepuratedDocument18 pagesLinfocitos B y T-DepuratedByron Emerson Gonzales GonzalesNo ratings yet
- Fundamentals of Immunology (Updated)Document59 pagesFundamentals of Immunology (Updated)Marydith OrtilloNo ratings yet
- Diseases of ImmunityDocument85 pagesDiseases of ImmunityOsama SaidatNo ratings yet
- How Do B Cells Produce Antibodies?Document165 pagesHow Do B Cells Produce Antibodies?Sharmaine TrangiaNo ratings yet
- Adaptive ImmunityDocument34 pagesAdaptive ImmunityMohamed Mido100% (1)
- Lecture 1moninfect ImmuDocument50 pagesLecture 1moninfect ImmuFrancisco HenriquezNo ratings yet
- 12 TransplantationDocument137 pages12 TransplantationLee BoborasNo ratings yet
- HAT HAS TO Happen TO Clear A Viral InfectionDocument57 pagesHAT HAS TO Happen TO Clear A Viral InfectionStella Michelle XuNo ratings yet
- Basic Immunology: Presented By-Dr. Prachi MulayDocument42 pagesBasic Immunology: Presented By-Dr. Prachi MulayPrachi MulayNo ratings yet
- 08 ImmunopathologyDocument118 pages08 ImmunopathologySteven Mark MananguNo ratings yet
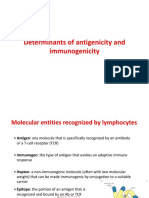
- Determinants of Antigenicity and ImmunogenicityDocument20 pagesDeterminants of Antigenicity and ImmunogenicitypowekNo ratings yet
- Adaptive Immune SystemDocument28 pagesAdaptive Immune SystemRiana AgathaNo ratings yet
- Day 3 IMMUNOLOGY-January 2021Document159 pagesDay 3 IMMUNOLOGY-January 2021ShriefElghazalyNo ratings yet
- IMMUNOLOGYDocument48 pagesIMMUNOLOGYIqbalmia911No ratings yet
- Activation of Adaptive ImmunityDocument19 pagesActivation of Adaptive ImmunityUtomo BudidarmoNo ratings yet
- 8 - Transplantation ImmunologyDocument60 pages8 - Transplantation Immunologymohammed barwaryNo ratings yet
- Adaptive Immunity II - Humoral ImmunityDocument29 pagesAdaptive Immunity II - Humoral Immunityxfxw5m5bczNo ratings yet
- B CELLS SeminarDocument81 pagesB CELLS SeminarviolaNo ratings yet
- PKB-immunology - II AntigensDocument42 pagesPKB-immunology - II AntigensSounak MandalNo ratings yet
- 2 Transplantation ImmunologyDocument33 pages2 Transplantation Immunologykirubel getyeNo ratings yet
- Immunology and MicrobiologyDocument91 pagesImmunology and MicrobiologyB.simhachalamNo ratings yet
- Vaccine Immunology and Herd Immunity: SubjectsDocument13 pagesVaccine Immunology and Herd Immunity: SubjectsWint ArdhayaniNo ratings yet
- Cells in ResponsesDocument30 pagesCells in ResponsesbacitusNo ratings yet
- Transplantation and Rejection 2022Document25 pagesTransplantation and Rejection 2022malkalhmaidh03No ratings yet
- Scientifica2012 215308Document18 pagesScientifica2012 215308AnjanaNo ratings yet
- Antigen PresentationDocument41 pagesAntigen PresentationDavid lufafaNo ratings yet
- Overview of The Immune System 2020Document31 pagesOverview of The Immune System 2020mehakNo ratings yet
- Lecture 5 - Cell Mediated Immunity - UpdateDocument29 pagesLecture 5 - Cell Mediated Immunity - UpdateLisandrea BrownNo ratings yet
- TransplantationDocument34 pagesTransplantationIlham KuNo ratings yet
- Humoral Immunity: Dr. Beenish ZahidDocument24 pagesHumoral Immunity: Dr. Beenish ZahidayeshaNo ratings yet
- Immunology PDFDocument70 pagesImmunology PDFstancy thomasNo ratings yet
- Sanchez Trincado2017Document15 pagesSanchez Trincado2017Andres JarrinNo ratings yet
- Humoral Immune ResponsesDocument34 pagesHumoral Immune ResponsesvivinNo ratings yet
- Clinical Immunology and Allergic Disease: Asthma Acquired Cat Acute Asthma Cell AllergenDocument8 pagesClinical Immunology and Allergic Disease: Asthma Acquired Cat Acute Asthma Cell AllergenSarfaraz ansariNo ratings yet
- Overview of Adaptive Immune Mechanisms - SlidesDocument26 pagesOverview of Adaptive Immune Mechanisms - SlidesEssington BeloNo ratings yet
- Immunity: Innate Defenses Specific Immunity Cell Mediated Immunity Self RecognitionDocument56 pagesImmunity: Innate Defenses Specific Immunity Cell Mediated Immunity Self RecognitionMiranda sekar arumNo ratings yet
- ImmunityDocument58 pagesImmunityzaha shamseerNo ratings yet
- Immunology Study Sheet: Immunohistology, IntroductoryDocument48 pagesImmunology Study Sheet: Immunohistology, IntroductoryAnonymous fnJQ3ONo ratings yet
- Specific Host Defenses: The Immune ResponseDocument54 pagesSpecific Host Defenses: The Immune Responseadyaly44No ratings yet
- Immuno Chapter 31323334Document12 pagesImmuno Chapter 31323334pia przNo ratings yet
- Programme M.SC BT Course Code: 19BTP06 Course Title: ImmunotechnologyDocument14 pagesProgramme M.SC BT Course Code: 19BTP06 Course Title: ImmunotechnologyNarendhran SNo ratings yet
- 7.2 Immunology Adaptive Immunity 17dec2021Document37 pages7.2 Immunology Adaptive Immunity 17dec20212023406162No ratings yet
- Chapter 17 Winter 2020Document47 pagesChapter 17 Winter 2020LESLI RODRIGUEZ BENDEZUNo ratings yet
- Diseases of The Immune SystemDocument8 pagesDiseases of The Immune SystemRuel MateoNo ratings yet
- Lecture 19, Ch. 43Document21 pagesLecture 19, Ch. 43S. SpencerNo ratings yet
- Lecture 2 Adaptive Immunity and Immunological ToleranceDocument26 pagesLecture 2 Adaptive Immunity and Immunological ToleranceNadia SolohNo ratings yet
- Basi ImmunologiaDocument53 pagesBasi ImmunologiaAanchalNo ratings yet
- Class 05-06Document64 pagesClass 05-06Vinoth Kanna ANo ratings yet
- Immune Regulation and ToleranceDocument33 pagesImmune Regulation and ToleranceAniruddha RoyNo ratings yet
- Adaptive Immunity IDocument29 pagesAdaptive Immunity Ixfxw5m5bczNo ratings yet
- Humoral ImmunityDocument9 pagesHumoral ImmunityPavel NesmiyanovNo ratings yet
- Host Defense Against Viral Infection-AnimalsDocument25 pagesHost Defense Against Viral Infection-AnimalsAshleyNo ratings yet
- Somatic Recombination and Hypermutation in The Immune SystemDocument62 pagesSomatic Recombination and Hypermutation in The Immune SystemLaura TapiaNo ratings yet
- Transplantation Immunology: MEDT 21 - Immunology and SerologyDocument47 pagesTransplantation Immunology: MEDT 21 - Immunology and SerologyViena Mae MaglupayNo ratings yet
- Piis0272638615005120 1Document11 pagesPiis0272638615005120 1KRIZARA MARIA VALVERDE RIVERANo ratings yet
- Medical Microbiology - Chapter 18 - Haemophilus, Bordetella, Brucella, and FrancisellaDocument1 pageMedical Microbiology - Chapter 18 - Haemophilus, Bordetella, Brucella, and FrancisellaBella DonnaNo ratings yet
- Gribbles Heska Gvmar BF Nat 01542Document32 pagesGribbles Heska Gvmar BF Nat 01542Emna BouhajjaNo ratings yet
- GCSE Week 12 Pathogens and DiseaseDocument27 pagesGCSE Week 12 Pathogens and DiseaseFrankie BarnesNo ratings yet
- EvaluasiDocument143 pagesEvaluasidyna rosyidahNo ratings yet
- Quantitative Flow Cytometry in The Clinical LaboratoryDocument20 pagesQuantitative Flow Cytometry in The Clinical Laboratorykmaher8256No ratings yet
- GAF 2021 BrochureDocument16 pagesGAF 2021 BrochureAtulSanapNo ratings yet
- RH. Lesson PlanDocument14 pagesRH. Lesson PlanNithiya NadesanNo ratings yet
- Cytokines - IntroductionDocument2 pagesCytokines - IntroductionTra gicNo ratings yet
- Philippine Medical Association Study Indicates That Women Were Injected With Contaminated Tetanus VaccineDocument2 pagesPhilippine Medical Association Study Indicates That Women Were Injected With Contaminated Tetanus VaccineJonathan Robert Kraus (OutofMudProductions)No ratings yet
- Best of Fives For Dentistry, Third Edition - NodrmDocument216 pagesBest of Fives For Dentistry, Third Edition - NodrmbassamNo ratings yet
- Etiology of ThrombocytosisDocument5 pagesEtiology of ThrombocytosisSimon Messi SiringoringoNo ratings yet
- Dengue Fever Case StudyDocument5 pagesDengue Fever Case StudyJen Faye Orpilla100% (1)
- Baba T.1984. Cell-Mediated Immune Protection in Chickens Against P MultocidaDocument6 pagesBaba T.1984. Cell-Mediated Immune Protection in Chickens Against P MultocidakrodriguezNo ratings yet
- DMH Blood Safety IndicatorDocument7 pagesDMH Blood Safety IndicatorCharmaine Corpuz GranilNo ratings yet
- Chapter 1 - Performance TaskDocument18 pagesChapter 1 - Performance Taskmargarita perezNo ratings yet
- Hepatitis C PHD ThesisDocument8 pagesHepatitis C PHD Thesisafkogftet100% (2)
- Final Micro Module 1Document73 pagesFinal Micro Module 1Ahmed KerAtyNo ratings yet
- HIV NotesDocument38 pagesHIV NotesMie CorsNo ratings yet
- Immunization Review GPDocument46 pagesImmunization Review GPKishore ChandkiNo ratings yet
- Discharge TB Summary CensusDocument5 pagesDischarge TB Summary CensusEdryl Piamonte UgpoNo ratings yet
- 2-Step TB Testing Info2Document2 pages2-Step TB Testing Info2desiyaniNo ratings yet
- DISEASE: - Malaria - : CAUSATIVE AGENTDocument3 pagesDISEASE: - Malaria - : CAUSATIVE AGENTDiamante MhayaleneNo ratings yet
- IVMS - General Pathology, Inflammation NotesDocument19 pagesIVMS - General Pathology, Inflammation NotesMarc Imhotep Cray, M.D.No ratings yet
- AMOEBIASISDocument11 pagesAMOEBIASISsrini9047No ratings yet
- PPDS - PK. 03-19 But N DAFTAR PUSTAKA PDFDocument6 pagesPPDS - PK. 03-19 But N DAFTAR PUSTAKA PDFZulfirahnurhalimahNo ratings yet