You might also like
- Flossophy Forsyth: N e W S L e T T e RDocument4 pagesFlossophy Forsyth: N e W S L e T T e RAnthony LiNo ratings yet
- Optimal Vs Ideal OcclusionDocument6 pagesOptimal Vs Ideal OcclusionshraddhaNo ratings yet
- Article 1525485399Document4 pagesArticle 1525485399anisah fadilahNo ratings yet
- Text F15ACF818884 1Document5 pagesText F15ACF818884 1Triman AhluwaliaNo ratings yet
- Diastema Closure and Long-Term Stability: Thomas F. Mulligan, DDS, MSDDocument15 pagesDiastema Closure and Long-Term Stability: Thomas F. Mulligan, DDS, MSDcristhian NustesNo ratings yet
- Canine Impaction A Review of The Prevalence, Etiology, Diagnosis and TreatmentDocument7 pagesCanine Impaction A Review of The Prevalence, Etiology, Diagnosis and TreatmentFadiShihabNo ratings yet
- Black TriangleDocument9 pagesBlack TriangleYasser MagramiNo ratings yet
- Anagement of Space Problems in The Primary and Mixed DentitionsDocument10 pagesAnagement of Space Problems in The Primary and Mixed Dentitionsjing.zhao222No ratings yet
- Diagnosis Dilemmas in Vital Pulp Therapy Treatment For The Toothache Is Changing.Document10 pagesDiagnosis Dilemmas in Vital Pulp Therapy Treatment For The Toothache Is Changing.khawla boukhNo ratings yet
- Open Bite, A Review of Etiology and Manageme PDFDocument8 pagesOpen Bite, A Review of Etiology and Manageme PDFVieussens JoffreyNo ratings yet
- Spear Anterior Open BitesDocument28 pagesSpear Anterior Open BitesMahmoud AlsuleimanNo ratings yet
- Management of Impacted Maxillary Canines Using The Kilroy Spring: A Case SeriesDocument7 pagesManagement of Impacted Maxillary Canines Using The Kilroy Spring: A Case SeriesThang Nguyen TienNo ratings yet
- Lechner. Placement of Artificial Teeth The Influence of Psyche and Illusion. (1997)Document9 pagesLechner. Placement of Artificial Teeth The Influence of Psyche and Illusion. (1997)Jose Enrique AvilaNo ratings yet
- The Clues Behind BruxismDocument3 pagesThe Clues Behind BruxismXRL8No ratings yet
- History and Physical Treatment / Management: Page 2 of 5Document1 pageHistory and Physical Treatment / Management: Page 2 of 5Adliah ZahiraNo ratings yet
- Ijcmr Jul Sep 5 2014Document16 pagesIjcmr Jul Sep 5 2014Kimberly Zeña MadridNo ratings yet
- Pugliese2019 Black Triangles - Preventing Their Occurrence, Managing Them When Prevention Is Not PracticalDocument12 pagesPugliese2019 Black Triangles - Preventing Their Occurrence, Managing Them When Prevention Is Not Practicalsolodont1No ratings yet
- Spear-Approaches To Vertical DimensionDocument11 pagesSpear-Approaches To Vertical DimensionMario Zúñiga Gonzales100% (2)
- The Great Occlusion Fiasco: DitorialDocument2 pagesThe Great Occlusion Fiasco: DitorialruacondungmanhNo ratings yet
- Milton Lappin, Detroit, MichDocument10 pagesMilton Lappin, Detroit, MichMarcos CastroNo ratings yet
- Timing in Orthodontics PDFDocument5 pagesTiming in Orthodontics PDFdrzana78No ratings yet
- Chapter 2: Operative Dentistry and Prosthodontics: AnswersDocument13 pagesChapter 2: Operative Dentistry and Prosthodontics: AnswersBinayak UpadhyayaNo ratings yet
- When Does A Patient Need A "Functional Analysis" of Their Dental Occlusion?Document3 pagesWhen Does A Patient Need A "Functional Analysis" of Their Dental Occlusion?David ColonNo ratings yet
- Lit 064Document8 pagesLit 064James LinNo ratings yet
- Direct CompositDocument8 pagesDirect CompositJulianna BartalusNo ratings yet
- Etiology and Treatment of Midline DiastemaDocument3 pagesEtiology and Treatment of Midline DiastemaPuteri NazirahNo ratings yet
- Diastema Closure and Long-Term Stability - JCO-OnLINEDocument15 pagesDiastema Closure and Long-Term Stability - JCO-OnLINEAbad SalcedoNo ratings yet
- Midline Diastema Treatment OptionsDocument6 pagesMidline Diastema Treatment OptionsnandaNo ratings yet
- Functional Analysis of OcclusionDocument3 pagesFunctional Analysis of OcclusionOrtodoncia UNAL 2020No ratings yet
- Hsieh - Nuance in Bilateral Cleft Lip RepairDocument9 pagesHsieh - Nuance in Bilateral Cleft Lip RepairFauzia Latifah SupriyadiNo ratings yet
- Occlusion 6Document9 pagesOcclusion 6Fatima AliNo ratings yet
- Periodontal Treatment of Excessive Gingival Display: Ramzi V. Abou-Arraj, DDS, MS, and Nada M. Souccar, DDS, MSDocument12 pagesPeriodontal Treatment of Excessive Gingival Display: Ramzi V. Abou-Arraj, DDS, MS, and Nada M. Souccar, DDS, MSvaleriaNo ratings yet
- 5-Management of Space ProblemsDocument10 pages5-Management of Space ProblemsMuhammad UzairNo ratings yet
- Hudson Ling Arch 2013Document6 pagesHudson Ling Arch 2013Manda JoanNo ratings yet
- Gingival Replacement in The Aesthetic ZoneDocument6 pagesGingival Replacement in The Aesthetic ZoneLynda M. NaranjoNo ratings yet
- Perio-Restorative Inter-Relationships: 8# Periodontal Lec. April 16, 2009Document10 pagesPerio-Restorative Inter-Relationships: 8# Periodontal Lec. April 16, 2009api-3827876No ratings yet
- Palatally Impacted CaninesDocument5 pagesPalatally Impacted CaninesMoisés MartinsNo ratings yet
- Cleft Lip PalateDocument4 pagesCleft Lip PalateManjulika TysgiNo ratings yet
- Soft Tissue Analysis: Dr. Ayushi Toley PG Ist YearDocument70 pagesSoft Tissue Analysis: Dr. Ayushi Toley PG Ist YearAyushi ToleyNo ratings yet
- Biologic Width and Its Relation To PeriodontalDocument7 pagesBiologic Width and Its Relation To PeriodontalBethania CarolinaNo ratings yet
- Decision Making For Tooth Extraction or ConservationDocument16 pagesDecision Making For Tooth Extraction or Conservationavi_sdc100% (1)
- Surgical OrthodonticsDocument301 pagesSurgical Orthodonticsdr_nilofervevai2360100% (4)
- NBK482262Document1 pageNBK482262Adliah ZahiraNo ratings yet
- Midline ShiftDocument6 pagesMidline ShiftMaiush JbNo ratings yet
- Cleft Management 11Document6 pagesCleft Management 11Aniket PotnisNo ratings yet
- Burke Et Al-2009-Journal of Esthetic and Restorative DentistryDocument4 pagesBurke Et Al-2009-Journal of Esthetic and Restorative DentistryMatheus CostaNo ratings yet
- Occlusion, Function, and ParafunctionDocument11 pagesOcclusion, Function, and ParafunctionVesna DjurdjevicNo ratings yet
- 6+SADJ June 2022 Review Part+5+New+roots+titanium+and+its+influenceDocument5 pages6+SADJ June 2022 Review Part+5+New+roots+titanium+and+its+influenceDr. Zardasht N. BradostyNo ratings yet
- KuyfDocument10 pagesKuyfdwNo ratings yet
- 1947 Immediate Denture GielerDocument7 pages1947 Immediate Denture Gielersiti corynikenNo ratings yet
- 4.gingival RecessionDocument4 pages4.gingival RecessionmirfanulhaqNo ratings yet
- OrthodonticDocument3 pagesOrthodonticFirma Nurdinia DewiNo ratings yet
- Management of The Soft Palate Defect Steven Eckert PDFDocument15 pagesManagement of The Soft Palate Defect Steven Eckert PDFintanursamsiNo ratings yet
- Periodontal Considerations in Veneer CasesDocument7 pagesPeriodontal Considerations in Veneer CasesBethania CarolinaNo ratings yet
- Decision Making of Treatment of Furcation InvolvementDocument4 pagesDecision Making of Treatment of Furcation InvolvementazyytieNo ratings yet
- Crown ContoursDocument6 pagesCrown Contoursdorasani99No ratings yet
- Ranula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandRanula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- ISQ Scale Articles Summaries A4Document2 pagesISQ Scale Articles Summaries A4Nestor WilderNo ratings yet
- The Neutral Zone in Complete DenturesDocument8 pagesThe Neutral Zone in Complete DenturesToDownload81No ratings yet
- Li 2011Document11 pagesLi 2011Hurāirāh ĐāřNo ratings yet
- Attachment Selection For Implant OverdenturesDocument36 pagesAttachment Selection For Implant OverdenturesNestor WilderNo ratings yet
- Pi Is 0022391307601176Document4 pagesPi Is 0022391307601176Nestor WilderNo ratings yet
- JIndianProsthodontSoc21119-5027627 135756Document9 pagesJIndianProsthodontSoc21119-5027627 135756Nestor WilderNo ratings yet
- Abutment Selection CriteriaDocument4 pagesAbutment Selection CriteriaNestor WilderNo ratings yet
- Jurnal Perbandingan Tipe AbutmentDocument7 pagesJurnal Perbandingan Tipe AbutmentKharismaNisaNo ratings yet
- Jurnal Perbandingan Tipe AbutmentDocument7 pagesJurnal Perbandingan Tipe AbutmentKharismaNisaNo ratings yet
- Li 2011Document11 pagesLi 2011Hurāirāh ĐāřNo ratings yet
- Li 2011Document11 pagesLi 2011Hurāirāh ĐāřNo ratings yet
- Complex Numbers and The Complex Exponential: Figure 1. A Complex NumberDocument22 pagesComplex Numbers and The Complex Exponential: Figure 1. A Complex NumberClyde LabayNo ratings yet
- Optimum Selection Dental Implant DiameterDocument11 pagesOptimum Selection Dental Implant DiameterNestor WilderNo ratings yet
- Li 2011Document11 pagesLi 2011Hurāirāh ĐāřNo ratings yet
- Prime Number Chart: Math Learning Center Supplements 698-1579 CB 116Document1 pagePrime Number Chart: Math Learning Center Supplements 698-1579 CB 116Nestor WilderNo ratings yet
- Causes of Color: - The Sensation of Color Is Caused by The Brain. - Some Ways To Get This Sensation IncludeDocument66 pagesCauses of Color: - The Sensation of Color Is Caused by The Brain. - Some Ways To Get This Sensation IncludeNestor WilderNo ratings yet
- S.19 Flyer QuecksDocument1 pageS.19 Flyer QuecksNestor WilderNo ratings yet
- ERA TroubleshootingDocument3 pagesERA TroubleshootingNestor WilderNo ratings yet
- DFU AH 26 EngDocument3 pagesDFU AH 26 EngNestor WilderNo ratings yet
- Glumadesensitizer Card d1424f8Document1 pageGlumadesensitizer Card d1424f8Nestor WilderNo ratings yet
- QPD - Post-Discharge Follow-Up Phone Call Script SampleDocument3 pagesQPD - Post-Discharge Follow-Up Phone Call Script Samplejphinazee218No ratings yet
- FCA Problems RevisedDocument12 pagesFCA Problems RevisedRomelle Jane M. VelascoNo ratings yet
- Invoice, packing list mẫuDocument2 pagesInvoice, packing list mẫuPHI BUI MINHNo ratings yet
- Rigatoni With Beef and Onion RaguDocument3 pagesRigatoni With Beef and Onion RagumadduxdavidNo ratings yet
- 94 175 1 SM PDFDocument8 pages94 175 1 SM PDFikaNo ratings yet
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- QTR-2 2023 Meeting Format Nov.23Document45 pagesQTR-2 2023 Meeting Format Nov.23skumar31397No ratings yet
- IDSA Guias Infeccion de Tejidos Blandos 2014 PDFDocument43 pagesIDSA Guias Infeccion de Tejidos Blandos 2014 PDFyonaNo ratings yet
- Mayank Yadav: Academic QualificationDocument2 pagesMayank Yadav: Academic QualificationJacob PruittNo ratings yet
- Concrete Canvas Presentation-PT. Prima Minechem IndonesiaDocument98 pagesConcrete Canvas Presentation-PT. Prima Minechem Indonesiaantonsugiarto20_7049No ratings yet
- Oedipus SummaryDocument1 pageOedipus SummaryReynold FrancoNo ratings yet
- Worksheet. 5. Sexual Reproduction in PlantDocument4 pagesWorksheet. 5. Sexual Reproduction in PlantLeonita SwandjajaNo ratings yet
- PilatesDocument65 pagesPilatesAna MariaNo ratings yet
- Escape From The Western Diet Summary RevisedDocument3 pagesEscape From The Western Diet Summary Revisedapi-385530863100% (1)
- MAPEH Assignment For Mr. Felicilda (Only)Document6 pagesMAPEH Assignment For Mr. Felicilda (Only)Jericho Green Gerona100% (1)
- Ark of The Covenant Montessori Chamber of Learning PoblacionDocument3 pagesArk of The Covenant Montessori Chamber of Learning PoblacionMaiAce Sean Shawn SynneNo ratings yet
- Mission and VissionDocument11 pagesMission and VissionPradeep Kumar V PradiNo ratings yet
- Initial Data Base FormatDocument7 pagesInitial Data Base FormatrhamhonaNo ratings yet
- Immulite Homocysteine 2000Document30 pagesImmulite Homocysteine 2000Symbolin MusenkoNo ratings yet
- Iodine Clock ReactionDocument3 pagesIodine Clock Reactionsunny_415No ratings yet
- Amp-Eng Anger Management ProfileDocument6 pagesAmp-Eng Anger Management Profileminodora100% (1)
- 1often Wonder About My Future As I Am About To Finish Secondary SchoolDocument2 pages1often Wonder About My Future As I Am About To Finish Secondary SchoolMidz Santayana100% (1)
- Laboratory Manual For Microbiology Fundamentals A Clinical Approach 4Th Edition Susan Finazzo Full ChapterDocument51 pagesLaboratory Manual For Microbiology Fundamentals A Clinical Approach 4Th Edition Susan Finazzo Full Chapterlinda.ferguson121100% (7)
- Labour Market Regimes V4.0Document8 pagesLabour Market Regimes V4.0Gail WardNo ratings yet
- First Communion: You Are The VoiceDocument10 pagesFirst Communion: You Are The VoiceErnesto Albeus Villarete Jr.No ratings yet
- Explain Why Seed Vigor Determination Is ImportantDocument5 pagesExplain Why Seed Vigor Determination Is ImportantSolomon MbeweNo ratings yet
- A Grammar of Power in Psychotherapy Exploring The Dynamics of Privilege (Malin Fors)Document220 pagesA Grammar of Power in Psychotherapy Exploring The Dynamics of Privilege (Malin Fors)Andrea A. Ortiz Vázquez100% (1)
- 3RD Summative Exam in Science 6Document6 pages3RD Summative Exam in Science 6Maricris Palermo SancioNo ratings yet
- Paper - Impact of Rapid Urbanization On Agricultural LandsDocument10 pagesPaper - Impact of Rapid Urbanization On Agricultural LandsKosar Jabeen100% (1)
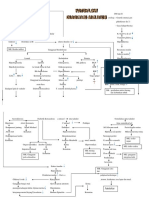
- Patoflow DMDocument2 pagesPatoflow DMAngel da CostaNo ratings yet