You might also like
- The Concise Book of Trigger Points, Third Edition - Simeon Niel-AsherDocument5 pagesThe Concise Book of Trigger Points, Third Edition - Simeon Niel-Asherxysypocu0% (1)
- Multi-Drug-resistant Tuberculosis - Wikipedia, The Free EncyclopediaDocument8 pagesMulti-Drug-resistant Tuberculosis - Wikipedia, The Free Encyclopedianayan555No ratings yet
- MDRTB Case StudyDocument35 pagesMDRTB Case StudyFejlean Angelica AntineoNo ratings yet
- JOP Vol 3 Issue 2 MayDocument84 pagesJOP Vol 3 Issue 2 Mayesma bekirogluNo ratings yet
- Drug Study - CefuroximeDocument2 pagesDrug Study - CefuroximeSiergs Smith GervacioNo ratings yet
- Fast Facts: Asthma: Improve patient self-management and drug use, achieve asthma controlFrom EverandFast Facts: Asthma: Improve patient self-management and drug use, achieve asthma controlNo ratings yet
- Clexane® 60mg/0.6ml SyringesDocument8 pagesClexane® 60mg/0.6ml Syringesnaga chaitanyaNo ratings yet
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareFrom EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareNo ratings yet
- Mupirocin Drug StudyDocument1 pageMupirocin Drug StudyArthur Christopher Corpuz0% (1)
- Skrining ResepDocument8 pagesSkrining ResephanifakhNo ratings yet
- Reflection in and On Nursing Practices - How NursesDocument7 pagesReflection in and On Nursing Practices - How NursesChris LeeNo ratings yet
- Clinical management of tuberculosis with a focus on gastrointestinal TBDocument5 pagesClinical management of tuberculosis with a focus on gastrointestinal TBparmar jalpabenNo ratings yet
- Akurit 4 TBDocument14 pagesAkurit 4 TBNicolloNo ratings yet
- PHD Thesis Samuel Coenen PDFDocument172 pagesPHD Thesis Samuel Coenen PDFsamuel_coenenNo ratings yet
- Treatment Outcome of Multi-Drug Resistant Tuberculosis in The United Kingdom: Retrospective-Prospective Cohort Study From 2004 To 2007Document15 pagesTreatment Outcome of Multi-Drug Resistant Tuberculosis in The United Kingdom: Retrospective-Prospective Cohort Study From 2004 To 2007galih suharnoNo ratings yet
- Original Articles: 32 Years' Experience of Peritoneal Dialysis-Related Peritonitis in A University HospitalDocument9 pagesOriginal Articles: 32 Years' Experience of Peritoneal Dialysis-Related Peritonitis in A University HospitalRicardo Costa da SilvaNo ratings yet
- Ibrt 06 I 4 P 232Document2 pagesIbrt 06 I 4 P 232Aditia Nata KusumaNo ratings yet
- MX of Paediatric TBDocument8 pagesMX of Paediatric TBAjanapakhi SahaNo ratings yet
- Case Study TBDocument4 pagesCase Study TBMichael Baylon DueñasNo ratings yet
- E AungDocument9 pagesE AungDr.Hemant SharmaNo ratings yet
- Extrapulmonary TuberculosisDocument2 pagesExtrapulmonary TuberculosisIcha NathaniaNo ratings yet
- Servikal TBDocument15 pagesServikal TBnur wahidaNo ratings yet
- Drug Resistance of TBDocument17 pagesDrug Resistance of TBGaurav Sharma100% (1)
- Association of Food and Drug Allergy With Anti-Tuberculosis Drug Related Hepatitis or Skin Reactions: A Case Control StudyDocument6 pagesAssociation of Food and Drug Allergy With Anti-Tuberculosis Drug Related Hepatitis or Skin Reactions: A Case Control StudyPutri YingNo ratings yet
- Factors Impacting Tuberculosis Treatment Adherence in Rural TurkeyDocument7 pagesFactors Impacting Tuberculosis Treatment Adherence in Rural TurkeyAnonymous QPXAgjBwNo ratings yet
- Cryptococcus GuidelinesDocument9 pagesCryptococcus GuidelinesAndreas IoannouNo ratings yet
- Jurnal Intensified Antituberculosis Therapy in Adult With Tuberculous MeningitisDocument13 pagesJurnal Intensified Antituberculosis Therapy in Adult With Tuberculous Meningitisnaila ghinayaNo ratings yet
- Consensus StatementDocument4 pagesConsensus StatementPrasanna NarayananNo ratings yet
- TB Nursing CareplanDocument14 pagesTB Nursing CareplanEstherThompson100% (1)
- TUBERCULOSIS GUIDELINESDocument11 pagesTUBERCULOSIS GUIDELINESAbdul AkhtarNo ratings yet
- Moxifloxaxin For CAPDocument9 pagesMoxifloxaxin For CAPmateri posNo ratings yet
- s3-2Document6 pagess3-2stephenpillar1718No ratings yet
- WAO Journal: Pei-Ying Lin, Chun-Hui Chu, Fang-Yu Chang, Ya-Wen Huang, Hui-Ju Tsai, Tsung-Chieh YaoDocument10 pagesWAO Journal: Pei-Ying Lin, Chun-Hui Chu, Fang-Yu Chang, Ya-Wen Huang, Hui-Ju Tsai, Tsung-Chieh YaoSiti Arum WidiyantiNo ratings yet
- WHO Bulletin 2005Document10 pagesWHO Bulletin 2005ajh2675No ratings yet
- Adverse Drug Reactions of Primary Anti-tuberculosis DrugsDocument8 pagesAdverse Drug Reactions of Primary Anti-tuberculosis DrugsSelina WijayaNo ratings yet
- PCT Guidance Reduces Antibiotic Use in CAPDocument10 pagesPCT Guidance Reduces Antibiotic Use in CAPmohd zonNo ratings yet
- Early ViewDocument34 pagesEarly Viewyesid urregoNo ratings yet
- Treatment of TuberculosisDocument15 pagesTreatment of TuberculosisLabbakYaMahdiNo ratings yet
- MDR-TB HIV Coinfection Case Report King Khalid HospitalDocument2 pagesMDR-TB HIV Coinfection Case Report King Khalid HospitalryoNo ratings yet
- Mortality Among Tuberculosis Patients in The Democratic Republic of CongoDocument7 pagesMortality Among Tuberculosis Patients in The Democratic Republic of CongoGary Rios DionicioNo ratings yet
- Real World Experiences Pirfenidone and Nintedanib Are Effective and Well Tolerated Treatments For Idiopathic Pulmonary FibrosisDocument12 pagesReal World Experiences Pirfenidone and Nintedanib Are Effective and Well Tolerated Treatments For Idiopathic Pulmonary FibrosismaleticjNo ratings yet
- Adverse Reactions To First-LineDocument19 pagesAdverse Reactions To First-Linegeneva123No ratings yet
- Treatment of Multidrug-Resistant Tuberculosis: Evidence and ControversiesDocument9 pagesTreatment of Multidrug-Resistant Tuberculosis: Evidence and ControversiesAta07No ratings yet
- Severe Asthma in Primary Care: Identification and ManagementDocument8 pagesSevere Asthma in Primary Care: Identification and ManagementIzza UrfanNo ratings yet
- Drug and Therapeutics Newsletter Vol 1 No 3 Dec 2019Document4 pagesDrug and Therapeutics Newsletter Vol 1 No 3 Dec 2019AnGeL_4No ratings yet
- IJTLDeditorial Protecting HCworkers Form TBDocument2 pagesIJTLDeditorial Protecting HCworkers Form TBRoma ParyaniNo ratings yet
- TUBERCULOSISDocument16 pagesTUBERCULOSISfranciz CalagoNo ratings yet
- The Clinical Impact of Drug-Induced HepatotoxicityDocument9 pagesThe Clinical Impact of Drug-Induced HepatotoxicityDi LaNo ratings yet
- Rifampicina TBMR NEJM 2019Document13 pagesRifampicina TBMR NEJM 2019carolinaNo ratings yet
- Prediction of Post-Tuberculosis Lung Function ImpairmentDocument12 pagesPrediction of Post-Tuberculosis Lung Function ImpairmentputriargathyaNo ratings yet
- Modifications in Drug Adherence After Switch To Fixed Dose Combination of Perindopril Amlodipine in Clinical Practice Results of A Large ScaleDocument8 pagesModifications in Drug Adherence After Switch To Fixed Dose Combination of Perindopril Amlodipine in Clinical Practice Results of A Large ScalenembutalNo ratings yet
- ITU Comparacion 7 - 14 Dias de TtoDocument9 pagesITU Comparacion 7 - 14 Dias de TtoJohana Zamudio RojasNo ratings yet
- Comparison of Cefepime With Piperacillin Tazobactam Treatment in Patients With HDocument11 pagesComparison of Cefepime With Piperacillin Tazobactam Treatment in Patients With HWilliam BarreraNo ratings yet
- 3 RaDocument16 pages3 RaNitish TankNo ratings yet
- Mind The Gap - Managing Tuberculosis Across The DiDocument12 pagesMind The Gap - Managing Tuberculosis Across The DiK ValtierraNo ratings yet
- Joanne Bernadette C. Aguilar Bsn-3Document3 pagesJoanne Bernadette C. Aguilar Bsn-3Joanne Bernadette AguilarNo ratings yet
- International Standard For Tuberculosis Care 2009Document5 pagesInternational Standard For Tuberculosis Care 2009Stephanie DewiNo ratings yet
- Assessment of Synthetic Glucocorticoids in Asthmatic SputumDocument3 pagesAssessment of Synthetic Glucocorticoids in Asthmatic SputumDewiRahmatikaNo ratings yet
- Multidrug Resistant Tuberculosis A Pharmacological View Based On Revised National Tuberculosis Control Programme DOTS-Plus GuidelinesDocument7 pagesMultidrug Resistant Tuberculosis A Pharmacological View Based On Revised National Tuberculosis Control Programme DOTS-Plus GuidelinesIOSR Journal of PharmacyNo ratings yet
- Inappropriate Use of Proton Pump Inhibitors in Elderly Patients Discharged From Acute Care HospitalsDocument6 pagesInappropriate Use of Proton Pump Inhibitors in Elderly Patients Discharged From Acute Care HospitalsFitriNo ratings yet
- Burden of Tuberculosis - Combating Drug Resistance: EditorialDocument3 pagesBurden of Tuberculosis - Combating Drug Resistance: EditorialmominamalikNo ratings yet
- J. Antimicrob. Chemother. 2011 Xu 1687 95Document9 pagesJ. Antimicrob. Chemother. 2011 Xu 1687 95novia khairulbariaNo ratings yet
- Antibiotics For Recurrent Acute Pharyngo-Tonsillitis Systematic Review 2018 PDFDocument10 pagesAntibiotics For Recurrent Acute Pharyngo-Tonsillitis Systematic Review 2018 PDFNoca AriantiNo ratings yet
- Predicting Benign Course and Prolonged Illness in Lower Respiratory Tract Infections: A 13 European Country StudyDocument8 pagesPredicting Benign Course and Prolonged Illness in Lower Respiratory Tract Infections: A 13 European Country Studypanji satryo utomoNo ratings yet
- Smoking Increases Risk of Recurrence After Successful Anti-Tuberculosis TreatmentDocument8 pagesSmoking Increases Risk of Recurrence After Successful Anti-Tuberculosis TreatmentRaditya Imam PratanaNo ratings yet
- Atorvastatin Improves Sputum Conversion and Chest X-Ray Severity ScoreDocument6 pagesAtorvastatin Improves Sputum Conversion and Chest X-Ray Severity Scorecharmainemargaret.parreno.medNo ratings yet
- Istc & DotsDocument67 pagesIstc & DotsNadilaNo ratings yet
- The "Completely Randomised" and The "Randomised Block" Are The Only Experimental Designs Suitable For Widespread Use in Pre Clinical ResearchDocument5 pagesThe "Completely Randomised" and The "Randomised Block" Are The Only Experimental Designs Suitable For Widespread Use in Pre Clinical ResearchChris LeeNo ratings yet
- Reflections in LearningDocument17 pagesReflections in LearningChris LeeNo ratings yet
- Arterial Blood Gas (ABG) Analysis: Normal ValuesDocument3 pagesArterial Blood Gas (ABG) Analysis: Normal ValuesNayem Hossain HemuNo ratings yet
- Nursing Reflective Practice - An Empirical Literature ReviewDocument10 pagesNursing Reflective Practice - An Empirical Literature ReviewChris LeeNo ratings yet
- Reflective Learning in Higher Education - A Comparative AnalysisDocument8 pagesReflective Learning in Higher Education - A Comparative AnalysisChris LeeNo ratings yet
- 3B User-Manual CPAP-Auto-CPAP RESmart BMC V1.7 ENG-1Document35 pages3B User-Manual CPAP-Auto-CPAP RESmart BMC V1.7 ENG-1Ricardo Costa CaribéNo ratings yet
- Terms of The Creative Commons Attribution Share Alike-3.0 LicenseDocument109 pagesTerms of The Creative Commons Attribution Share Alike-3.0 LicenseChris LeeNo ratings yet
- Pneumonia, Atelectasis & EffusionsDocument38 pagesPneumonia, Atelectasis & EffusionsChris LeeNo ratings yet
- CT Scans of The Head: A Neurologist's PerspectiveDocument111 pagesCT Scans of The Head: A Neurologist's PerspectiveChris LeeNo ratings yet
- 12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramDocument66 pages12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramlalaNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityChris LeeNo ratings yet
- 狗乾糧推薦名單2021Document5 pages狗乾糧推薦名單2021Chris LeeNo ratings yet
- RESmart - CPAP, Auto - User ManualDocument40 pagesRESmart - CPAP, Auto - User ManualChris LeeNo ratings yet
- Thoracic Radiographic Anatomy: Einav Shochat MS4 Visiting Medical StudentDocument81 pagesThoracic Radiographic Anatomy: Einav Shochat MS4 Visiting Medical StudentChris LeeNo ratings yet
- How To Read A Head CTDocument90 pagesHow To Read A Head CTChris LeeNo ratings yet
- Pneumonia, Atelectasis & EffusionsDocument38 pagesPneumonia, Atelectasis & EffusionsChris LeeNo ratings yet
- Acute Stroke Management Resource:: Types of Stroke & Anatomy and Physiology of Acute StrokeDocument52 pagesAcute Stroke Management Resource:: Types of Stroke & Anatomy and Physiology of Acute StrokeChris LeeNo ratings yet
- CT Head and Ischemic Cva: What To Look For On The Early Scan??Document19 pagesCT Head and Ischemic Cva: What To Look For On The Early Scan??Chris LeeNo ratings yet
- 12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramDocument66 pages12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramlalaNo ratings yet
- 2 4 Plasma ProductsDocument3 pages2 4 Plasma Productsشريف عبد المنعمNo ratings yet
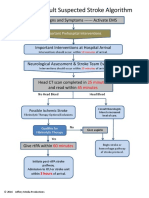
- ACLS Stroke Algorithm PDFDocument1 pageACLS Stroke Algorithm PDFChris LeeNo ratings yet
- CAPD - StaySafe Training Manual PDFDocument16 pagesCAPD - StaySafe Training Manual PDFChris LeeNo ratings yet
- Nursing Tools Psychotherapy PDFDocument1 pageNursing Tools Psychotherapy PDFChris LeeNo ratings yet
- Catheter Care Guidelines PDFDocument45 pagesCatheter Care Guidelines PDFJayakumar JNo ratings yet
- Cir 0000000000000613 PDFDocument10 pagesCir 0000000000000613 PDFDeivy De Jesus Cordoba SerratoNo ratings yet
- AHA Elearning - ACLS Precourse Self-Assessment and Precourse WorkDocument3 pagesAHA Elearning - ACLS Precourse Self-Assessment and Precourse WorkMalik AljaberiNo ratings yet
- NCCN Pain ManagementDocument14 pagesNCCN Pain ManagementcoooleNo ratings yet
- DAFTAR HARGA Produk Medis dari PT SEJAHTERA SURYA INTRAMEDIKADocument56 pagesDAFTAR HARGA Produk Medis dari PT SEJAHTERA SURYA INTRAMEDIKACilviNo ratings yet
- 368371Document10 pages368371Ashraf Uddin AhmedNo ratings yet
- Kategori Obat VenDocument40 pagesKategori Obat Venmulla ali qoriNo ratings yet
- DMTAC Protocol Tuanku Ampuan Najihah Kuala Pilah Update March 2013Document17 pagesDMTAC Protocol Tuanku Ampuan Najihah Kuala Pilah Update March 2013ummuawisy100% (1)
- Jurnal Reading Anestesi M. Fikri Ridha1102015122Document6 pagesJurnal Reading Anestesi M. Fikri Ridha1102015122Hielmy Auliya HasyimNo ratings yet
- Intramascular PharmaDocument7 pagesIntramascular Pharmajoher_junior16No ratings yet
- Roger Case Study and Nursing Process 2Document9 pagesRoger Case Study and Nursing Process 2E.R.ONo ratings yet
- Kuliah 2 Dermato Terapi 2015Document47 pagesKuliah 2 Dermato Terapi 2015Indit Septi PamujiNo ratings yet
- Drugs Used in IBDDocument44 pagesDrugs Used in IBDBegmuhammet BabayevNo ratings yet
- Bio Generics & IndiaDocument38 pagesBio Generics & Indiagupta1704100% (8)
- Faculty Advisers SY2022-2023-1Document2 pagesFaculty Advisers SY2022-2023-1Clark Joshua ManguneNo ratings yet
- GAD Treatment OptionsDocument3 pagesGAD Treatment OptionsRosaNo ratings yet
- Dosis Oseltamivir CDCDocument3 pagesDosis Oseltamivir CDCivonne marinNo ratings yet
- Internal Medicine Rotation SyllabusDocument9 pagesInternal Medicine Rotation Syllabusapi-665372449No ratings yet
- Drug Study: College of NursingDocument1 pageDrug Study: College of NursingJhielo ArambulaNo ratings yet
- Dry Needling - WikiDocument7 pagesDry Needling - WikiDavid ElirazNo ratings yet
- Lab Report PDDocument17 pagesLab Report PDhaikalNo ratings yet
- Spiritual Counseling Approach Helps Drug Patients RecoverDocument22 pagesSpiritual Counseling Approach Helps Drug Patients RecoverSitti Shafira Salsabilah 035No ratings yet
- Francis N. Ramirez, MDDocument9 pagesFrancis N. Ramirez, MDPridas GidNo ratings yet
- Obstetri & Gynekologi: AcarboseDocument2 pagesObstetri & Gynekologi: AcarboseDesi BrilianNo ratings yet
- Yguadiz TeachingDocument1 pageYguadiz TeachingYESSAMIN GUADIZNo ratings yet
- ICH GuidelinesDocument4 pagesICH Guidelinesaakash sahaNo ratings yet