You might also like
- How To Read A Head CT: (Or "How I Learned To Stop Worrying and Love Computed Tomography")Document89 pagesHow To Read A Head CT: (Or "How I Learned To Stop Worrying and Love Computed Tomography")Crhistian David García MontoyaNo ratings yet
- Brain CT ScanDocument127 pagesBrain CT ScanAsep Saripudin MNo ratings yet
- DFSGDFGDFDocument60 pagesDFSGDFGDFMada Dwi HariNo ratings yet
- How To Read A Head CT ScanDocument60 pagesHow To Read A Head CT ScanPompomNo ratings yet
- How To Read A Head CT: DR Mohamed El Safwany. MDDocument60 pagesHow To Read A Head CT: DR Mohamed El Safwany. MDYusuf BrilliantNo ratings yet
- Blood Can Be Very Bad (Perron Ich Acep 2005 Peds Course (1) )Document15 pagesBlood Can Be Very Bad (Perron Ich Acep 2005 Peds Course (1) )Moileon2011No ratings yet
- Dopplerultrasoundofthekidneys 130629025936 Phpapp01Document133 pagesDopplerultrasoundofthekidneys 130629025936 Phpapp01Denis PogoreviciNo ratings yet
- Dopple Ultrasound of The KidneysDocument60 pagesDopple Ultrasound of The KidneysivoklarinNo ratings yet
- Neuroimaging For Medical Residents: Kanokwan Boonyapisit, M.D. Department of Medicine Siriraj HospitalDocument106 pagesNeuroimaging For Medical Residents: Kanokwan Boonyapisit, M.D. Department of Medicine Siriraj HospitalRapid Medicine100% (4)
- Basic CXR Mod AdamDocument59 pagesBasic CXR Mod AdamCheska TumulakNo ratings yet
- Surgery Observation 3Document3 pagesSurgery Observation 3combuekNo ratings yet
- Pediatric Emergency Medicine Point of Care Ultrasound (POCUS) - Beyond FASTDocument51 pagesPediatric Emergency Medicine Point of Care Ultrasound (POCUS) - Beyond FASTSagar ShahNo ratings yet
- Thoracic Endoscopy: Advances in Interventional PulmonologyFrom EverandThoracic Endoscopy: Advances in Interventional PulmonologyMichael J. SimoffNo ratings yet
- 9 Femia2021Document9 pages9 Femia2021Vivi DeviyanaNo ratings yet
- Radiology CWRU Medical Student Elective Week 1Document112 pagesRadiology CWRU Medical Student Elective Week 1Yopi SimargiNo ratings yet
- Ankit 10 YrsDocument1 pageAnkit 10 YrsRAJESHNo ratings yet
- Poonama DeviDocument1 pagePoonama DeviRAJESHNo ratings yet
- Clinical Correlation Is NecessaryDocument1 pageClinical Correlation Is NecessaryRAJESHNo ratings yet
- Laporan Kasus: A 44-Day Old Male Infant With Thoracoabdominal Ectopia Cordis of Pentalogy Cantrell'S SyndromeDocument6 pagesLaporan Kasus: A 44-Day Old Male Infant With Thoracoabdominal Ectopia Cordis of Pentalogy Cantrell'S SyndromearlitasofyanNo ratings yet
- Head CT ScanDocument84 pagesHead CT ScanAbegail IbañezNo ratings yet
- Normal Brain of CTDocument1 pageNormal Brain of CTfuntwohowNo ratings yet
- Brain Imaging 2004-5finalDocument72 pagesBrain Imaging 2004-5finalCzar GrabNo ratings yet
- Permanent Junctional Reciprocating Tachycardia in Children - A Multicenter Experience 2014Document26 pagesPermanent Junctional Reciprocating Tachycardia in Children - A Multicenter Experience 2014Võ Từ NhấtNo ratings yet
- CT Study of Head Plain & ContrastDocument1 pageCT Study of Head Plain & ContrastRAJESHNo ratings yet
- Clinical Correlation Is NecessaryDocument1 pageClinical Correlation Is NecessaryrajeshsaloaNo ratings yet
- Short Case Hydrocephalus: by Febrianto Haba Bunga, S.Ked Consultant DR .Donny Argie, SP - BSDocument29 pagesShort Case Hydrocephalus: by Febrianto Haba Bunga, S.Ked Consultant DR .Donny Argie, SP - BSErkoNo ratings yet
- Cardiac UltrasoundDocument72 pagesCardiac Ultrasoundramon100% (6)
- Emergency Radiology With QuizDocument115 pagesEmergency Radiology With QuizJustisia PadmiyatiNo ratings yet
- Cara Membaca CTDocument61 pagesCara Membaca CTDio Alexander100% (1)
- 5 Minute Assessment: Arthur Cantos RN, MANDocument48 pages5 Minute Assessment: Arthur Cantos RN, MANCynthia ThomasNo ratings yet
- Nervous System AlterationsDocument45 pagesNervous System AlterationsMajesty ParkerNo ratings yet
- HHS Public Access: Common Findings in Late Gestation Fetal EchocardiographyDocument14 pagesHHS Public Access: Common Findings in Late Gestation Fetal EchocardiographyHugo ARNo ratings yet
- Tfus Part 1Document10 pagesTfus Part 1Seyfullah Halit KaragözNo ratings yet
- Carotid Artery Stenosis Gray-Scale and Doppler USDocument8 pagesCarotid Artery Stenosis Gray-Scale and Doppler USAli AlSowaidiNo ratings yet
- Clinical Correlation Is NecessaryDocument1 pageClinical Correlation Is NecessaryrajeshsaloaNo ratings yet
- Interpretation of CBCTDocument93 pagesInterpretation of CBCTSagar Adhikari100% (4)
- Diaphragmatic Paralysis: Federico Minen Andreu Roca Bajona 30th September 2016Document42 pagesDiaphragmatic Paralysis: Federico Minen Andreu Roca Bajona 30th September 2016Sihome ThodireNo ratings yet
- Adult Chest X-RayDocument60 pagesAdult Chest X-RayAnil DasNo ratings yet
- Brain 2014 Yu Brain Awu239Document5 pagesBrain 2014 Yu Brain Awu239Angeles RbNo ratings yet
- Basic Chest X-Ray Interpretation (5minutes Talk) : DR - Alemayehu (ECCM R1)Document35 pagesBasic Chest X-Ray Interpretation (5minutes Talk) : DR - Alemayehu (ECCM R1)Alex beharuNo ratings yet
- Clinical Correlation Is NecessaryDocument1 pageClinical Correlation Is NecessaryRajesh SharmaNo ratings yet
- How To Read A Head CT ScanDocument34 pagesHow To Read A Head CT ScanBoby ArisofianNo ratings yet
- الترجمة التقنية الشبه نهائيDocument16 pagesالترجمة التقنية الشبه نهائيsalehaltiryNo ratings yet
- Grand Round Discussion: Dr. Nyaoncha A. NDocument36 pagesGrand Round Discussion: Dr. Nyaoncha A. NomoturetiNo ratings yet
- Epelman2010 Neonatal EncephalopathyDocument11 pagesEpelman2010 Neonatal EncephalopathyModou NianeNo ratings yet
- NEJM-Case 2-2023 - A 76-Year-Old Man With Dizziness and Altered Mental StatusDocument9 pagesNEJM-Case 2-2023 - A 76-Year-Old Man With Dizziness and Altered Mental StatussysysysyNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document6 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Riri KumalaNo ratings yet
- Large Arachnoid Cyst: T. Mondal K. Jagdish Kumar R. Anand N.K. Dubey D. SharmaDocument3 pagesLarge Arachnoid Cyst: T. Mondal K. Jagdish Kumar R. Anand N.K. Dubey D. SharmaJaya PrabhaNo ratings yet
- Molecular Investigation Into The Human Atrioventricular Node in Heart Failure 2161 0940.1000164Document8 pagesMolecular Investigation Into The Human Atrioventricular Node in Heart Failure 2161 0940.1000164Mei RieģoNo ratings yet
- Pushpa CT Head 62Document1 pagePushpa CT Head 62RAJESHNo ratings yet
- Hitrh JainDocument1 pageHitrh JainRAJESHNo ratings yet
- Sacks, Oliver - A Compulsive Collecting Behavior... (Letter) (2001)Document2 pagesSacks, Oliver - A Compulsive Collecting Behavior... (Letter) (2001)uerico roeheNo ratings yet
- Clinical Correlation Is NecessaryDocument1 pageClinical Correlation Is NecessaryrajeshsaloaNo ratings yet
- Clinical Correlation Is NecessaryDocument1 pageClinical Correlation Is NecessaryrajeshsaloaNo ratings yet
- Introduction To Critical Care USDocument39 pagesIntroduction To Critical Care USAntonio MedinaNo ratings yet
- Kanchan CT HesdDocument1 pageKanchan CT HesdrajeshcharakNo ratings yet
- Noninvasive Diagnosis of Vascular DiseaseFrom EverandNoninvasive Diagnosis of Vascular DiseaseFalls B. HersheyRating: 5 out of 5 stars5/5 (1)
- Mei 2018Document9 pagesMei 2018FidelisaNo ratings yet
- Transcranial Ultrasound Doppler Parameters in CereDocument7 pagesTranscranial Ultrasound Doppler Parameters in CereImin BuntaraNo ratings yet
- Reflective Learning in Higher Education - A Comparative AnalysisDocument8 pagesReflective Learning in Higher Education - A Comparative AnalysisChris LeeNo ratings yet
- The "Completely Randomised" and The "Randomised Block" Are The Only Experimental Designs Suitable For Widespread Use in Pre Clinical ResearchDocument5 pagesThe "Completely Randomised" and The "Randomised Block" Are The Only Experimental Designs Suitable For Widespread Use in Pre Clinical ResearchChris LeeNo ratings yet
- Reflections in LearningDocument17 pagesReflections in LearningChris LeeNo ratings yet
- Nursing Reflective Practice - An Empirical Literature ReviewDocument10 pagesNursing Reflective Practice - An Empirical Literature ReviewChris LeeNo ratings yet
- 3B User-Manual CPAP-Auto-CPAP RESmart BMC V1.7 ENG-1Document35 pages3B User-Manual CPAP-Auto-CPAP RESmart BMC V1.7 ENG-1Ricardo Costa CaribéNo ratings yet
- Reflection in and On Nursing Practices - How NursesDocument7 pagesReflection in and On Nursing Practices - How NursesChris LeeNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityChris LeeNo ratings yet
- 狗乾糧推薦名單2021Document5 pages狗乾糧推薦名單2021Chris LeeNo ratings yet
- Chemotherapy of Tuberculosis in Hong KongDocument17 pagesChemotherapy of Tuberculosis in Hong KongChris LeeNo ratings yet
- RESmart - CPAP, Auto - User ManualDocument40 pagesRESmart - CPAP, Auto - User ManualChris LeeNo ratings yet
- Arterial Blood Gas (ABG) Analysis: Normal ValuesDocument3 pagesArterial Blood Gas (ABG) Analysis: Normal ValuesNayem Hossain HemuNo ratings yet
- CAPD - StaySafe Training Manual PDFDocument16 pagesCAPD - StaySafe Training Manual PDFChris LeeNo ratings yet
- CT Scans of The Head: A Neurologist's PerspectiveDocument111 pagesCT Scans of The Head: A Neurologist's PerspectiveChris LeeNo ratings yet
- Terms of The Creative Commons Attribution Share Alike-3.0 LicenseDocument109 pagesTerms of The Creative Commons Attribution Share Alike-3.0 LicenseChris LeeNo ratings yet
- CT Head and Ischemic Cva: What To Look For On The Early Scan??Document19 pagesCT Head and Ischemic Cva: What To Look For On The Early Scan??Chris LeeNo ratings yet
- 12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramDocument66 pages12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramlalaNo ratings yet
- Pneumonia, Atelectasis & EffusionsDocument38 pagesPneumonia, Atelectasis & EffusionsChris LeeNo ratings yet
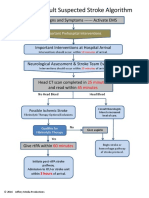
- Acute Stroke Management Resource:: Types of Stroke & Anatomy and Physiology of Acute StrokeDocument52 pagesAcute Stroke Management Resource:: Types of Stroke & Anatomy and Physiology of Acute StrokeChris LeeNo ratings yet
- 12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramDocument66 pages12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramlalaNo ratings yet
- Pneumonia, Atelectasis & EffusionsDocument38 pagesPneumonia, Atelectasis & EffusionsChris LeeNo ratings yet
- ACLS Stroke Algorithm PDFDocument1 pageACLS Stroke Algorithm PDFChris LeeNo ratings yet
- Cir 0000000000000613 PDFDocument10 pagesCir 0000000000000613 PDFDeivy De Jesus Cordoba SerratoNo ratings yet
- 2 4 Plasma ProductsDocument3 pages2 4 Plasma Productsشريف عبد المنعمNo ratings yet
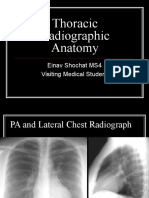
- Thoracic Radiographic Anatomy: Einav Shochat MS4 Visiting Medical StudentDocument81 pagesThoracic Radiographic Anatomy: Einav Shochat MS4 Visiting Medical StudentChris LeeNo ratings yet
- Nursing Tools Psychotherapy PDFDocument1 pageNursing Tools Psychotherapy PDFChris LeeNo ratings yet
- Catheter Care Guidelines PDFDocument45 pagesCatheter Care Guidelines PDFJayakumar JNo ratings yet
- Jama Echouffotcheugui 2023 RV 230007 1680895578.04302Document11 pagesJama Echouffotcheugui 2023 RV 230007 1680895578.04302Buton InspirasiNo ratings yet
- Oseltamivir (Tamifluw) and Its Potential For UseDocument17 pagesOseltamivir (Tamifluw) and Its Potential For UseRafael MusicasNo ratings yet
- GlaucomaDocument53 pagesGlaucomaLyNo ratings yet
- ACLS Drug TherapyDocument8 pagesACLS Drug TherapySahrensNo ratings yet
- 5BBK Lec5 - Other Blood Groups MQA 2019-09-26 08-14-44Document37 pages5BBK Lec5 - Other Blood Groups MQA 2019-09-26 08-14-44gothai sivapragasamNo ratings yet
- Oncology NCLEX Questions Flashcards - QuizletDocument50 pagesOncology NCLEX Questions Flashcards - QuizletGLORY MI SHANLEY CARUMBANo ratings yet
- Immunologic and Allergic DiseaseDocument49 pagesImmunologic and Allergic DiseaseFidz LiankoNo ratings yet
- HSE Bulletin - March 2024 - RamadanDocument2 pagesHSE Bulletin - March 2024 - RamadanraiavaniranjanNo ratings yet
- Nurses ChartingDocument2 pagesNurses ChartingdemethraNo ratings yet
- Defense Medical Epidemiology Database Report - Jan 26, 2022Document41 pagesDefense Medical Epidemiology Database Report - Jan 26, 2022adan_infowars100% (2)
- DOLICHOCOLONDocument6 pagesDOLICHOCOLONCassNo ratings yet
- Posterior Uveitis HandoutDocument4 pagesPosterior Uveitis Handoutdanny wiryaNo ratings yet
- Vestibular NeuronitisDocument3 pagesVestibular NeuronitisAnish RajNo ratings yet
- Is Vaginal Delivery or Caesarean Section The Safer Mode of Delivery in Patients With Adult Congenital Heart DiseaseDocument7 pagesIs Vaginal Delivery or Caesarean Section The Safer Mode of Delivery in Patients With Adult Congenital Heart DiseaseNathania TjuwatjaNo ratings yet
- Physical DisabilitiesDocument5 pagesPhysical Disabilitiesteachersmanual100% (2)
- Obsessive-Compulsive Disorder SectionDocument19 pagesObsessive-Compulsive Disorder Sectionark1974No ratings yet
- Adult Health - Soap Note 5Document3 pagesAdult Health - Soap Note 5api-546259691100% (3)
- AXR Made EasyDocument13 pagesAXR Made EasycswathikanNo ratings yet
- Joining InstructionsDocument30 pagesJoining InstructionsMuthike WachiraNo ratings yet
- HANDOUTS Brain SurgeryDocument3 pagesHANDOUTS Brain SurgerynieltresNo ratings yet
- Dental Treatment Considerations in The Chemotherapy PatientDocument12 pagesDental Treatment Considerations in The Chemotherapy PatientAdeel TahirNo ratings yet
- Universiti Kuala Lumpur Royal College of Medicine Perak: Year 3 Module Handbook (Medicine) 2014-2015Document15 pagesUniversiti Kuala Lumpur Royal College of Medicine Perak: Year 3 Module Handbook (Medicine) 2014-2015Codillia CheongNo ratings yet
- Abo Blood Group System GeneticsDocument17 pagesAbo Blood Group System GeneticsSYED MUHAMMAD ALI100% (1)
- Adex PearlsDocument7 pagesAdex PearlsLorenzini GrantNo ratings yet
- Hs TroponinDocument6 pagesHs TroponinNerhis Sydney WisakaNo ratings yet
- Module 3 FSIE BTVTED III A and BDocument10 pagesModule 3 FSIE BTVTED III A and BJhonnas obstaculoNo ratings yet
- Role of LABACS Provides A Simple and Effective For COPD and Asthma ManagementDocument74 pagesRole of LABACS Provides A Simple and Effective For COPD and Asthma ManagementHans WinardiNo ratings yet
- Pep 2021 - October QuestionsDocument4 pagesPep 2021 - October QuestionsCynthia ObiNo ratings yet
- Bilateral Peritonsillar AbscessDocument5 pagesBilateral Peritonsillar AbscessRadu BonaciuNo ratings yet
- Ortho Neck FemurDocument28 pagesOrtho Neck FemurgebyfondaNo ratings yet