You might also like
- Climbing PortugalDocument11 pagesClimbing Portugalhattori_gonzo0% (1)
- Diagnostic and Treatment Protocol For A Patient With TMD Using Stabilization Splint and TADDocument18 pagesDiagnostic and Treatment Protocol For A Patient With TMD Using Stabilization Splint and TADErna NaharuddinNo ratings yet
- AVEVA Everything 3D 2.1 Supports Chapter 14Document9 pagesAVEVA Everything 3D 2.1 Supports Chapter 14sanmiteNo ratings yet
- Orthodontic Treatment Protocols For Patients With Idiopathic Condylar ResorptionDocument13 pagesOrthodontic Treatment Protocols For Patients With Idiopathic Condylar ResorptionLESLY CATALINA GUZMAN CASTRONo ratings yet
- Progressive-Idiopathic Condylar Resorption - An Orthodontic PerspectiveDocument16 pagesProgressive-Idiopathic Condylar Resorption - An Orthodontic Perspective0308966uNo ratings yet
- Progressive Idiopathic Condylar Resorption - Three Case ReportsDocument14 pagesProgressive Idiopathic Condylar Resorption - Three Case ReportsCatalina Soler LioiNo ratings yet
- Idiopathic Condylar ResorptionbDocument12 pagesIdiopathic Condylar ResorptionbBelizNo ratings yet
- Sarver PDFDocument8 pagesSarver PDFanon_768201406No ratings yet
- Aaid Joi D 10 00056 - 1Document5 pagesAaid Joi D 10 00056 - 1Nora FarkashNo ratings yet
- Maloklusi - JournalDocument7 pagesMaloklusi - JournalarfahNo ratings yet
- Angle Orthod. 2023 93 1 49-56Document8 pagesAngle Orthod. 2023 93 1 49-56brookortontiaNo ratings yet
- Tibial Derotational Osteotomies in Two Neuromuscular PopulationsDocument6 pagesTibial Derotational Osteotomies in Two Neuromuscular PopulationsJuan Agustin Valcarce LeonNo ratings yet
- Resorcion Condilar Idiopatica PDFDocument7 pagesResorcion Condilar Idiopatica PDFJuan Carlos MeloNo ratings yet
- Fratura Condilar - AnquiloseDocument8 pagesFratura Condilar - AnquiloseMatheus MoraisNo ratings yet
- Wurgaft R, Rappoport K, Soler C, Ponce C, Flores-Mir CDocument16 pagesWurgaft R, Rappoport K, Soler C, Ponce C, Flores-Mir CCatalina Soler LioiNo ratings yet
- Hed 20192Document6 pagesHed 20192Tiago TavaresNo ratings yet
- 1 s2.0 S1079210400648655 MainDocument7 pages1 s2.0 S1079210400648655 Mainوليد محمد ابوعليNo ratings yet
- Surgical Management of Complex Mandibular Fracture: Case ReportDocument5 pagesSurgical Management of Complex Mandibular Fracture: Case ReportlindaNo ratings yet
- Uoi 114 HDocument6 pagesUoi 114 HashajangamNo ratings yet
- Osteosarcoma CondroblasticoDocument5 pagesOsteosarcoma CondroblasticoFrancis SortoNo ratings yet
- Management of Sub Condylar Fracture in 15 Yr Old Patient: Case ReportDocument6 pagesManagement of Sub Condylar Fracture in 15 Yr Old Patient: Case ReportIma ShofyaNo ratings yet
- Anehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesDocument7 pagesAnehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesHenry Adhy SantosoNo ratings yet
- Kjod 52 5 362Document10 pagesKjod 52 5 362khiemnguyen13No ratings yet
- "Unilateral Subcondylar Fracture Treated by Close Reduction: A CaseDocument3 pages"Unilateral Subcondylar Fracture Treated by Close Reduction: A CaseAlbertine JaneNo ratings yet
- Articular Disc Displacement Disorders and Its Prosthodontic Management: A Literature ReviewDocument9 pagesArticular Disc Displacement Disorders and Its Prosthodontic Management: A Literature ReviewTopan MuhamadNo ratings yet
- The Literature Review of Ollier DiseaseDocument8 pagesThe Literature Review of Ollier DiseaseCassNo ratings yet
- Pi Is 1991790212001626Document6 pagesPi Is 1991790212001626Lina NiatiNo ratings yet
- Displasia FibrosaDocument7 pagesDisplasia FibrosaRubi Diaz RomeroNo ratings yet
- MX - Stiff ElbowDocument8 pagesMX - Stiff ElbowPrabath ChinthakaNo ratings yet
- Arnett Combined Orthodontic and Surgical Open Bite CorrectionDocument12 pagesArnett Combined Orthodontic and Surgical Open Bite CorrectionAlex ReaNo ratings yet
- Surgical-Orthodontic Treatment For Severe Malocclusion in A Patient With Osteopetrosis and Bilateral Cleft Lip and Palate: Case Report With A 5-Year Follow-UpDocument9 pagesSurgical-Orthodontic Treatment For Severe Malocclusion in A Patient With Osteopetrosis and Bilateral Cleft Lip and Palate: Case Report With A 5-Year Follow-UpIslam GhorabNo ratings yet
- Art CXDocument9 pagesArt CXMilena RamirezNo ratings yet
- Correlations Between Malocclusion and Postural Anomalies in Children With Mixed DentitionDocument12 pagesCorrelations Between Malocclusion and Postural Anomalies in Children With Mixed DentitionMiguel candelaNo ratings yet
- Kaban2009 PDFDocument13 pagesKaban2009 PDFValsala UdayNo ratings yet
- Conservative Management of A Cervical Horizontal Root Fracture by Long Term StabilisationDocument4 pagesConservative Management of A Cervical Horizontal Root Fracture by Long Term StabilisationAlfonso SernaNo ratings yet
- Orthodontic Treatmentafter High Condylectomyin Patientswith Unilateral Condylar HyperplasiaDocument9 pagesOrthodontic Treatmentafter High Condylectomyin Patientswith Unilateral Condylar HyperplasiaOrtodoncia UNAL 2020No ratings yet
- Pédiatrie Elbow Trauma: An Orthopaedic Perspective On The Importance of Radiographie InterpretationDocument10 pagesPédiatrie Elbow Trauma: An Orthopaedic Perspective On The Importance of Radiographie InterpretationtripodegrandeNo ratings yet
- Management of Malocclusion After MaxillofacialDocument9 pagesManagement of Malocclusion After MaxillofacialZaimi Ginanjar Z GNo ratings yet
- Fractures of The Tibial PlafondDocument21 pagesFractures of The Tibial PlafondCamila FontechaNo ratings yet
- Broadie 2Document12 pagesBroadie 2Stefana NanuNo ratings yet
- Cirugia AtmDocument25 pagesCirugia AtmJuan Carlos SaavedraNo ratings yet
- Cleidocranial Dysplasia: Case Report of Three SiblingsDocument8 pagesCleidocranial Dysplasia: Case Report of Three SiblingsThang Nguyen TienNo ratings yet
- Distal Radius FractureDocument16 pagesDistal Radius FractureDeneishMuruNo ratings yet
- International Journal of Surgery Case Reports: Kanistika Jha, Manoj AdhikariDocument4 pagesInternational Journal of Surgery Case Reports: Kanistika Jha, Manoj AdhikariYeraldin EspañaNo ratings yet
- A. Congenital Radioulnar Synostosis: Self-Directed LearningDocument6 pagesA. Congenital Radioulnar Synostosis: Self-Directed Learningapi-477982644No ratings yet
- Adult Langerhans Cell Histiocytosis With A Rare BRAF - 2022 - Advances in Oral ADocument3 pagesAdult Langerhans Cell Histiocytosis With A Rare BRAF - 2022 - Advances in Oral Ag.abdulrhmanNo ratings yet
- Anterior Open Bite With ICR HistoryDocument12 pagesAnterior Open Bite With ICR HistoryKanchit SuwanswadNo ratings yet
- A Rare Case Report Along With Surgical Management of Bilateral Maxillary Buccal Exostosis in A Patient of Polydactyly and Distomol.Document3 pagesA Rare Case Report Along With Surgical Management of Bilateral Maxillary Buccal Exostosis in A Patient of Polydactyly and Distomol.Fransiski HoNo ratings yet
- The Journal of Foot & Ankle SurgeryDocument5 pagesThe Journal of Foot & Ankle SurgeryGilbert Tormis DaguploNo ratings yet
- DL TPSFDocument5 pagesDL TPSFPramod N KNo ratings yet
- Intramedullary Nailing of Distal Metaphyseal.5Document9 pagesIntramedullary Nailing of Distal Metaphyseal.5Joël Clarck EkowongNo ratings yet
- AAOS2002 TumorDocument59 pagesAAOS2002 TumorHizkyas KassayeNo ratings yet
- Manson1974 PDFDocument5 pagesManson1974 PDFharithrra vNo ratings yet
- The Role of Craniofacial Distraction in Contemporary OrthodonticsDocument10 pagesThe Role of Craniofacial Distraction in Contemporary OrthodonticswjeelaniNo ratings yet
- CA LS Bướu Nhiều Hốc - Multilocular Radiolucency in the Body of MandibleDocument4 pagesCA LS Bướu Nhiều Hốc - Multilocular Radiolucency in the Body of MandibleThành Luân NguyễnNo ratings yet
- Pi Is 0889540613006197Document3 pagesPi Is 0889540613006197mutiaNo ratings yet
- TENS HúmeroDocument7 pagesTENS HúmeronetongasNo ratings yet
- Pos Nick 2004Document16 pagesPos Nick 2004Bhárbara Marinho BarcellosNo ratings yet
- Craniofacial Syndromes.33Document26 pagesCraniofacial Syndromes.33andrew kilshawNo ratings yet
- Nils Worsaae1994Document8 pagesNils Worsaae1994João Paulo DutraNo ratings yet
- Hip Disorders in Children: Postgraduate Orthopaedics SeriesFrom EverandHip Disorders in Children: Postgraduate Orthopaedics SeriesRating: 3 out of 5 stars3/5 (2)
- Dislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementFrom EverandDislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementNigel Shaun MatthewsNo ratings yet
- Tekin - Comparative Determination of Skeletal Maturity by Hand-WristDocument10 pagesTekin - Comparative Determination of Skeletal Maturity by Hand-WristCatherine NocuaNo ratings yet
- Sachez, Arriola - Reliability of Cephalograms Derived of Cone BeamDocument8 pagesSachez, Arriola - Reliability of Cephalograms Derived of Cone BeamCatherine NocuaNo ratings yet
- Amasya-Validation of Cervical Vertebral Maturation Stages Artificial Intelligence Vs Human Observer Visual AnalysisDocument7 pagesAmasya-Validation of Cervical Vertebral Maturation Stages Artificial Intelligence Vs Human Observer Visual AnalysisCatherine NocuaNo ratings yet
- Kok - Usage and Comparison of Artificial AlgorithmsDocument10 pagesKok - Usage and Comparison of Artificial AlgorithmsCatherine NocuaNo ratings yet
- Demirjian - A New System of Dental Age Assessment.Document18 pagesDemirjian - A New System of Dental Age Assessment.Catherine NocuaNo ratings yet
- Tsubota 2009Document7 pagesTsubota 2009Catherine NocuaNo ratings yet
- Rho 1998Document11 pagesRho 1998Catherine NocuaNo ratings yet
- Use of Laser Systems in OrthodonticsDocument8 pagesUse of Laser Systems in OrthodonticsCatherine NocuaNo ratings yet
- BoneTissueandBiomaterialDesignBasedontheAnisotropicMicrostreucture-TakayoshiNAKANOetalAdvances in Metallic BiomaterDocument32 pagesBoneTissueandBiomaterialDesignBasedontheAnisotropicMicrostreucture-TakayoshiNAKANOetalAdvances in Metallic BiomaterCatherine NocuaNo ratings yet
- Comparison of Conventional and Laser-Aided Fiberetomy in Relapse Tendency of Rotated ToothDocument11 pagesComparison of Conventional and Laser-Aided Fiberetomy in Relapse Tendency of Rotated ToothCatherine NocuaNo ratings yet
- Orthodontic Relapse Versus Natural DevelopmentDocument2 pagesOrthodontic Relapse Versus Natural DevelopmentCatherine NocuaNo ratings yet
- University of Lisbon Institute of Social SciencesDocument288 pagesUniversity of Lisbon Institute of Social SciencesAnastasiya MytkoNo ratings yet
- Loan Officer Financial Sales in Houston TX Resume Ralph GardnerDocument1 pageLoan Officer Financial Sales in Houston TX Resume Ralph GardnerRalphGardnerNo ratings yet
- Checklist For Hospital For Data CollectionDocument8 pagesChecklist For Hospital For Data CollectionMuhammad Nadeem NasirNo ratings yet
- DEPEDBATS CID F 009 Pre Obsevation Conference English and FilipinoDocument4 pagesDEPEDBATS CID F 009 Pre Obsevation Conference English and FilipinoAngelo VillafrancaNo ratings yet
- BBVA Continental-Preliminary Offering Circular PDFDocument362 pagesBBVA Continental-Preliminary Offering Circular PDFfanatico1982No ratings yet
- Tanzania National Business CouncilDocument5 pagesTanzania National Business CouncilNakul ChandakNo ratings yet
- April Bayer Resume 2018Document1 pageApril Bayer Resume 2018api-395856965No ratings yet
- Leadscrews Ballscrews Splines CtenDocument236 pagesLeadscrews Ballscrews Splines CtenTony BeltranNo ratings yet
- Karnataka Apartment Act 1972Document7 pagesKarnataka Apartment Act 1972cnath_1No ratings yet
- 10 Principles of EconomicsDocument12 pages10 Principles of EconomicsAbdul Rehman AhmadNo ratings yet
- HV Book Complete PDFDocument129 pagesHV Book Complete PDFseeb19100% (1)
- Uae Oil Gas DirectoryDocument262 pagesUae Oil Gas DirectoryVincs100% (1)
- Transportation Management ModuleDocument58 pagesTransportation Management Modulecathy palomoNo ratings yet
- E406 81 (2012)Document4 pagesE406 81 (2012)diego rodriguezNo ratings yet
- Chapter 9-Center of Gravity and Centroids-OdatDocument74 pagesChapter 9-Center of Gravity and Centroids-OdatMohammed Al-OdatNo ratings yet
- 3.4 Hazards/Glitches and How To Avoid Them: 3.4.1 The Problem With HazardsDocument8 pages3.4 Hazards/Glitches and How To Avoid Them: 3.4.1 The Problem With HazardsHarish KumarNo ratings yet
- Gta Eflc Car Mods v3.5 ReadmeDocument6 pagesGta Eflc Car Mods v3.5 ReadmeAdrian MandacheNo ratings yet
- What A Language Student Should Learn?: NeedsDocument8 pagesWhat A Language Student Should Learn?: Needsmonday bluesNo ratings yet
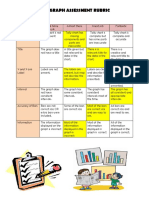
- Shelby Bar Graph Assessment RubricDocument1 pageShelby Bar Graph Assessment Rubricapi-360512521No ratings yet
- Questionnaire Sections A B and C ..KamamaDocument7 pagesQuestionnaire Sections A B and C ..KamamaJoseph KamenyaNo ratings yet
- Ireland Financial CrisisDocument15 pagesIreland Financial Crisissantaukura2No ratings yet
- Statistics and Probability Beed2b Instructional Planning ModelfinalDocument15 pagesStatistics and Probability Beed2b Instructional Planning ModelfinalRiza ReambonanzaNo ratings yet
- PK PD Relationships SummaryDocument2 pagesPK PD Relationships Summarynick224No ratings yet
- Iexpenses Overview 1Document48 pagesIexpenses Overview 1rcp.generalNo ratings yet
- GCS Course Flyer UpdatedDocument8 pagesGCS Course Flyer Updatedજીસીએસ હોસ્પિટલNo ratings yet
- 9708 s06 QP 3Document12 pages9708 s06 QP 3icicle_skyNo ratings yet
- P3 Integration FormulaDocument6 pagesP3 Integration FormulaRahyan AshrafNo ratings yet
- Chem Academy: Daily Assignment Iit-Jam Home Work DPPDocument4 pagesChem Academy: Daily Assignment Iit-Jam Home Work DPPVkumar100% (1)