You might also like
- Prematurity OSCE Counselling Child Health Paediatric Non-Clinical Patient EncounterDocument5 pagesPrematurity OSCE Counselling Child Health Paediatric Non-Clinical Patient EncounterJJ LimNo ratings yet
- Pedia QuizesDocument19 pagesPedia QuizesPraneeth PaletiNo ratings yet
- Case 9: 2-Week-Old With Lethargy - CrimsonDocument7 pagesCase 9: 2-Week-Old With Lethargy - Crimsonalwaysbeclosing52No ratings yet
- Construction Site PremisesDocument78 pagesConstruction Site PremisesDrew B Mrtnz67% (6)
- Preformed Expansion Joint Filler For Concrete (Bituminous Type)Document2 pagesPreformed Expansion Joint Filler For Concrete (Bituminous Type)Katerin HernandezNo ratings yet
- 11 - FORAGERS by Sam BoyerDocument106 pages11 - FORAGERS by Sam BoyerMurtaza HussainNo ratings yet
- Factory made uPVC windows installationDocument2 pagesFactory made uPVC windows installationAmit Singh100% (2)
- Medical Management of Children With Down SyndromeDocument8 pagesMedical Management of Children With Down SyndromeMariana OrozcoNo ratings yet
- Down Screen Proposal For Health Screen at Thyrocare AmitDocument19 pagesDown Screen Proposal For Health Screen at Thyrocare AmitSwatiSuranaNo ratings yet
- Perinatal Medicine GuideDocument7 pagesPerinatal Medicine GuideMerna MahrousNo ratings yet
- CF and SidsDocument7 pagesCF and SidsEira LopezNo ratings yet
- Group-3 Ncm109 Trisonomy18Document8 pagesGroup-3 Ncm109 Trisonomy18JOHN ROIENo ratings yet
- Obg PPT 1Document27 pagesObg PPT 1yash myatraNo ratings yet
- Intra Uterine Growth RetardationDocument46 pagesIntra Uterine Growth RetardationIba Ghannam100% (1)
- Risks of Preterm, SGA, LGA and Newborn ComplicationsDocument6 pagesRisks of Preterm, SGA, LGA and Newborn ComplicationsAlyssa DeleonNo ratings yet
- Preterm Birth and ComplicationsDocument5 pagesPreterm Birth and Complicationsandrahlyn100% (1)
- Term PaperDocument85 pagesTerm PaperAbhilash PaulNo ratings yet
- Respiratory Distress Syndrome & PrematureDocument48 pagesRespiratory Distress Syndrome & PrematureDivieya Tharisini KrisnanNo ratings yet
- Lagan 2020Document16 pagesLagan 2020Aurha Akmal GinarisNo ratings yet
- Care of at-risk mothers and childrenDocument7 pagesCare of at-risk mothers and childrenJumamoy, Bea ArabelaNo ratings yet
- Edwards Down SyndromeDocument5 pagesEdwards Down Syndromeapi-346355246No ratings yet
- Pediatric pregnancy complicated by viral infectionsDocument17 pagesPediatric pregnancy complicated by viral infectionsSherilyn Joy AdelNo ratings yet
- Birth Defects 1Document38 pagesBirth Defects 1SaidNo ratings yet
- A Premature Infant Is An Infant Born Before 37 WK GestationDocument5 pagesA Premature Infant Is An Infant Born Before 37 WK GestationKamila KawaiiNo ratings yet
- Síndrome de PotterDocument4 pagesSíndrome de Potternaomi orozcoNo ratings yet
- Fetal Mediine PDFDocument5 pagesFetal Mediine PDFDr.yeasin ArafatNo ratings yet
- English in Paediatrics 2: Textbook for Mothers, Babysitters, Nurses, and PaediatriciansFrom EverandEnglish in Paediatrics 2: Textbook for Mothers, Babysitters, Nurses, and PaediatriciansNo ratings yet
- Care of Preterm Babies FinalDocument33 pagesCare of Preterm Babies Finalchinchu100% (1)
- General EmbryologyDocument41 pagesGeneral EmbryologyRiya SinghNo ratings yet
- Down Syndrome Scott DunlopDocument3 pagesDown Syndrome Scott DunlopYwagar YwagarNo ratings yet
- NCM 109 PEDIA PPT 2 High Risk Infant A New Pre TermDocument72 pagesNCM 109 PEDIA PPT 2 High Risk Infant A New Pre TermJoyce EricaNo ratings yet
- Plabable 2020 Pediatrics 1uvDocument89 pagesPlabable 2020 Pediatrics 1uvRajesh Kumar Asunala100% (1)
- Pediatric MCQ Questions on Neuropathies, Genitalia, Heart Defects and MoreDocument17 pagesPediatric MCQ Questions on Neuropathies, Genitalia, Heart Defects and MoreAhmed Kassem100% (1)
- Downs SyndromeDocument8 pagesDowns Syndromezainab sarhanNo ratings yet
- Sudden Infant Death Syndrome (SIDS)Document4 pagesSudden Infant Death Syndrome (SIDS)Julliza Joy PandiNo ratings yet
- English in Paediatrics 1: Textbook for Mothers, Caregivers, Nurses and PaediatriciansFrom EverandEnglish in Paediatrics 1: Textbook for Mothers, Caregivers, Nurses and PaediatriciansRating: 5 out of 5 stars5/5 (1)
- Congenital and Hereditary Diseases Introduction-1Document21 pagesCongenital and Hereditary Diseases Introduction-1Melvin OnyanchaNo ratings yet
- Prematurity to Postmaturity: Nursing Care for Preterm and Post-Term NewbornsDocument38 pagesPrematurity to Postmaturity: Nursing Care for Preterm and Post-Term NewbornsJessy Arcaina BañagaNo ratings yet
- Nada's Pediatric Path ReviewDocument16 pagesNada's Pediatric Path ReviewNada MuchNo ratings yet
- DevelopmentDocument15 pagesDevelopmentagustinus salimNo ratings yet
- Hydrops FetalisDocument4 pagesHydrops FetalisAngelito LeritNo ratings yet
- Down SyndromeDocument4 pagesDown SyndromeninaersNo ratings yet
- Newborn Screening Blood Tests Detect Rare DisordersDocument2 pagesNewborn Screening Blood Tests Detect Rare DisordersYwagar YwagarNo ratings yet
- JP 2014116Document5 pagesJP 2014116koas forensikNo ratings yet
- Homework PreemiDocument8 pagesHomework PreemiTeenie Guerrero-GarciaNo ratings yet
- NCLEX Tips On ProceduresDocument4 pagesNCLEX Tips On Proceduresromin_soledad100% (7)
- Down Syndrom (Eng)Document11 pagesDown Syndrom (Eng)Echa MagungNo ratings yet
- High Risk NewbornDocument25 pagesHigh Risk NewbornViji MNo ratings yet
- Definition: Down Syndrome, Down's Syndrome, or Trisomy 21 Is A Chromosomal Disorder Caused by TheDocument3 pagesDefinition: Down Syndrome, Down's Syndrome, or Trisomy 21 Is A Chromosomal Disorder Caused by TheLove Shery SabrosoNo ratings yet
- Down Syndrome PresentationDocument43 pagesDown Syndrome Presentationapi-509245925No ratings yet
- Case Report For Case Presentations Short Rib Polydactyly SyndromeDocument8 pagesCase Report For Case Presentations Short Rib Polydactyly Syndromeapi-390240132No ratings yet
- SGD Pedia: Pruritus SGD Pedia: Pruritus: Amy Luz T. Corpuz, M.D. DPPS, MPH Amy Luz T. Corpuz, M.D. DPPS, MPHDocument14 pagesSGD Pedia: Pruritus SGD Pedia: Pruritus: Amy Luz T. Corpuz, M.D. DPPS, MPH Amy Luz T. Corpuz, M.D. DPPS, MPHNewbornMed FABELLANo ratings yet
- High Risk Infant-1Document5 pagesHigh Risk Infant-1MauZungNo ratings yet
- Spina Bifida Guide: Types, Causes & Nursing CareDocument5 pagesSpina Bifida Guide: Types, Causes & Nursing CareJulliza Joy PandiNo ratings yet
- Letter From PhysiciansDocument6 pagesLetter From PhysiciansABC Action NewsNo ratings yet
- Final Theoretical Exam in Pediatrics " Set A ": Choose The Most Appropriate ResponseDocument54 pagesFinal Theoretical Exam in Pediatrics " Set A ": Choose The Most Appropriate ResponseYousif AlaaNo ratings yet
- Azazim 2012 PDFDocument27 pagesAzazim 2012 PDFShowmik PaulNo ratings yet
- Assignment ON Identification, Classification & Nursing Management of High Risk NewbornDocument18 pagesAssignment ON Identification, Classification & Nursing Management of High Risk NewbornSanthosh.S.U100% (1)
- Pediatrics 2005 Trotter 771 83Document16 pagesPediatrics 2005 Trotter 771 83Ligia RiosNo ratings yet
- Hematologic Disorders PowerpointDocument51 pagesHematologic Disorders PowerpointjoycechicagoNo ratings yet
- Genetic Disorders at Haramaya UniversityDocument32 pagesGenetic Disorders at Haramaya UniversityMerwan KemalNo ratings yet
- Prematurity: Signs and SymptomsDocument13 pagesPrematurity: Signs and SymptomsGladie Ann Dela RosaNo ratings yet
- Urosepsis Is The Most Common Complication of Purn-Belly SyndromeDocument4 pagesUrosepsis Is The Most Common Complication of Purn-Belly Syndromeraisa desti ardiantyNo ratings yet
- Iufd Bali 2006Document26 pagesIufd Bali 2006Andy YusrizalNo ratings yet
- 2008 Infosys Model QuestionsDocument23 pages2008 Infosys Model Questionsapi-3824713No ratings yet
- Category D Fluid ServiceDocument2 pagesCategory D Fluid Serviceaslam.ambNo ratings yet
- HEAT EFFECTS (Cha 4) : Outline of Chapter OneDocument65 pagesHEAT EFFECTS (Cha 4) : Outline of Chapter OneAdam MekonnenNo ratings yet
- Thalassemia: Submitted By: Jovan Pierre C. Ouano Submitted To: Mark Gil T. DacutanDocument8 pagesThalassemia: Submitted By: Jovan Pierre C. Ouano Submitted To: Mark Gil T. DacutanJvnpierre AberricanNo ratings yet
- BrosurDocument68 pagesBrosurKiki Xhui7No ratings yet
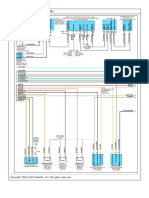
- Liebert AC4 Controller ManualDocument88 pagesLiebert AC4 Controller ManualGreg WilliamsNo ratings yet
- Studyguide TracksDocument75 pagesStudyguide TracksAnonymous FabB2WJl485% (13)
- Fire and Blast in The Future OffshoreDocument45 pagesFire and Blast in The Future OffshoredrgNo ratings yet
- Script For TSB GRDDocument9 pagesScript For TSB GRDJuvel OrquinazaNo ratings yet
- Encore 700 Diaphragm Pump 1Document12 pagesEncore 700 Diaphragm Pump 1bagurtoNo ratings yet
- SGDJ PDFDocument334 pagesSGDJ PDFDouglas Rogério de CastroNo ratings yet
- S2 Papers FinalizedDocument149 pagesS2 Papers FinalizedRaffles HolmesNo ratings yet
- Kyocera Fs-6900 Parts ManualDocument28 pagesKyocera Fs-6900 Parts ManualNic CowpeNo ratings yet
- Girbau STI-54 STI-77 Parts ManualDocument74 pagesGirbau STI-54 STI-77 Parts Manualrpm14sheratonbsasNo ratings yet
- NOISE ANALYSISDocument16 pagesNOISE ANALYSISDiana Rose TapelNo ratings yet
- Treatment of Headaches in The ED With Lower Cervical Intramuscular Bupivacaine Injections: A 1-Year Retrospective Review of 417 PatientsDocument9 pagesTreatment of Headaches in The ED With Lower Cervical Intramuscular Bupivacaine Injections: A 1-Year Retrospective Review of 417 PatientsLarry B. Mellick, MDNo ratings yet
- Plasma ChemistryDocument6 pagesPlasma ChemistryArief RomadhonNo ratings yet
- 9709 s15 QP 12Document4 pages9709 s15 QP 12Abrar JahinNo ratings yet
- General Biology 1: Go Fast, or Slow Down?Document23 pagesGeneral Biology 1: Go Fast, or Slow Down?Mikhael OiraNo ratings yet
- QRP Yu1lm SDR-RX TXDocument299 pagesQRP Yu1lm SDR-RX TXD BNo ratings yet
- AbstractDocument2 pagesAbstractramyaNo ratings yet
- Diagrama 4 AMBIENT AIR TEMPER..Document1 pageDiagrama 4 AMBIENT AIR TEMPER..Gustavo PérezNo ratings yet
- Cse Reviewer - MathDocument58 pagesCse Reviewer - MathLyne LerinNo ratings yet
- Popular CultureDocument25 pagesPopular CultureVibhuti KachhapNo ratings yet
- Mohair FiberDocument33 pagesMohair FiberMuhammad Ahsan AftabNo ratings yet
- Giddings & Lewis Sect08 HydDocument24 pagesGiddings & Lewis Sect08 HydAngel AdautaNo ratings yet