You might also like
- First Year Critical Appraisal Randomize Control TrialDocument4 pagesFirst Year Critical Appraisal Randomize Control Trialapi-615708784No ratings yet
- Reviewer:: Jbisynthesis@adelaide - Edu.auDocument7 pagesReviewer:: Jbisynthesis@adelaide - Edu.auapi-676766856No ratings yet
- Article Appraisal 1Document5 pagesArticle Appraisal 1api-670980669No ratings yet
- Article 1 AppraisalDocument4 pagesArticle 1 Appraisalapi-621026204No ratings yet
- Critical Apprasisal 1Document5 pagesCritical Apprasisal 1api-622033233No ratings yet
- Critical Apprasisal of RCT Thompson 1Document5 pagesCritical Apprasisal of RCT Thompson 1api-677601309No ratings yet
- Critical Apprasisal of RCTDocument6 pagesCritical Apprasisal of RCTapi-678649411No ratings yet
- Critical Apprasisal 2Document5 pagesCritical Apprasisal 2api-678326591No ratings yet
- Checklist - Hyperbaric Treatment For Children With Autism A MulticenterDocument3 pagesChecklist - Hyperbaric Treatment For Children With Autism A MulticenterJim GoetzNo ratings yet
- Users' Guide: Assessing Study Validity and ResultsDocument2 pagesUsers' Guide: Assessing Study Validity and ResultsnjunaidiNo ratings yet
- Critical AppraisalDocument47 pagesCritical AppraisalNaman KhalidNo ratings yet
- Controlled Trial Methodology ChecklistDocument4 pagesControlled Trial Methodology ChecklistriiaayuNo ratings yet
- Appraising The Evidence Critical AppraisalDocument47 pagesAppraising The Evidence Critical AppraisalMuhammad Rizki PratamaNo ratings yet
- Therapy Appraisalform 2004RDocument3 pagesTherapy Appraisalform 2004RpurletpunkNo ratings yet
- Therapy Worksheet 2Document1 pageTherapy Worksheet 2stylesh828No ratings yet
- Controlled Trials Methodology ChecklistDocument3 pagesControlled Trials Methodology ChecklistPanggih SaputroNo ratings yet
- Critical Appraisal JRDocument3 pagesCritical Appraisal JRRizky AgustriaNo ratings yet
- Tugas Terapi Modalitas Keperawatan Chronic Kidney Disease (CKD)Document7 pagesTugas Terapi Modalitas Keperawatan Chronic Kidney Disease (CKD)Winda WidyaNo ratings yet
- Checklist RCTDocument5 pagesChecklist RCTFajar SukmajayaNo ratings yet
- Dan - Patinet ReluctanceDocument6 pagesDan - Patinet Reluctanceamandeep khuranaNo ratings yet
- PENANG MEDICAL COLLEGE Critical Appraisal TherapyDocument3 pagesPENANG MEDICAL COLLEGE Critical Appraisal TherapyRebecca WongNo ratings yet
- EBP Presentation by Group 2Document25 pagesEBP Presentation by Group 2Dr-Muhammad QasimNo ratings yet
- GROUP THERAPY IN THE CANCER SETTING - Fawzy and Fawzy 1998Document10 pagesGROUP THERAPY IN THE CANCER SETTING - Fawzy and Fawzy 1998Manuel PernetasNo ratings yet
- Critical Appraisal: Prof. Dr. Mohammad Hakimi, Spog (K), PHDDocument37 pagesCritical Appraisal: Prof. Dr. Mohammad Hakimi, Spog (K), PHDFebbty KuswantiNo ratings yet
- Article 2 RCADocument4 pagesArticle 2 RCAHeather CunninghamNo ratings yet
- 1-Critical Appraisal For RCT and Other Interventional StudiesDocument2 pages1-Critical Appraisal For RCT and Other Interventional StudiesCharles Kyalo NyamaiNo ratings yet
- Effects of Massage and Acupressure On Relieving Labor Pain, Reducing Labor Time, and Increasing Delivery SatisfactionDocument3 pagesEffects of Massage and Acupressure On Relieving Labor Pain, Reducing Labor Time, and Increasing Delivery SatisfactionNuryn UridhaNo ratings yet
- Study Analysis and CritiqueDocument3 pagesStudy Analysis and Critique7lightbourn5893No ratings yet
- Do Empirically Supported Treatments Generalize To Private Practice? 1Document8 pagesDo Empirically Supported Treatments Generalize To Private Practice? 1api-340608725No ratings yet
- Jbi Critical Appraisal Checklist For Randomized Controlled TrialsDocument4 pagesJbi Critical Appraisal Checklist For Randomized Controlled TrialsNatasya Cindy SaraswatiNo ratings yet
- TMK - Kelompok CKDDocument13 pagesTMK - Kelompok CKDWinda WidyaNo ratings yet
- Acfrogablxota17ubsxnocf0sulcs0yxzk1ieqobaba89fhirrp9afgxsi M9trrmjbw59ygqyimsoeb8 Osuisry2soyu6xf3uboxnu6h6m-90ibt61hjz-Uiufefcefptktzfol3ccisa W VJDocument5 pagesAcfrogablxota17ubsxnocf0sulcs0yxzk1ieqobaba89fhirrp9afgxsi M9trrmjbw59ygqyimsoeb8 Osuisry2soyu6xf3uboxnu6h6m-90ibt61hjz-Uiufefcefptktzfol3ccisa W VJKarylle RiveroNo ratings yet
- Resmume Jurnal JiwaDocument3 pagesResmume Jurnal Jiwaanj arNo ratings yet
- Nursing Research ExamDocument3 pagesNursing Research ExamAyanne Arcena70% (10)
- Critical Apraisal CitaDocument4 pagesCritical Apraisal Citamarhayudi15No ratings yet
- Therapystudy: Are The Results of The Trial Valid? (Internal Validity)Document10 pagesTherapystudy: Are The Results of The Trial Valid? (Internal Validity)WiraNo ratings yet
- Relationship between hypertension control and cardiovascular risk factorsDocument3 pagesRelationship between hypertension control and cardiovascular risk factorsRezki Pratama SadeliNo ratings yet
- Awad2000 Determinants in Patients PreferencesDocument7 pagesAwad2000 Determinants in Patients Preferenceslaur112233No ratings yet
- JC Presentation FormatDocument12 pagesJC Presentation FormatNikitha AshokNo ratings yet
- Checklist To Appraise RCTsDocument1 pageChecklist To Appraise RCTsrisha7No ratings yet
- N375 Critical Thinking Activity ExampleDocument6 pagesN375 Critical Thinking Activity ExamplefaizaNo ratings yet
- A Strategy To Advance The Evidence Base in Palliative Medicine: Formation of A Palliative Care Research Cooperative GroupDocument8 pagesA Strategy To Advance The Evidence Base in Palliative Medicine: Formation of A Palliative Care Research Cooperative GroupLLloydNo ratings yet
- RCT GuideDocument29 pagesRCT Guidemvs hardhikNo ratings yet
- Intervencionbueno FullDocument6 pagesIntervencionbueno FullfafiscribdNo ratings yet
- Community Medicine: DesignDocument6 pagesCommunity Medicine: Designapi-3829364No ratings yet
- Diy RCT AppraisalDocument43 pagesDiy RCT AppraisalimperiallightNo ratings yet
- Post Test Nursing ResearchDocument7 pagesPost Test Nursing ResearchPrince Jhessie L. AbellaNo ratings yet
- Franchie M. HsuDocument2 pagesFranchie M. HsuFranchieNo ratings yet
- Not All Patiens Want To ParticipateDocument5 pagesNot All Patiens Want To ParticipateAmelia ArnisNo ratings yet
- Critical Appraisal of Cohort Studies EBMP 1000e108Document2 pagesCritical Appraisal of Cohort Studies EBMP 1000e108thetaggerung100% (1)
- Davis Ak, Barrett FS, May DG, Et Al. No CancerDocument2 pagesDavis Ak, Barrett FS, May DG, Et Al. No Cancercameron pollardNo ratings yet
- PH 210: Epidemiology For Public Health Practice Dr. Grosskopf Post-Class Activity: Experimental Studies ANSWERSDocument1 pagePH 210: Epidemiology For Public Health Practice Dr. Grosskopf Post-Class Activity: Experimental Studies ANSWERSMelodic DubzNo ratings yet
- Biostatistics Refresher WB PHDocument24 pagesBiostatistics Refresher WB PHreham ONo ratings yet
- Srep 25325Document9 pagesSrep 25325Marco NgNo ratings yet
- Checklist Critical Appraisal Cross SectionalDocument2 pagesChecklist Critical Appraisal Cross SectionalDewii YuliianaNo ratings yet
- Therapy Worksheet Undergraduate Feb 2008 ExplainedDocument3 pagesTherapy Worksheet Undergraduate Feb 2008 ExplainedstylussimoNo ratings yet
- Team-Based Oncology Care: The Pivotal Role of Oncology NavigationFrom EverandTeam-Based Oncology Care: The Pivotal Role of Oncology NavigationLillie D. ShockneyNo ratings yet
- PCORI Methodology Standards Curriculum Research Questions 3Document13 pagesPCORI Methodology Standards Curriculum Research Questions 3Krizele Acu PagalananNo ratings yet
- Kelompok CKD - Tugas Terapi Modalitas KeperawatanDocument14 pagesKelompok CKD - Tugas Terapi Modalitas KeperawatanWinda WidyaNo ratings yet
- Ambers Resume PDFDocument1 pageAmbers Resume PDFapi-619891965No ratings yet
- Hip Interventions ProjectDocument3 pagesHip Interventions Projectapi-619891965No ratings yet
- Reflection Narrative For PortfolioDocument2 pagesReflection Narrative For Portfolioapi-619891965No ratings yet
- Knee Interventions Project Little SchoenickeDocument3 pagesKnee Interventions Project Little Schoenickeapi-619891965No ratings yet
- Pth636-Case6 With FeedbackDocument2 pagesPth636-Case6 With Feedbackapi-619891965No ratings yet
- Article 2 AppraisalDocument5 pagesArticle 2 Appraisalapi-619891965No ratings yet
- The Effect of Potassium Permanganate (KMnO4) Concentration and Storage Time on Quality of California Papaya (Carica papaya LDocument8 pagesThe Effect of Potassium Permanganate (KMnO4) Concentration and Storage Time on Quality of California Papaya (Carica papaya LSyifa UlNo ratings yet
- Ethics of Blood TransfusionDocument6 pagesEthics of Blood TransfusionHo Yong WaiNo ratings yet
- Unit 4 CommunicationDocument3 pagesUnit 4 Communicationsutarmisaja15No ratings yet
- Exercises For Task 3 InglesDocument3 pagesExercises For Task 3 InglesNoelia De Los SantosNo ratings yet
- Leni Robredo CredentialsDocument2 pagesLeni Robredo CredentialsJhelliene Rose V. De CastroNo ratings yet
- Midwifery LedDocument15 pagesMidwifery LedRizka Dita Hidayati100% (1)
- Affidavit of Accident Dominador Rosario BagamaspadDocument2 pagesAffidavit of Accident Dominador Rosario BagamaspadJaime GonzalesNo ratings yet
- Giraffe and Panda Warmer TRM M1128921 Rev PDocument230 pagesGiraffe and Panda Warmer TRM M1128921 Rev PRonnelSerranoNo ratings yet
- BSBMKG502 Task 2Document9 pagesBSBMKG502 Task 2Diana PulidoNo ratings yet
- Apply teacher short leaveDocument1 pageApply teacher short leaveJean Claudine MandayNo ratings yet
- Couchiching FN Toll BoothDocument8 pagesCouchiching FN Toll BoothpegspirateNo ratings yet
- NCM 101 Vital Signs PPT BSN 1a Group 1Document138 pagesNCM 101 Vital Signs PPT BSN 1a Group 1Brian Anthony100% (1)
- Theory Critique of Boundaries in MarriageDocument8 pagesTheory Critique of Boundaries in MarriagepatrickakingNo ratings yet
- Introduction To The Alpaca andDocument9 pagesIntroduction To The Alpaca andMai Chi PhạmNo ratings yet
- Atkinson R L - Weight CyclingDocument7 pagesAtkinson R L - Weight CyclingmaddafackerNo ratings yet
- Human Population and EnvironmentDocument4 pagesHuman Population and Environmentmonkeybike88No ratings yet
- Anatomia SufletuluiDocument1 pageAnatomia SufletuluiAlexandrina DeaşNo ratings yet
- 4.schedule Waste Management UTM - SWMP - 22mei2018 PDFDocument54 pages4.schedule Waste Management UTM - SWMP - 22mei2018 PDFfaraNo ratings yet
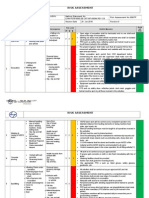
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- Que No4 & 5-With Clues and Without CluesDocument4 pagesQue No4 & 5-With Clues and Without CluesMir Yamin Uddin ZidanNo ratings yet
- Careers Surrey 20181Document15 pagesCareers Surrey 20181Kevin_Nguyen117No ratings yet
- Petroleum Gases, Liquefied Petroleum Gas: IdentificationDocument4 pagesPetroleum Gases, Liquefied Petroleum Gas: IdentificationdigecaNo ratings yet
- R.E.B.T.-overcoming Worry and Fear-Paul A. HauckDocument116 pagesR.E.B.T.-overcoming Worry and Fear-Paul A. Hauckinnersensation100% (8)
- U WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDocument75 pagesU WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDrbee10No ratings yet
- Young InfantDocument69 pagesYoung InfantAurora Doris BatagaNo ratings yet
- Soal Bahasa Inggris Kelas 5Document8 pagesSoal Bahasa Inggris Kelas 5imam hambaliNo ratings yet
- Water Treatment PDFDocument87 pagesWater Treatment PDFJubin KumarNo ratings yet
- Caldorol (Ibuprofen IV)Document14 pagesCaldorol (Ibuprofen IV)Agus SusantoNo ratings yet
- DISC2-14071 AppealLetter PublicCommentsDocument17 pagesDISC2-14071 AppealLetter PublicCommentsJames ParsonsNo ratings yet
- Tile Setting NC II Training RegulationsDocument67 pagesTile Setting NC II Training RegulationsRTC Zamboanga100% (1)