You might also like
- When Glass meets Pharma: Insights about glass as primary packaging materialFrom EverandWhen Glass meets Pharma: Insights about glass as primary packaging materialNo ratings yet
- Inside: Classification of Dental CeramicsDocument10 pagesInside: Classification of Dental CeramicsDaniela AlvisNo ratings yet
- Classification of Dental Ceramics: April 2013Document11 pagesClassification of Dental Ceramics: April 2013Eman Abdalla AhmedNo ratings yet
- 19 Ceramics 2nd YrDocument162 pages19 Ceramics 2nd YrLalit KumarNo ratings yet
- GROUP 3 - Ceramic and GlassesDocument45 pagesGROUP 3 - Ceramic and GlassesKazuha MinatoNo ratings yet
- Metal Free Ceramics in DentistryDocument5 pagesMetal Free Ceramics in DentistryAkanksha MahajanNo ratings yet
- Ceramics: Porcelain-Glass-Structural Clay-Abrasive-Advance CeramicsDocument42 pagesCeramics: Porcelain-Glass-Structural Clay-Abrasive-Advance CeramicsCaryann GumbanNo ratings yet
- Ceramics 2Document42 pagesCeramics 2Caryann GumbanNo ratings yet
- Recent Advances in Ceramics For DentistryDocument10 pagesRecent Advances in Ceramics For DentistryMaqbul AlamNo ratings yet
- Insights On Ceramics As Dental Materials. Part I: Ceramic Material Types in DentistryDocument7 pagesInsights On Ceramics As Dental Materials. Part I: Ceramic Material Types in DentistryKarolina WójcikNo ratings yet
- CeramicsDocument49 pagesCeramicsArun KumarNo ratings yet
- Dental CeramicsDocument162 pagesDental CeramicsDr.Ragini Pandey100% (1)
- Dental Ceramics A Current Review-1Document7 pagesDental Ceramics A Current Review-1Wirajulay Pratiwi SanusiNo ratings yet
- Chemistry For EngineersDocument19 pagesChemistry For EngineersRhomel BonghanoyNo ratings yet
- Dental Ceramics Used in DentistryDocument10 pagesDental Ceramics Used in DentistryERIKA BLANQUETNo ratings yet
- Dental CeramicsDocument62 pagesDental CeramicsAnamika Thakur Rana100% (2)
- Updating Classifications of Ceramic Dental Materials: A Guide To Material SelectionDocument7 pagesUpdating Classifications of Ceramic Dental Materials: A Guide To Material SelectionAngela AcostaNo ratings yet
- Classifications of Dental Ceramics (Autosaved)Document52 pagesClassifications of Dental Ceramics (Autosaved)Muralidharan100% (1)
- Ceramics Portfolio 1Document88 pagesCeramics Portfolio 1Kiann DomingoNo ratings yet
- Ceramic Materials for Aerospace ApplicationsDocument20 pagesCeramic Materials for Aerospace ApplicationsTyasYolanSafitri'BhsNo ratings yet
- Ceramics in Materials ScienceDocument250 pagesCeramics in Materials ScienceNguyễn Thiên AnNo ratings yet
- Materials Classification and Properties IntroductionDocument5 pagesMaterials Classification and Properties Introductionalejandra Rodriguez GodoyNo ratings yet
- Insights On Ceramics As Dental Materials Part I Ce1Document8 pagesInsights On Ceramics As Dental Materials Part I Ce121-104 Michelle Angel LigatsyahNo ratings yet
- CeramicsDocument4 pagesCeramicsAayushi VaidyaNo ratings yet
- Ceramics Report Structure and PropertiesDocument7 pagesCeramics Report Structure and PropertiesSecret TalagaNo ratings yet
- Dental CeramicsDocument434 pagesDental Ceramicskirtiabhi100% (2)
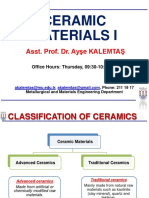
- Ceramic Materials I: Asst - Prof. Dr. Ayşe KALEMTAŞDocument32 pagesCeramic Materials I: Asst - Prof. Dr. Ayşe KALEMTAŞŞebnem Gül İlarslanNo ratings yet
- Ceramics: Automobiles (Sparkplugs and Ceramic Engine Parts Found in Racecars), and Phone Lines. TheyDocument8 pagesCeramics: Automobiles (Sparkplugs and Ceramic Engine Parts Found in Racecars), and Phone Lines. TheyGian BanaresNo ratings yet
- CERAMICSDocument20 pagesCERAMICSChanoxismNo ratings yet
- 4 Dental CeramicDocument153 pages4 Dental CeramicLekshmy ARNo ratings yet
- Dental CeramicsDocument204 pagesDental CeramicsRishabh VermaNo ratings yet
- Dental CeramicsDocument86 pagesDental Ceramicsvadlamudi chakradharNo ratings yet
- Ceramics and Glass Industry: EnvironmentalDocument2 pagesCeramics and Glass Industry: EnvironmentalPatricia de LeonNo ratings yet
- Use of Rhyolite As A Flux in Porcelain SDocument11 pagesUse of Rhyolite As A Flux in Porcelain Smap vitco100% (1)
- Ceramic 2Document173 pagesCeramic 2Dr.Ragini PandeyNo ratings yet
- Ceramics: Materials of Choice for Harsh EnvironmentsDocument54 pagesCeramics: Materials of Choice for Harsh EnvironmentsGeorgina YapNo ratings yet
- CeramicsDocument3 pagesCeramicsFaizah Ayulia NawitaNo ratings yet
- CeramicsDocument28 pagesCeramicswilsonlewinfreud.pulgoNo ratings yet
- Ceramics and Glasses: An Overview of Non-Metallic MaterialsDocument36 pagesCeramics and Glasses: An Overview of Non-Metallic MaterialsShockBlade ZedNo ratings yet
- Comparison of The Marginal Fit of Various Ceramic Crown SystemsDocument5 pagesComparison of The Marginal Fit of Various Ceramic Crown SystemsrojNo ratings yet
- Ceramics DypDocument168 pagesCeramics DypRukhsar VankaniNo ratings yet
- CeramicsDocument18 pagesCeramicsyashwanth h nNo ratings yet
- Ceramics Overview Classification by Microstructure and Processing Methods.Document13 pagesCeramics Overview Classification by Microstructure and Processing Methods.jose100% (1)
- Guided By:-Dr. Jnanadev: Mrs. SavithaDocument121 pagesGuided By:-Dr. Jnanadev: Mrs. SavithaAnuRaveendranNo ratings yet
- PDF-Chaper-5 Ceramic-MaterialsDocument92 pagesPDF-Chaper-5 Ceramic-Materialsaljhun fujitsuNo ratings yet
- ceramicsDocument24 pagesceramicsjahanzeb aliNo ratings yet
- All Ceramic Material SelectionDocument6 pagesAll Ceramic Material SelectionERIKA BLANQUETNo ratings yet
- Ceramics: Properties and TypesDocument25 pagesCeramics: Properties and TypesKawaii SamaNo ratings yet
- Introduction To CeramicsDocument39 pagesIntroduction To CeramicsRasika MalodeNo ratings yet
- Ceramics, PolymersDocument7 pagesCeramics, PolymersArnab Saha100% (1)
- Composition of Ceramic and Its UsesDocument28 pagesComposition of Ceramic and Its UsesManveer SinghNo ratings yet
- 2.dental CeramicsDocument320 pages2.dental CeramicsNamitha AP100% (1)
- CERAMICSDocument41 pagesCERAMICSramandeep singhNo ratings yet
- Ceramics - Shadow of Enamel An OverviewDocument14 pagesCeramics - Shadow of Enamel An OverviewSalma MahmoudNo ratings yet
- BDJ 22 - Do you know your ceremics 2Document4 pagesBDJ 22 - Do you know your ceremics 2Mathias SchottNo ratings yet
- Lecture 08Document36 pagesLecture 08winnieNo ratings yet
- Guide To All-Ceramic BondingDocument12 pagesGuide To All-Ceramic BondingDan CosteaNo ratings yet
- UNIT V - Ceramics-Composites-Nano MaterialsDocument59 pagesUNIT V - Ceramics-Composites-Nano MaterialsHarsha MallaNo ratings yet
- Discover the History and Uses of Ceramic MaterialsDocument7 pagesDiscover the History and Uses of Ceramic Materialsletter_ashish4444No ratings yet
- PCI Standard Design Practice Manual - 2014Document32 pagesPCI Standard Design Practice Manual - 2014rahuljoagNo ratings yet
- Tenax 88s HR (E 50 6 Mn1ni B 32 h5)Document1 pageTenax 88s HR (E 50 6 Mn1ni B 32 h5)brunizzaNo ratings yet
- MOC - Ullmann'sDocument48 pagesMOC - Ullmann'sacer_asdNo ratings yet
- Distorsion Prevented by DesignDocument3 pagesDistorsion Prevented by DesignMathew RodriguezNo ratings yet
- E-Store PricelistDocument43 pagesE-Store PricelistDibya Ranjan Dash100% (1)
- DacnisDocument1 pageDacnisironiteNo ratings yet
- Stability-and-precision-of-immobilization-in-Radiation-Oncology-using-Nanotechnology and Thesis Ecological DevelopmentDocument8 pagesStability-and-precision-of-immobilization-in-Radiation-Oncology-using-Nanotechnology and Thesis Ecological DevelopmentSelvabala904260No ratings yet
- AOC FR Resin K320-A - Technical DataDocument3 pagesAOC FR Resin K320-A - Technical Dataomarjaime01No ratings yet
- Anti Skid Mechanical Grooves On Concrete PavementDocument13 pagesAnti Skid Mechanical Grooves On Concrete PavementRainakNo ratings yet
- Havells Cables Pricelist 01.05.2018 PDFDocument5 pagesHavells Cables Pricelist 01.05.2018 PDFjuga2013No ratings yet
- Adequacy of Materials For Civil WorksDocument25 pagesAdequacy of Materials For Civil Workshari vNo ratings yet
- Study of The Potentiality To Manufacture Forming Tools Via Waam (Wire + Arc Additive Manufacturing)Document10 pagesStudy of The Potentiality To Manufacture Forming Tools Via Waam (Wire + Arc Additive Manufacturing)jefferson segundoNo ratings yet
- Chemical Equivalent ListDocument2 pagesChemical Equivalent ListRifat Azad100% (1)
- Conclusion M60 PDFDocument39 pagesConclusion M60 PDFAnurag PilaniaNo ratings yet
- Silica Plastic BlockDocument5 pagesSilica Plastic Blockdharshini deivasigamaniNo ratings yet
- Vetoflex SS783: High Quality Elastic One Component Moisture Cure Silicone SealantDocument2 pagesVetoflex SS783: High Quality Elastic One Component Moisture Cure Silicone SealantSHAIK ASIMUDDINNo ratings yet
- CC-Flat and Elongated ASTM D4791Document1 pageCC-Flat and Elongated ASTM D4791VasaNo ratings yet
- Ethylene Glycol MonostearateDocument4 pagesEthylene Glycol MonostearateVaibhav NikharNo ratings yet
- A11 High Performance Butterfly Valve BulletinDocument28 pagesA11 High Performance Butterfly Valve BulletinRizalfariz HasbiNo ratings yet
- IFC EHS GuidelinesDocument31 pagesIFC EHS GuidelinesSamiNo ratings yet
- BS 31 Steel Conduit and Fittings For Electrical Wiring PDFDocument36 pagesBS 31 Steel Conduit and Fittings For Electrical Wiring PDFEddy Volao100% (3)
- PROTECTIVE COATING FOR CONCRETE & STEELDocument2 pagesPROTECTIVE COATING FOR CONCRETE & STEELkhrisna.dipa.utamaNo ratings yet
- Ma'Aden Engineering Manual: Piping MaterialsDocument21 pagesMa'Aden Engineering Manual: Piping Materialssameer ejaazNo ratings yet
- Idoc - Pub Bs en 13369 TolerancesDocument6 pagesIdoc - Pub Bs en 13369 TolerancesRai Singh MalhiNo ratings yet
- Sight GlassDocument2 pagesSight GlassLorenzoNo ratings yet
- Nanogen Product Lists Includes Starch, Talc, Mica and MoreDocument3 pagesNanogen Product Lists Includes Starch, Talc, Mica and MoreRobertusNo ratings yet
- Pervious ConcreteDocument4 pagesPervious ConcretesuwashNo ratings yet
- 5-1-4.DRAW LATCH enDocument2 pages5-1-4.DRAW LATCH enThan Zaw OoNo ratings yet
- Fastener Academy Basics PDFDocument94 pagesFastener Academy Basics PDFKiran BathiniNo ratings yet
- Montage Brochure PDFDocument8 pagesMontage Brochure PDFCharlie SouzaNo ratings yet
- Beginning AutoCAD® 2020 Exercise WorkbookFrom EverandBeginning AutoCAD® 2020 Exercise WorkbookRating: 2.5 out of 5 stars2.5/5 (3)
- FreeCAD | Step by Step: Learn how to easily create 3D objects, assemblies, and technical drawingsFrom EverandFreeCAD | Step by Step: Learn how to easily create 3D objects, assemblies, and technical drawingsRating: 5 out of 5 stars5/5 (1)
- Certified Solidworks Professional Advanced Weldments Exam PreparationFrom EverandCertified Solidworks Professional Advanced Weldments Exam PreparationRating: 5 out of 5 stars5/5 (1)
- CATIA V5-6R2015 Basics - Part I : Getting Started and Sketcher WorkbenchFrom EverandCATIA V5-6R2015 Basics - Part I : Getting Started and Sketcher WorkbenchRating: 4 out of 5 stars4/5 (10)
- SketchUp Success for Woodworkers: Four Simple Rules to Create 3D Drawings Quickly and AccuratelyFrom EverandSketchUp Success for Woodworkers: Four Simple Rules to Create 3D Drawings Quickly and AccuratelyRating: 1.5 out of 5 stars1.5/5 (2)
- Design Research Through Practice: From the Lab, Field, and ShowroomFrom EverandDesign Research Through Practice: From the Lab, Field, and ShowroomRating: 3 out of 5 stars3/5 (7)
- From Vision to Version - Step by step guide for crafting and aligning your product vision, strategy and roadmap: Strategy Framework for Digital Product Management RockstarsFrom EverandFrom Vision to Version - Step by step guide for crafting and aligning your product vision, strategy and roadmap: Strategy Framework for Digital Product Management RockstarsNo ratings yet
- Fusion 360 | Step by Step: CAD Design, FEM Simulation & CAM for Beginners.From EverandFusion 360 | Step by Step: CAD Design, FEM Simulation & CAM for Beginners.No ratings yet
- FreeCAD | Design Projects: Design advanced CAD models step by stepFrom EverandFreeCAD | Design Projects: Design advanced CAD models step by stepRating: 5 out of 5 stars5/5 (1)
- Certified Solidworks Professional Advanced Surface Modeling Exam PreparationFrom EverandCertified Solidworks Professional Advanced Surface Modeling Exam PreparationRating: 5 out of 5 stars5/5 (1)
- Autodesk Fusion 360: A Power Guide for Beginners and Intermediate Users (3rd Edition)From EverandAutodesk Fusion 360: A Power Guide for Beginners and Intermediate Users (3rd Edition)Rating: 5 out of 5 stars5/5 (2)
- Contactless Vital Signs MonitoringFrom EverandContactless Vital Signs MonitoringWenjin WangNo ratings yet