You might also like
- NCLEX Medical Terminology ReviewDocument15 pagesNCLEX Medical Terminology Reviewapollo100% (3)
- Nursing InductionDocument114 pagesNursing InductionMichael Long92% (26)
- ECG2350 EnglishSM 08SK2.006.00045BDocument102 pagesECG2350 EnglishSM 08SK2.006.00045BЮрій КобцевNo ratings yet
- 3f Medical - Iris Pms8210a - Service ManualDocument42 pages3f Medical - Iris Pms8210a - Service ManualNuno Freitas Bastos100% (1)
- BSM6000 UG Part I-HDocument0 pagesBSM6000 UG Part I-HMiguel Ángel Escobar FloresNo ratings yet
- 23 Cardiac PDFDocument5 pages23 Cardiac PDFIJAERS JOURNALNo ratings yet
- Myarticle 2Document6 pagesMyarticle 2mypinklagoon8411No ratings yet
- Modern Concepts Concerning The Origin Physiol.00054.2012Document19 pagesModern Concepts Concerning The Origin Physiol.00054.2012Pedro RodriguezNo ratings yet
- 4 - Sinoatrialnode ArchitectureDocument7 pages4 - Sinoatrialnode ArchitectureSergio BenavidesNo ratings yet
- 247 FullDocument6 pages247 FullBryan FarrelNo ratings yet
- Geko and OtherDocument7 pagesGeko and OtherParul ThakurNo ratings yet
- Intravascular Low-Power Laser Illumination Through Special Fiber DiffusersDocument3 pagesIntravascular Low-Power Laser Illumination Through Special Fiber DiffusersNoura RoseNo ratings yet
- Cardiac PacemakersDocument206 pagesCardiac PacemakersMiguel PenarandaNo ratings yet
- Cardiac Ion ChannelsDocument10 pagesCardiac Ion ChannelsPedro RodriguezNo ratings yet
- Fundamentals of ECG InterpretationDocument12 pagesFundamentals of ECG InterpretationPankaj Patil100% (1)
- Nihms 992969Document26 pagesNihms 992969aliusman laseNo ratings yet
- Arritmia SVDocument17 pagesArritmia SVCésar Lobo TarangoNo ratings yet
- Application 2Document13 pagesApplication 2Samiul Basir ShuvoNo ratings yet
- 38.17 Cardiac Pacing: Basic Concepts: Renato Pietro RicciDocument16 pages38.17 Cardiac Pacing: Basic Concepts: Renato Pietro RicciurtikikeNo ratings yet
- Marchant2022 CardiacPacemakerAPDocument7 pagesMarchant2022 CardiacPacemakerAPsabrinasameja75No ratings yet
- Logy Assighnment On Automaticity Rhythmicity AutorecoveredDocument10 pagesLogy Assighnment On Automaticity Rhythmicity AutorecoveredM Asif RiazNo ratings yet
- The Evolution of PacemakersDocument11 pagesThe Evolution of PacemakersAman PotdarNo ratings yet
- Balloon Assisted Technique in Peripheral Interventions A Useful ToolDocument4 pagesBalloon Assisted Technique in Peripheral Interventions A Useful ToolHerald Scholarly Open AccessNo ratings yet
- Diagnostic Challenges in Musculoskeletal Radiology PDFDocument182 pagesDiagnostic Challenges in Musculoskeletal Radiology PDFphuong mai leNo ratings yet
- Adjunctive Therapies For Ventricular Arrhythmia ManagementDocument10 pagesAdjunctive Therapies For Ventricular Arrhythmia ManagementsaikrishnaNo ratings yet
- Type of PacemakerDocument26 pagesType of PacemakerMohammad AlmuhaiminNo ratings yet
- Taquicardias Ventriculares Qhion Cheng y Andrea Natale 2020Document16 pagesTaquicardias Ventriculares Qhion Cheng y Andrea Natale 2020Vallejo Romo Alberto CristianNo ratings yet
- Multi-Case Review of Various Applications of Vascular Plugs in Embolization of High Flow Vascular LesionsDocument8 pagesMulti-Case Review of Various Applications of Vascular Plugs in Embolization of High Flow Vascular LesionsBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- Adverse Diastolic Remodeling After Reperfused ST-elevation Myocardial Infarction: An Important Prognostic IndicatorDocument11 pagesAdverse Diastolic Remodeling After Reperfused ST-elevation Myocardial Infarction: An Important Prognostic IndicatorCatia MoraesNo ratings yet
- Nattel&Carlsson2006 Antiarrhythmic Drugs TaseDocument16 pagesNattel&Carlsson2006 Antiarrhythmic Drugs TaseGiulia AndreeaNo ratings yet
- Design of An ECG Sensor Circuitry For Cardiovascular Disease DiagnosisDocument6 pagesDesign of An ECG Sensor Circuitry For Cardiovascular Disease DiagnosisLaalai LaalaiNo ratings yet
- Manejo Perioperatorio de MarcapasosDocument6 pagesManejo Perioperatorio de MarcapasosPao Sofía MoralesNo ratings yet
- Cardiac Pacemakers A Basic ReviewDocument11 pagesCardiac Pacemakers A Basic ReviewMuhammad Dilawar khanNo ratings yet
- Mastering Temporary Invasive Cardiac Pacing: ClinicalDocument8 pagesMastering Temporary Invasive Cardiac Pacing: ClinicaldenokNo ratings yet
- Jha Sheth 2023 2023 Neurocritical Care Updates in Cerebrovascular DiseaseDocument5 pagesJha Sheth 2023 2023 Neurocritical Care Updates in Cerebrovascular DiseaseProdi Bedah SarafNo ratings yet
- Gene Therapy For Cardiac ArrhythmiasDocument9 pagesGene Therapy For Cardiac ArrhythmiasIdada EzekielNo ratings yet
- Interpreting AV (Heart) Blocks: Breaking Down The Mystery: 2 Contact HoursDocument29 pagesInterpreting AV (Heart) Blocks: Breaking Down The Mystery: 2 Contact HoursAsri RachmawatiNo ratings yet
- 1 s2.0 S0735109720344909 MainDocument13 pages1 s2.0 S0735109720344909 MainIndira Ulfa DunandNo ratings yet
- Motor Stimulation With Interferential Cu 1985 Australian Journal of PhysiothDocument6 pagesMotor Stimulation With Interferential Cu 1985 Australian Journal of PhysiothEmad Tawfik AhmadNo ratings yet
- Heart Valve Function: A Biomechanical Perspective: ReferencesDocument24 pagesHeart Valve Function: A Biomechanical Perspective: ReferencesShivaji DoraNo ratings yet
- Restoring Heart Function and Electrical IntegrityDocument13 pagesRestoring Heart Function and Electrical IntegrityRaul OrtegaNo ratings yet
- Arrhythmogenic Ion-Channel Remodeling in The Heart: Heart Failure, Myocardial Infarction, and Atrial FibrillationDocument34 pagesArrhythmogenic Ion-Channel Remodeling in The Heart: Heart Failure, Myocardial Infarction, and Atrial FibrillationPio ArayaNo ratings yet
- 2021 Article 2376Document6 pages2021 Article 2376Anna Sofía ParedesNo ratings yet
- Heart Rate Detection From Plantar Bioimpedance Measurements: R. González Landaeta, O. Casas, R. Pallàs-ArenyDocument4 pagesHeart Rate Detection From Plantar Bioimpedance Measurements: R. González Landaeta, O. Casas, R. Pallàs-ArenyLowayNo ratings yet
- Management of Acute Ischemic Stroke Due To Large-Vessel OcclusionDocument12 pagesManagement of Acute Ischemic Stroke Due To Large-Vessel OcclusionYaiza VillalobosNo ratings yet
- Cardiovascular (Reviewer)Document19 pagesCardiovascular (Reviewer)cataleya mesaNo ratings yet
- Clinical Neurophysiology: Derek M. Miller, James F. Baker, W. Zev RymerDocument9 pagesClinical Neurophysiology: Derek M. Miller, James F. Baker, W. Zev RymerMiguelNo ratings yet
- Bio Impedance Monitoring For Physicians 1Document35 pagesBio Impedance Monitoring For Physicians 1ChiquinquiraNo ratings yet
- 10 1161@circep 118 007142Document13 pages10 1161@circep 118 007142cardionerd101No ratings yet
- Cervical Arterial Dysfunction Assessment and Manual Therapy: Roger Kerry, Alan J. TaylorDocument11 pagesCervical Arterial Dysfunction Assessment and Manual Therapy: Roger Kerry, Alan J. Taylornídia_santos_3No ratings yet
- Tissue To Organisms/Physiology & PharmacologyDocument6 pagesTissue To Organisms/Physiology & PharmacologyStudent LifeNo ratings yet
- PurkinjeDocument11 pagesPurkinjemaciejNo ratings yet
- Detection and Classification of Cardiac Arrhythmias by A Challenge-Best Deep Learning Neural Network ModelDocument27 pagesDetection and Classification of Cardiac Arrhythmias by A Challenge-Best Deep Learning Neural Network ModelMhd rdbNo ratings yet
- Joung2007-BM Mononuclear Cells - MIDocument11 pagesJoung2007-BM Mononuclear Cells - MIiulia andreeaNo ratings yet
- Vejdani Jahromi2015Document10 pagesVejdani Jahromi2015Daniel Stefano Vásquez RojasNo ratings yet
- EJMSOL14Document10 pagesEJMSOL14Sara TeixeiraNo ratings yet
- AANA Journal Course: Update For Nurse AnesthetistsDocument7 pagesAANA Journal Course: Update For Nurse AnesthetistsDayuKurnia DewantiNo ratings yet
- Brain Death Provokes Acute Alteration in Myocardial Morphology Transplant Int 2011Document7 pagesBrain Death Provokes Acute Alteration in Myocardial Morphology Transplant Int 2011Marisol Gallego DuqueNo ratings yet
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXFrom EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXRating: 5 out of 5 stars5/5 (2)
- Endocardial Infarct Scar Recognition by MyocardialDocument8 pagesEndocardial Infarct Scar Recognition by MyocardialMihai-Marian RuseiNo ratings yet
- Application of Nuclear Magnetic Resonance ImagingDocument19 pagesApplication of Nuclear Magnetic Resonance ImagingHoracio Dorantes ReyesNo ratings yet
- Interpretation of The Electrocardiogram - Part IV - The ST Segment, T and U Waves, and The QT IntervalDocument10 pagesInterpretation of The Electrocardiogram - Part IV - The ST Segment, T and U Waves, and The QT Intervallu truongNo ratings yet
- Noninvasive Imaging of Congenital Heart Disease Before and After Surgical ReconstructionFrom EverandNoninvasive Imaging of Congenital Heart Disease Before and After Surgical ReconstructionNo ratings yet
- Cardiac Electrophysiology Without FluoroscopyFrom EverandCardiac Electrophysiology Without FluoroscopyRiccardo ProiettiNo ratings yet
- Vesta 121iDocument4 pagesVesta 121iAnil JainNo ratings yet
- User Manual: Shenzhen Biocare Bio-Medical Equipment Co., LTDDocument182 pagesUser Manual: Shenzhen Biocare Bio-Medical Equipment Co., LTDArnaldo AbadNo ratings yet
- Hypokalemia and Anesthetic Implications: Wong, Patrick Schafer, and John R. SchultzDocument23 pagesHypokalemia and Anesthetic Implications: Wong, Patrick Schafer, and John R. SchultzRidski D. MiruNo ratings yet
- Datascope 98XT BrochureDocument2 pagesDatascope 98XT BrochureFelipe ValenciaNo ratings yet
- 2 - Holter ECG - TLC5000 Dynamic ECG SystemDocument3 pages2 - Holter ECG - TLC5000 Dynamic ECG SystemChristian Donfack fogang100% (1)
- PB2 NP3Document8 pagesPB2 NP3Herne BalberdeNo ratings yet
- S8 Specifications V2.0 20221208Document8 pagesS8 Specifications V2.0 20221208Declan WangNo ratings yet
- Final - Exam - 6512N - EXAM 1Document13 pagesFinal - Exam - 6512N - EXAM 1erick kanyi100% (1)
- Nursing Responsibilities After CCDocument5 pagesNursing Responsibilities After CCSofia P. PanlilioNo ratings yet
- Chyu Shah 2022 Electrocardiograms in Critical Care CardiologyDocument5 pagesChyu Shah 2022 Electrocardiograms in Critical Care Cardiologytegar ksatriaNo ratings yet
- SaikatDocument50 pagesSaikatSaurabh MondalNo ratings yet
- Biosignals For EveryoneDocument8 pagesBiosignals For EveryoneDiMayerNo ratings yet
- FX 3000MD enDocument2 pagesFX 3000MD enhieu tongNo ratings yet
- An Approach To Ekgs: By: Siraj Mithoowani & Richa Parashar 2012 Medical Education Interest GroupDocument34 pagesAn Approach To Ekgs: By: Siraj Mithoowani & Richa Parashar 2012 Medical Education Interest GroupAli MullaNo ratings yet
- Acute Cardiac EKG Interpretation - Basics Part 1 - ScriptDocument2 pagesAcute Cardiac EKG Interpretation - Basics Part 1 - ScriptDarby GravinoNo ratings yet
- Ecg Findings in Pulmonary Embolism: Acute Cor PulmonaleDocument1 pageEcg Findings in Pulmonary Embolism: Acute Cor PulmonaleSuci Dika UtariNo ratings yet
- BeneHeart D3 Operators ManualDocument208 pagesBeneHeart D3 Operators Manualelectromedicina.esNo ratings yet
- Nursing Induction PPT 2Document114 pagesNursing Induction PPT 2Mukesh Choudhary Jat100% (3)
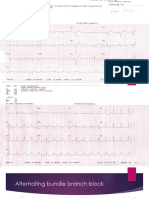
- Alternating Bundle Branch BlockDocument9 pagesAlternating Bundle Branch BlockSyifa Mahmud Syukran AkbarNo ratings yet
- Mit Thesis FormatDocument7 pagesMit Thesis Formatafloblnpeewxby100% (2)
- Cardioline AR1200Document56 pagesCardioline AR1200MauricioGS100% (1)
- A Brief Review History To Understand Fundamentals of ElectrocardiographyDocument6 pagesA Brief Review History To Understand Fundamentals of ElectrocardiographyAbdullah AbdurrehmanNo ratings yet
- ADAS1000Document80 pagesADAS1000Serhii SerikovNo ratings yet
- The CardiacDocument7 pagesThe CardiacCake ManNo ratings yet
- Syaqiq 094-Lpk EkgDocument6 pagesSyaqiq 094-Lpk EkgEko HarmokoNo ratings yet