You might also like
- Pre-Employment Medical FormsDocument8 pagesPre-Employment Medical Formsnot your medz duranNo ratings yet
- UHS Pre-Enrolment Physical Examination Report Form (FILLABLE)Document2 pagesUHS Pre-Enrolment Physical Examination Report Form (FILLABLE)Guillermo PantuhanNo ratings yet
- Med FormDocument3 pagesMed FormWsu CampusHousingNo ratings yet
- Student Health RecordsDocument2 pagesStudent Health Recordsailen joy villoNo ratings yet
- Newborn Screening Continuity Clinic Initial Consult Form Ncr/MimaropaDocument3 pagesNewborn Screening Continuity Clinic Initial Consult Form Ncr/Mimaropajacqueline licupNo ratings yet
- DAAD - Health CertificateDocument2 pagesDAAD - Health Certificaterosenrot1100% (2)
- Family Health Assessment Form: University of San Jose-Recoletos School of Allied Medical Sciences NursingDocument4 pagesFamily Health Assessment Form: University of San Jose-Recoletos School of Allied Medical Sciences NursingIvan A. EleginoNo ratings yet
- UHS Employee Health Info FormDocument7 pagesUHS Employee Health Info FormCrystal AnnNo ratings yet
- Referral FormDocument4 pagesReferral FormLchg KrvyNo ratings yet
- ZIKA ICIFDocument2 pagesZIKA ICIFMarav SymbNo ratings yet
- MedicalDocument2 pagesMedicalChris HutchinsonNo ratings yet
- Medical Certificate of FitnessDocument2 pagesMedical Certificate of FitnessDINESH CHANDRA GANNAVARAPUNo ratings yet
- Graduate Health Exam ReportDocument2 pagesGraduate Health Exam ReportTrieu LeNo ratings yet
- Manila, Philippines: I. Patient InformationDocument1 pageManila, Philippines: I. Patient InformationJoa QuinNo ratings yet
- Delhi Public School, Mathura Road, New Delhi-110003: Health History (Part-I)Document2 pagesDelhi Public School, Mathura Road, New Delhi-110003: Health History (Part-I)shoaibali09usNo ratings yet
- Welcome To Orthopedics Care Center !Document2 pagesWelcome To Orthopedics Care Center !Ahmed M. RafatNo ratings yet
- Manila, Philippines: I. Patient InformationDocument1 pageManila, Philippines: I. Patient InformationJoa QuinNo ratings yet
- UHS Pre-Enrolment Physical (Medical) Examination Form PDFDocument2 pagesUHS Pre-Enrolment Physical (Medical) Examination Form PDFReaStephanieCidNo ratings yet
- Medical Certificate of Fitness: To Be Filled by CandidateDocument2 pagesMedical Certificate of Fitness: To Be Filled by CandidatevenkatNo ratings yet
- Chinese General Hospital and Medical Center Institute of Pathology Covid-19 PCR Laboratory Test Request FormDocument1 pageChinese General Hospital and Medical Center Institute of Pathology Covid-19 PCR Laboratory Test Request FormJolaine ValloNo ratings yet
- Medical Information Record FormDocument2 pagesMedical Information Record FormCharlie SumagaysayNo ratings yet
- Medical Examination 5Document1 pageMedical Examination 5Melanie AgustinNo ratings yet
- Midsayap Doctors Specialist Hospital, Inc.: Clinical Cover SheetDocument2 pagesMidsayap Doctors Specialist Hospital, Inc.: Clinical Cover SheetRemej SilutgamNo ratings yet
- Nfhs Student Health RecordDocument2 pagesNfhs Student Health Recordestudillojesusimo64No ratings yet
- D ReportDocument2 pagesD ReportHihiNo ratings yet
- Medical and Dental Form Students 2022Document2 pagesMedical and Dental Form Students 2022MAC3No ratings yet
- Laboratory Referral Request Form For Covid-19: San Lazaro HospitalDocument1 pageLaboratory Referral Request Form For Covid-19: San Lazaro HospitalRalph Emmanuel MercadoNo ratings yet
- PAUNAWA: Mahigpit Na Ipinapatupad NG Kagawaran NG Edukasyon-Probinsya NG Cavite Ang "NO FACE MASK, NO ENTRY" BilangDocument1 pagePAUNAWA: Mahigpit Na Ipinapatupad NG Kagawaran NG Edukasyon-Probinsya NG Cavite Ang "NO FACE MASK, NO ENTRY" BilangMarvel Felicity Rosell ArmestoNo ratings yet
- Annual Medical ReportDocument6 pagesAnnual Medical ReportMark BuendiaNo ratings yet
- Health Declaration Form: Depedcavite - Medical@deped - Gov.phDocument2 pagesHealth Declaration Form: Depedcavite - Medical@deped - Gov.phAnne Esguerra100% (1)
- 2.physical E, HISTORY NCPDocument13 pages2.physical E, HISTORY NCPمريم حجيNo ratings yet
- Hao Medical Clnic Family Medicine: Buhangin, Davao CityDocument2 pagesHao Medical Clnic Family Medicine: Buhangin, Davao CityJulie Ann LacandulaNo ratings yet
- Bản sao của Form thực hành nhập môn KXNK 2Document2 pagesBản sao của Form thực hành nhập môn KXNK 2YouTube GoogleNo ratings yet
- Barasan, Michelle - UHS Patient RecordDocument12 pagesBarasan, Michelle - UHS Patient RecordMichelle barasanNo ratings yet
- Group Death - Attending Physician's StatementDocument2 pagesGroup Death - Attending Physician's StatementJohn Victor Perez OretoNo ratings yet
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Document6 pagesAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "Chum ChitaruNo ratings yet
- -HEALTH-DECLARATIONDocument2 pages-HEALTH-DECLARATIONrosabelromero09No ratings yet
- Saint Louis University School of Medicine Department of Medicine General Data: Past Medical HistoryDocument3 pagesSaint Louis University School of Medicine Department of Medicine General Data: Past Medical HistoryMarieCrisNo ratings yet
- Kolej Teknologi Darulnaim: Darulnaim College of TechnologyDocument5 pagesKolej Teknologi Darulnaim: Darulnaim College of TechnologyDaryanto SutejiNo ratings yet
- Dec 2020 AEFI reporting formDocument1 pageDec 2020 AEFI reporting formHeRha DAniarNo ratings yet
- Medical Fitness Form PDFDocument4 pagesMedical Fitness Form PDFKartikeya BagraNo ratings yet
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Document21 pagesAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "allen zacariasNo ratings yet
- Chinese General Hospital and Medical Center Institute of Pathology Covid-19 PCR Laboratory Test Request FormDocument1 pageChinese General Hospital and Medical Center Institute of Pathology Covid-19 PCR Laboratory Test Request Formrebecca orenaNo ratings yet
- medicaltests_formNDocument1 pagemedicaltests_formNJasanta JinorNo ratings yet
- 2017 Certificate of Health 1Document2 pages2017 Certificate of Health 1herman syahNo ratings yet
- Soccer Player Medical History Form TemplateDocument1 pageSoccer Player Medical History Form Templatejosephkwasikumah16No ratings yet
- HSU Pre-Enrollment Medical Record Form (FRESHMAN)Document4 pagesHSU Pre-Enrollment Medical Record Form (FRESHMAN)ChristnerNo ratings yet
- Comprehensive H&PDocument2 pagesComprehensive H&PjwwisnerNo ratings yet
- Medical History FormDocument2 pagesMedical History FormTameisha ThomasNo ratings yet
- Prenatal Check Up InterviewDocument7 pagesPrenatal Check Up InterviewSHIELOU LOMODNo ratings yet
- San Beda College of Medicine Batch 2017 Neuro-Pedia ChecklistDocument9 pagesSan Beda College of Medicine Batch 2017 Neuro-Pedia ChecklistAngelaTrinidadNo ratings yet
- Medical ReportDocument1 pageMedical Reportwhit.ehouseboyquantiumNo ratings yet
- Form G Health Examination Report International StudentDocument6 pagesForm G Health Examination Report International StudentVictor OjukwuNo ratings yet
- Health Insurance Pre-Authorisation FormDocument3 pagesHealth Insurance Pre-Authorisation FormTofan kumar MohapatraNo ratings yet
- Student Health Services - 305 Estill Street Berea, KY 40403 - Phone: (859) 985-1415Document4 pagesStudent Health Services - 305 Estill Street Berea, KY 40403 - Phone: (859) 985-1415JohnNo ratings yet
- ISO 05 Student Health Record 1 RevDocument2 pagesISO 05 Student Health Record 1 RevHahaha HihihooNo ratings yet
- Health Screening and Assessment Form - SampleDocument3 pagesHealth Screening and Assessment Form - SampleRhu1 San Ildefonso100% (1)
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- Preclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1From EverandPreclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1No ratings yet
- Final OutputDocument33 pagesFinal OutputNiko ChavezNo ratings yet
- AsiaPacific Obs ReportDocument4 pagesAsiaPacific Obs ReportNiko ChavezNo ratings yet
- Final - Mechanics For The Logo Design Contest For The Philippine Bamboo MonthDocument3 pagesFinal - Mechanics For The Logo Design Contest For The Philippine Bamboo MonthNiko ChavezNo ratings yet
- The Port of TaclobanDocument1 pageThe Port of TaclobanNiko ChavezNo ratings yet
- Port of Tacloban Proposed DesignDocument7 pagesPort of Tacloban Proposed DesignNiko ChavezNo ratings yet
- Ojt JournalDocument51 pagesOjt JournalNiko ChavezNo ratings yet
- Chapter 15Document69 pagesChapter 15Niko ChavezNo ratings yet
- 2023 UPDATED 2016 Revised IRR of RA No. 9184 As of 11 January 2023Document391 pages2023 UPDATED 2016 Revised IRR of RA No. 9184 As of 11 January 2023Agnes FranciscoNo ratings yet
- Lecture 1 - CONSTRUCTION PROJECT MANAGEMENTDocument17 pagesLecture 1 - CONSTRUCTION PROJECT MANAGEMENTNiko ChavezNo ratings yet
- EVSU R&D Research Proposal TemplateDocument3 pagesEVSU R&D Research Proposal TemplateNiko ChavezNo ratings yet
- Lecture 2a - Contracts and SpecificationDocument35 pagesLecture 2a - Contracts and SpecificationNiko ChavezNo ratings yet
- CE 412 CE Project I Course SyllabusDocument5 pagesCE 412 CE Project I Course SyllabusNiko ChavezNo ratings yet
- Book I General Provision 24 January 2019Document77 pagesBook I General Provision 24 January 2019Niko ChavezNo ratings yet
- Insect Muscles Innervated by Single Motoneurons: Structural and Biochemical FeaturesDocument10 pagesInsect Muscles Innervated by Single Motoneurons: Structural and Biochemical FeaturesNiko ChavezNo ratings yet
- Scores and Answer KeyDocument5 pagesScores and Answer KeyNiko ChavezNo ratings yet
- ACTIVITY 3 - Preparation of Undisturbed Soil Sample For TestingDocument5 pagesACTIVITY 3 - Preparation of Undisturbed Soil Sample For TestingNiko ChavezNo ratings yet
- Comprehensive Exam With Answer KeyDocument7 pagesComprehensive Exam With Answer KeyNiko ChavezNo ratings yet
- Reading and Writing Skills 11 Learning Activity Sheet 4 and 5 Quarter 3 Week 4-6Document3 pagesReading and Writing Skills 11 Learning Activity Sheet 4 and 5 Quarter 3 Week 4-6Niko ChavezNo ratings yet
- Breaking Down Barriers To Fitness: Here Are Some of The More Common Barriers and Solutions For Overcoming ThemDocument1 pageBreaking Down Barriers To Fitness: Here Are Some of The More Common Barriers and Solutions For Overcoming ThemNiko ChavezNo ratings yet
- Angle of DepressionDocument9 pagesAngle of DepressionNiko ChavezNo ratings yet
- Personal Development Jade Lynn H. Bersoza 11-MangoDocument19 pagesPersonal Development Jade Lynn H. Bersoza 11-MangoNiko ChavezNo ratings yet
- SteelDocument9 pagesSteelNiko ChavezNo ratings yet
- M MergedDocument7 pagesM MergedNiko ChavezNo ratings yet
- Ilovepdf Merged 3 2Document1 pageIlovepdf Merged 3 2Niko ChavezNo ratings yet
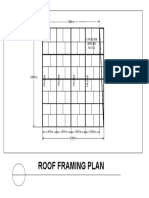
- Roof Framing PlanDocument1 pageRoof Framing PlanNiko ChavezNo ratings yet
- READING AND WRITING SKILLS 11Document2 pagesREADING AND WRITING SKILLS 11Niko ChavezNo ratings yet
- Second Floor Plan: Children Bedroom Children BedroomDocument1 pageSecond Floor Plan: Children Bedroom Children BedroomNiko ChavezNo ratings yet
- The 3D ModelDocument2 pagesThe 3D ModelNiko ChavezNo ratings yet
- Activity 2Document1 pageActivity 2Niko ChavezNo ratings yet
- Quiz Chapter 1 Business Combinations Part 1Document6 pagesQuiz Chapter 1 Business Combinations Part 1Kaye L. Dela CruzNo ratings yet
- HE HOUSEKEEPING GR11 Q1 MODULE-6-for-teacherDocument25 pagesHE HOUSEKEEPING GR11 Q1 MODULE-6-for-teacherMikaela YtacNo ratings yet
- 1967 2013 PDFDocument70 pages1967 2013 PDFAlberto Dorado Martín100% (1)
- The Three Pillars of The ASEANDocument13 pagesThe Three Pillars of The ASEANLouwell Abejo RiñoNo ratings yet
- Hele 4 PPT - 2nd QT - Week 1Document47 pagesHele 4 PPT - 2nd QT - Week 1jerico juarezNo ratings yet
- Cambridge English Business Vantage Sample Paper 1 Listening v2Document5 pagesCambridge English Business Vantage Sample Paper 1 Listening v2salma23478No ratings yet
- 5e3 Like ApproachDocument1 page5e3 Like Approachdisse_detiNo ratings yet
- 00001Document20 pages00001Maggie ZhuNo ratings yet
- CFPA E Guideline No 2 2013 FDocument39 pagesCFPA E Guideline No 2 2013 Fmexo62No ratings yet
- Fixture Design ProjectDocument4 pagesFixture Design ProjectJosh CastleNo ratings yet
- MPU 2232 Chapter 5-Marketing PlanDocument27 pagesMPU 2232 Chapter 5-Marketing Plandina azmanNo ratings yet
- The Essential Guide To Data in The Cloud:: A Handbook For DbasDocument20 pagesThe Essential Guide To Data in The Cloud:: A Handbook For DbasInes PlantakNo ratings yet
- Tem 2final PDFDocument9 pagesTem 2final PDFSkuukzky baeNo ratings yet
- Product Catalog Encoders en IM0038143Document788 pagesProduct Catalog Encoders en IM0038143Eric GarciaNo ratings yet
- Examen TSMDocument4 pagesExamen TSMKaryna VeraNo ratings yet
- Vertical Transportation SystemDocument15 pagesVertical Transportation SystemAnupama MorankarNo ratings yet
- Toyota's Marketing StrategyDocument14 pagesToyota's Marketing StrategyLavin Gurnani0% (1)
- Chapter 2 Research and DesignDocument24 pagesChapter 2 Research and Designalvin salesNo ratings yet
- The Mini-Guide To Sacred Codes and SwitchwordsDocument99 pagesThe Mini-Guide To Sacred Codes and SwitchwordsJason Alex100% (9)
- Chapter Three 3.0 Research MethodologyDocument5 pagesChapter Three 3.0 Research MethodologyBoyi EnebinelsonNo ratings yet
- Operational Readiness Guide - 2017Document36 pagesOperational Readiness Guide - 2017albertocm18100% (2)
- Online Student Enrollment SystemDocument29 pagesOnline Student Enrollment SystemajidonsonNo ratings yet
- Rick CobbyDocument4 pagesRick CobbyrickcobbyNo ratings yet
- Microsoft Security Product Roadmap Brief All Invitations-2023 AprilDocument5 pagesMicrosoft Security Product Roadmap Brief All Invitations-2023 Apriltsai wen yenNo ratings yet
- GC 1999 03 Minas BrethilDocument5 pagesGC 1999 03 Minas BrethilErszebethNo ratings yet
- TN Govt RecruitmentDocument12 pagesTN Govt RecruitmentPriyanka ShankarNo ratings yet
- RCD-GillesaniaDocument468 pagesRCD-GillesaniaJomarie Alcano100% (2)
- Solutions for QAT1001912Document3 pagesSolutions for QAT1001912NaveenNo ratings yet
- 2024 Yoga Vidya Training FormDocument8 pages2024 Yoga Vidya Training FormJohnNo ratings yet
- Air Brake System For Railway CoachesDocument40 pagesAir Brake System For Railway CoachesShashwat SamdekarNo ratings yet