You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Appi Ajp 2021 21111134 PDFDocument4 pagesAppi Ajp 2021 21111134 PDFSteve aokiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Herpes Zoster & KatarakDocument6 pagesHerpes Zoster & KatarakSteve aokiNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Anxiety Disorders and Age Related Changes in Physiology PDFDocument10 pagesAnxiety Disorders and Age Related Changes in Physiology PDFSteve aokiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Risk Factors Associated With Psychiatric Comorbidities Among Suicide AttemptersDocument8 pagesRisk Factors Associated With Psychiatric Comorbidities Among Suicide AttemptersSteve aokiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Tobacco Smoking, Related Harm and Motivation To Quit Smoking in People With Schizophrenia Spectrum DisordersDocument17 pagesTobacco Smoking, Related Harm and Motivation To Quit Smoking in People With Schizophrenia Spectrum DisordersSteve aokiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Outcomes of Cardiopulmonary Resuscitation in The Emergency DepartmentDocument4 pagesOutcomes of Cardiopulmonary Resuscitation in The Emergency DepartmentSteve aokiNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Angioedema in Systemic Lupus Erythematosus (SLE) in Emergency Setting: A Case ReportDocument6 pagesAngioedema in Systemic Lupus Erythematosus (SLE) in Emergency Setting: A Case ReportSteve aokiNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- DMSO 354627 Ramadan and Diabetes What About Non Fasting Patients With DDocument9 pagesDMSO 354627 Ramadan and Diabetes What About Non Fasting Patients With DSteve aokiNo ratings yet
- Drowning Management and Prevention: Summer HazardsDocument4 pagesDrowning Management and Prevention: Summer HazardsSteve aokiNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- 2022 Lin Sun - Difference of Serum Cytokine Profile in Allergic A RetrieveDocument12 pages2022 Lin Sun - Difference of Serum Cytokine Profile in Allergic A RetrieveSteve aokiNo ratings yet
- 2022 Miguel Angel Diaz - Clinical Features and Outcomes Associated With BroDocument7 pages2022 Miguel Angel Diaz - Clinical Features and Outcomes Associated With BroSteve aokiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Lasers: Outpatient Transurethral Cystolithotripsy of Large Bladder Stones by Holmium LaserDocument4 pagesLasers: Outpatient Transurethral Cystolithotripsy of Large Bladder Stones by Holmium LaserSteve aokiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Use of Cryotherapy For Managing Chronic Pain - An Evidence-Based NarrativeDocument20 pagesUse of Cryotherapy For Managing Chronic Pain - An Evidence-Based NarrativeSteve aokiNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Rare Case of Flood Syndrome in Emergency Department: A Case Report and Review of Recent Reported CasesDocument4 pagesA Rare Case of Flood Syndrome in Emergency Department: A Case Report and Review of Recent Reported CasesSteve aokiNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Antipsychotic Prescribing in DementiaDocument2 pagesAntipsychotic Prescribing in DementiaSteve aokiNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Icu BundlesDocument38 pagesIcu BundlesOsama BishtNo ratings yet
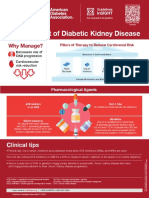
- Management of Diabetic Kidney Disease Updated 0Document1 pageManagement of Diabetic Kidney Disease Updated 0Jia-PeiWuNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Isolation and Hydrolysis of Casein From MilkDocument6 pagesIsolation and Hydrolysis of Casein From MilkPAUL CEDRIC BERNARDONo ratings yet
- History and Physical Exam For COPDDocument2 pagesHistory and Physical Exam For COPDKarenJulioNo ratings yet
- Infiltration, A New Therapy For Masking Enamel White Spot PDFDocument12 pagesInfiltration, A New Therapy For Masking Enamel White Spot PDFwijayanti siswantoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Roof Work HIRARCDocument4 pagesRoof Work HIRARCSarah Liyana86% (7)
- 1200 từ thường gặp trong listeningDocument5 pages1200 từ thường gặp trong listeningbunbunvyvyNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Genetic MaterialDocument2 pagesGenetic MaterialSammie GotchuNo ratings yet
- Roman Catholic: Lucena City, PHDocument4 pagesRoman Catholic: Lucena City, PHJennet RiveraNo ratings yet
- Behavior Change Theories and ModelsDocument4 pagesBehavior Change Theories and ModelsSintija100% (5)
- FT Schedule RM Phase 1Document1 pageFT Schedule RM Phase 1Virat ValiNo ratings yet
- Waste Management Plan-1Document16 pagesWaste Management Plan-1usama basionyNo ratings yet
- Unit-8 - Assignment-1 - WAGOLL 4Document3 pagesUnit-8 - Assignment-1 - WAGOLL 4Alisha AliNo ratings yet
- Seminar Kimia SPM Mmu 2017 CG Adura Jawapan Kertas 2 PDFDocument48 pagesSeminar Kimia SPM Mmu 2017 CG Adura Jawapan Kertas 2 PDFNoorleha Mohd YusoffNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Ryzon Baking BookDocument88 pagesRyzon Baking Bookbsaracco1100% (4)
- NCP For UtiDocument3 pagesNCP For UtiAaron Sanchez100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Jawaharlal Nehru Krishi Vishwa Vidyalaya, Jabalpur, Madhya PradeshDocument4 pagesJawaharlal Nehru Krishi Vishwa Vidyalaya, Jabalpur, Madhya PradeshSudhanshuAtkareNo ratings yet
- SB-78 (Traffic Advisory System)Document2 pagesSB-78 (Traffic Advisory System)Gerhard MNo ratings yet
- On Agents of MutationDocument22 pagesOn Agents of Mutationmine_ne361No ratings yet
- Sawa Server Training ManualDocument37 pagesSawa Server Training ManualVladan VujicNo ratings yet
- Double Displacement ReactionDocument7 pagesDouble Displacement Reactionlheanne manzulNo ratings yet
- 7 Days of Defining Moments: Chip Heath & Dan HeathDocument10 pages7 Days of Defining Moments: Chip Heath & Dan Heaththeowensgroup100% (1)
- Preboard 3 Plumbing Code Answer KeyDocument8 pagesPreboard 3 Plumbing Code Answer Keyfreanne_0527100% (5)
- Limit Sample PorosityDocument3 pagesLimit Sample PorosityJoeIsmailNo ratings yet
- Circontrol CirCarLife Catalogue PDFDocument38 pagesCircontrol CirCarLife Catalogue PDFfakesasoNo ratings yet
- Chapter 19 Notes 2015Document16 pagesChapter 19 Notes 2015Jason FanNo ratings yet
- Manual Vaporizador de GLP - Inglés PDFDocument54 pagesManual Vaporizador de GLP - Inglés PDFJhonattan Alvarez100% (1)
- Operational Procedure On Illegal Drugs and Vice ControlDocument18 pagesOperational Procedure On Illegal Drugs and Vice ControlJohn Lester PanaliganNo ratings yet
- Ground Water Quality Monitoring in A Developing Area Using Water Quality Index and Principal Component Analysis: A Case Study of Visakhapatnam IndiaDocument8 pagesGround Water Quality Monitoring in A Developing Area Using Water Quality Index and Principal Component Analysis: A Case Study of Visakhapatnam IndiaMallikarjuna Rao DuvvadaNo ratings yet
- Industrial Charcoal Production With Power Generation at Mully Children'S Family Yatta, KenyaDocument87 pagesIndustrial Charcoal Production With Power Generation at Mully Children'S Family Yatta, KenyapramitasNo ratings yet
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodFrom EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)