You might also like
- EKG/ECG Study GuideDocument13 pagesEKG/ECG Study GuideSherree HayesNo ratings yet
- Grammar Tests Upper Intermediate Determiners ...Document4 pagesGrammar Tests Upper Intermediate Determiners ...silvia0% (1)
- Hand and Wrist AAOS MCQ. 2019 PDFDocument158 pagesHand and Wrist AAOS MCQ. 2019 PDFantonio ferrer100% (2)
- TFN Reviewer PrelimsDocument8 pagesTFN Reviewer PrelimsCUBILLAS, JASMIN G.No ratings yet
- GCT ThumbDocument10 pagesGCT ThumbMoeez AkramNo ratings yet
- Giant Cell Tumor of The Phalanx of Finger: Case Reports: BackgroundDocument10 pagesGiant Cell Tumor of The Phalanx of Finger: Case Reports: BackgroundMoeez AkramNo ratings yet
- Sleeve Fracture of The Adult PatellaDocument3 pagesSleeve Fracture of The Adult PatellaRadenMasKaerNo ratings yet
- Giant Cell Tumor of Distal End of Femur With Pathological Fracture Treated by Resection and Megaprosthesis A Case ReportDocument5 pagesGiant Cell Tumor of Distal End of Femur With Pathological Fracture Treated by Resection and Megaprosthesis A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Management of Non-Metastatic Pelvic Bone Giant Cell Tumour by Resection, Extended Curettage and Reconstruction With Autograft and Allograft - A Case ReportDocument5 pagesManagement of Non-Metastatic Pelvic Bone Giant Cell Tumour by Resection, Extended Curettage and Reconstruction With Autograft and Allograft - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Giant Cell Tumor of The Tendon Sheath: A Rare Case in The Left Knee of A 15-Year-Old BoyDocument3 pagesGiant Cell Tumor of The Tendon Sheath: A Rare Case in The Left Knee of A 15-Year-Old BoyFriadi NataNo ratings yet
- Osteoblastoma A Spectrum of Presentation and TreatDocument10 pagesOsteoblastoma A Spectrum of Presentation and TreatmandetoperdiyuwanNo ratings yet
- 1 s2.0 S2049080122008718 MainDocument4 pages1 s2.0 S2049080122008718 MainFarizka Dwinda HidayatNo ratings yet
- Case Report: Osteomyelitis of The Patella in A 10-Year-Old Girl: A Case Report and Review of The LiteratureDocument6 pagesCase Report: Osteomyelitis of The Patella in A 10-Year-Old Girl: A Case Report and Review of The LiteratureIfal JakNo ratings yet
- Giant Cell Tumor of Tendon Sheath YjfasDocument6 pagesGiant Cell Tumor of Tendon Sheath YjfasPaulo Victor Dias AlmeidaNo ratings yet
- He 2019Document10 pagesHe 2019Rashif AkmalNo ratings yet
- Osteosarcoma of The Jaw: Report of 3 Cases (Including The Rare Epithelioid Variant) With Review of LiteratureDocument10 pagesOsteosarcoma of The Jaw: Report of 3 Cases (Including The Rare Epithelioid Variant) With Review of LiteraturesTEVENNo ratings yet
- Multifocal Giant Cell Tumor of The Carpus Unusua 2024 International JournalDocument5 pagesMultifocal Giant Cell Tumor of The Carpus Unusua 2024 International JournalRonald QuezadaNo ratings yet
- Isolated Lesser Trochanter Fracture Associated With LeukemiaDocument3 pagesIsolated Lesser Trochanter Fracture Associated With LeukemiaIndora DenniNo ratings yet
- Giant Cell Tumor of The Thoracal Spine Case Report 2020Document4 pagesGiant Cell Tumor of The Thoracal Spine Case Report 2020Ignatius Rheza SetiawanNo ratings yet
- Ispub 14140Document7 pagesIspub 14140Okkie Mharga SentanaNo ratings yet
- Ringe 2013Document3 pagesRinge 2013Minh ChíNo ratings yet
- 2020 Infantile Tuberculous Osteomyelitis of The Proximal TibiaDocument4 pages2020 Infantile Tuberculous Osteomyelitis of The Proximal TibiaMuhammad Muttaqee MisranNo ratings yet
- A Case of Eccrine Tumour Metastasis To Spine Managed With Posterior Spinal Stabilization With Recovering ParaparesisDocument3 pagesA Case of Eccrine Tumour Metastasis To Spine Managed With Posterior Spinal Stabilization With Recovering ParaparesisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cervical Osteomyelitis and An Epidural Abscess: An Unusual Form of Cat-Scratch Disease in One CaseDocument5 pagesCervical Osteomyelitis and An Epidural Abscess: An Unusual Form of Cat-Scratch Disease in One CaseRashmeeta ThadhaniNo ratings yet
- Primary Normo-Phosphatemic Tumoral Calcinosis - A Rare EntityDocument4 pagesPrimary Normo-Phosphatemic Tumoral Calcinosis - A Rare EntityIJAR JOURNALNo ratings yet
- Extra Cranial MetastasesDocument5 pagesExtra Cranial MetastasesJayendra Kumar AryaNo ratings yet
- Metastatic Vertebral Lesion Mimicking An Atypical Hemangioma WithDocument8 pagesMetastatic Vertebral Lesion Mimicking An Atypical Hemangioma Withsica_17_steaua6519No ratings yet
- Aspe 02 0177Document3 pagesAspe 02 0177igeltangdiayuNo ratings yet
- Cureus 0012 00000008855 PDFDocument11 pagesCureus 0012 00000008855 PDFAlberto BrahmNo ratings yet
- International Journal of Advances in Case ReportsDocument3 pagesInternational Journal of Advances in Case ReportsastritriNo ratings yet
- 1808 8694 Bjorl 86 s1 0s23Document3 pages1808 8694 Bjorl 86 s1 0s23VITOR PEREZNo ratings yet
- Tuberculous Osteomyelitis Mimicking A Lytic Bone Tumor: Report of Two Cases and Literature ReviewDocument5 pagesTuberculous Osteomyelitis Mimicking A Lytic Bone Tumor: Report of Two Cases and Literature ReviewazevedoNo ratings yet
- Medicine: Spontaneous Rupture of Solid Pseudopapillary Tumor of PancreasDocument8 pagesMedicine: Spontaneous Rupture of Solid Pseudopapillary Tumor of PancreasPatricia BezneaNo ratings yet
- Potts Puffy Tumour 4Document3 pagesPotts Puffy Tumour 4kityamuwesiNo ratings yet
- Adi Wasis Prakosa - Poster FulltextDocument11 pagesAdi Wasis Prakosa - Poster FulltextAdi Wasis PrakosaNo ratings yet
- Primum Non Nocere - First Do No HarmDocument4 pagesPrimum Non Nocere - First Do No HarmSuci AprilyaNo ratings yet
- A Rare Case of Large Size Undifferentiated Pleomorphic Sarcoma of AnkleDocument5 pagesA Rare Case of Large Size Undifferentiated Pleomorphic Sarcoma of AnkleIJAR JOURNALNo ratings yet
- Keithbidwell 1987Document5 pagesKeithbidwell 1987Ignatius Rheza SetiawanNo ratings yet
- Ecr2015 c-1165Document28 pagesEcr2015 c-1165Fitri Amelia RizkiNo ratings yet
- 2017 Article 713Document5 pages2017 Article 713فرجني موغNo ratings yet
- Case Report: Zehava Sadka Rosenberg, 1 Steven Shankman, 1 Michael Klein, 2'3 and Wallace Lehman4Document3 pagesCase Report: Zehava Sadka Rosenberg, 1 Steven Shankman, 1 Michael Klein, 2'3 and Wallace Lehman4Mohamed Ali Al-BuflasaNo ratings yet
- Unusual Presentation of Adamantinoma With Synchronous 2024 International JouDocument5 pagesUnusual Presentation of Adamantinoma With Synchronous 2024 International JouRonald QuezadaNo ratings yet
- ONCO 21 Desember 2020 Undiferentiated Pleomorfic Sarcoma Rev 1Document46 pagesONCO 21 Desember 2020 Undiferentiated Pleomorfic Sarcoma Rev 1ciptakarwanaNo ratings yet
- Jurnal 2Document6 pagesJurnal 2alexxxxxNo ratings yet
- Visual Diagnosis in Emergency Medicine: Superior Dislocation of The Patella: Case Report and Review of The LiteratureDocument3 pagesVisual Diagnosis in Emergency Medicine: Superior Dislocation of The Patella: Case Report and Review of The LiteratureTrisna AuliaNo ratings yet
- Patellar Tendon Avulsion With Tibial Tuberosity SLDocument4 pagesPatellar Tendon Avulsion With Tibial Tuberosity SLKirana ArinNo ratings yet
- Ijerph 19 05837Document9 pagesIjerph 19 05837chan kyoNo ratings yet
- Plantillo Anteromedial + LCP + ApeDocument7 pagesPlantillo Anteromedial + LCP + ApeThiagoNo ratings yet
- Mandibular Traumatic Peripheral Osteoma: A Case ReportDocument5 pagesMandibular Traumatic Peripheral Osteoma: A Case ReportrajtanniruNo ratings yet
- Tuberculosis of Talus A Case ReportDocument4 pagesTuberculosis of Talus A Case ReportPutra DariusNo ratings yet
- Giant CellDocument5 pagesGiant CellTamimahNo ratings yet
- Primary Ewing Sarcoma of The Adrenal Gland: A Rare Cause of Abdominal MassDocument6 pagesPrimary Ewing Sarcoma of The Adrenal Gland: A Rare Cause of Abdominal MassAndra KurniantoNo ratings yet
- TB Arthritis Ankle Mimicking SynovitisDocument8 pagesTB Arthritis Ankle Mimicking SynovitisAzmi FarhadiNo ratings yet
- 485-Article Text-5030-1-10-20100605 PDFDocument4 pages485-Article Text-5030-1-10-20100605 PDFAndreas NatanNo ratings yet
- Cuti Bacterium 2019 Aid2019Document10 pagesCuti Bacterium 2019 Aid2019Vita BūdvytėNo ratings yet
- Caso Clinico Sp3Document4 pagesCaso Clinico Sp3eduardoNo ratings yet
- Clavicle Fracture Following Neck Dissection: Imaging Features and Natural CourseDocument6 pagesClavicle Fracture Following Neck Dissection: Imaging Features and Natural CourseAngel IschiaNo ratings yet
- Pi Is 1991790212001626Document6 pagesPi Is 1991790212001626Lina NiatiNo ratings yet
- Scientific Abstracts Friday, 14 June 2019 1015Document1 pageScientific Abstracts Friday, 14 June 2019 1015حسام الدين إسماعيلNo ratings yet
- Mi TsuyamaDocument8 pagesMi TsuyamatnsourceNo ratings yet
- Osteomielitis PatelarDocument3 pagesOsteomielitis PatelarAlexander DanielNo ratings yet
- 1 PBDocument5 pages1 PBrahmat senjayaNo ratings yet
- Unicompartmental Knee Arthroplasty: Indications, Surgical Techniques and ComplicationsFrom EverandUnicompartmental Knee Arthroplasty: Indications, Surgical Techniques and ComplicationsTad L. GerlingerNo ratings yet
- Infantile Hemangioendothelioma: Bafana Elliot Hlatshwayo, Daba Ipfi, Sipho SitholeDocument4 pagesInfantile Hemangioendothelioma: Bafana Elliot Hlatshwayo, Daba Ipfi, Sipho SitholeDrAbdullah HajarNo ratings yet
- Spectrum of Teratoma: From Head To Toe, Radiological Pathological CorrelationDocument33 pagesSpectrum of Teratoma: From Head To Toe, Radiological Pathological CorrelationDrAbdullah HajarNo ratings yet
- AIUM Practice Parameter For The Performance of A Peripheral Venous Ultrasound ExaminationDocument8 pagesAIUM Practice Parameter For The Performance of A Peripheral Venous Ultrasound ExaminationDrAbdullah HajarNo ratings yet
- NEW Sat 1255 Imperial Whitelaw Protocols NEWDocument5 pagesNEW Sat 1255 Imperial Whitelaw Protocols NEWDrAbdullah HajarNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument12 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDrAbdullah HajarNo ratings yet
- CMR 00062-17Document78 pagesCMR 00062-17pokhara144No ratings yet
- English 10 1st Quarter Examination 22Document4 pagesEnglish 10 1st Quarter Examination 22Christian Jay PresiidenteNo ratings yet
- ArticleDocument10 pagesArticleperley.matiasNo ratings yet
- LIFESCI 2N03: Human: Nutrition For Life ScienceDocument40 pagesLIFESCI 2N03: Human: Nutrition For Life ScienceAnnalisa NguyenNo ratings yet
- Accuracy of Focused Assessment With Sonography For Trauma (FAST) in Blunt Trauma Abdomen - A Prospective StudyDocument5 pagesAccuracy of Focused Assessment With Sonography For Trauma (FAST) in Blunt Trauma Abdomen - A Prospective StudyEdison HernandezNo ratings yet
- Incorporating Mental Health Screening Into Adolescent Office VisitsDocument3 pagesIncorporating Mental Health Screening Into Adolescent Office VisitsnataliasulistyoNo ratings yet
- Harga KhususDocument16 pagesHarga KhususNoperitaNo ratings yet
- Persuasive Speech On HealthcareDocument4 pagesPersuasive Speech On HealthcareRobanderson126No ratings yet
- Revised PPAR-Q Aug. 2022Document2 pagesRevised PPAR-Q Aug. 2022RAY LORENZO LAGASCANo ratings yet
- Jurnal Ckd-EpiDocument6 pagesJurnal Ckd-EpinezaNo ratings yet
- D HC OperatorsDocument5,396 pagesD HC OperatorsCoupon VampireNo ratings yet
- P.e12 Lesson Safety ProtocolDocument23 pagesP.e12 Lesson Safety ProtocolArcLosephNo ratings yet
- Cardiopulmonary Resuscitation (CPR) : Akper BookDocument4 pagesCardiopulmonary Resuscitation (CPR) : Akper BookFitriana Noor SabrinaNo ratings yet
- Summer and Winter VacationsDocument5 pagesSummer and Winter VacationsYahia IdressNo ratings yet
- E-Cigarette Wholesale Distributor in USA - Vape Supplier in USADocument10 pagesE-Cigarette Wholesale Distributor in USA - Vape Supplier in USAAnjum JohnNo ratings yet
- HIS Analogy ExplanationDocument1 pageHIS Analogy ExplanationJake PendonNo ratings yet
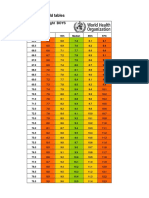
- Boys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Document4 pagesBoys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Gabrielly LopesNo ratings yet
- Republic of The Philippines Central Mindanao University College of NURSING University Town, Musuan, Maramag, BukidnonDocument2 pagesRepublic of The Philippines Central Mindanao University College of NURSING University Town, Musuan, Maramag, BukidnonJastine SabornidoNo ratings yet
- 02 - Establishing Background Levels - EPA - 1995Document7 pages02 - Establishing Background Levels - EPA - 1995JessikaNo ratings yet
- Instructions For Use: Technical InformationDocument5 pagesInstructions For Use: Technical InformationRiska SagitaNo ratings yet
- Ad Iver Nion Ad Iver Nion Ad Iver NionDocument8 pagesAd Iver Nion Ad Iver Nion Ad Iver NionMad River UnionNo ratings yet
- Eustachian TubeDocument6 pagesEustachian TubeNaruto_Uchiha777No ratings yet
- Walkthrough21 PDFDocument51 pagesWalkthrough21 PDFAnas SantyNo ratings yet
- Rinchuse 2006Document10 pagesRinchuse 2006Natalie JaraNo ratings yet
- PETRONAS Fuel Oil 80: Safety Data SheetDocument10 pagesPETRONAS Fuel Oil 80: Safety Data SheetJaharudin JuhanNo ratings yet
- Chapter 10Document55 pagesChapter 10Aimah ManafNo ratings yet
- Operating RoomDocument13 pagesOperating RoomrichardNo ratings yet