You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Peanuts 13Document3 pagesPeanuts 13Akshay KumarNo ratings yet
- Peanuts 11Document2 pagesPeanuts 11Akshay KumarNo ratings yet
- Peanuts 6Document3 pagesPeanuts 6Akshay KumarNo ratings yet
- Peanuts 12Document2 pagesPeanuts 12Akshay KumarNo ratings yet
- Peanuts 5Document2 pagesPeanuts 5Akshay KumarNo ratings yet
- Peanuts 3Document3 pagesPeanuts 3Akshay KumarNo ratings yet
- Peanuts 4Document2 pagesPeanuts 4Akshay KumarNo ratings yet
- Peanut Growing Science 18 - копияDocument1 pagePeanut Growing Science 18 - копияAkshay KumarNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Clsi H18 A3 PDFDocument52 pagesClsi H18 A3 PDFyandros666100% (2)
- Nurseslabs Normal Lab Values 1.2 PDFDocument5 pagesNurseslabs Normal Lab Values 1.2 PDFPrincess BaciaNo ratings yet
- IsoflavonsDocument23 pagesIsoflavonsPiyush KhetrapalNo ratings yet
- MCT Oil Powder PDFDocument3 pagesMCT Oil Powder PDFviand vanillalyciousNo ratings yet
- Bleeding Time PDFDocument6 pagesBleeding Time PDFMedic Guru100% (1)
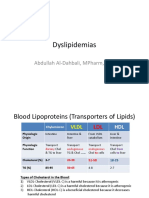
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDDocument15 pagesDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- Physiological Changes During Pregnancy 2-1Document32 pagesPhysiological Changes During Pregnancy 2-1PATRICK ROSHAN ANo ratings yet
- Time: 1 Hr. 30 Min. Total Marks: 60: Important InformationDocument9 pagesTime: 1 Hr. 30 Min. Total Marks: 60: Important Informationrishab KumarNo ratings yet
- Laboratory Department Tracking Sheet OriginalDocument124 pagesLaboratory Department Tracking Sheet OriginalCharmaine Corpuz GranilNo ratings yet
- Anp 120 Test 2Document22 pagesAnp 120 Test 2Joseph A MwitupaNo ratings yet
- 242 Vivinal Milk Fat Brochure PDFDocument11 pages242 Vivinal Milk Fat Brochure PDFCarlos MedinaNo ratings yet
- CIMS Health Checkup Brochure (English) PDFDocument4 pagesCIMS Health Checkup Brochure (English) PDFVaibhavNo ratings yet
- Aldosterone ELISA: Instructions For UseDocument39 pagesAldosterone ELISA: Instructions For UseYousra ZeidanNo ratings yet
- Lab Values 1Document30 pagesLab Values 1Ezekiel John GarciaNo ratings yet
- Case Study 3 StrokeDocument4 pagesCase Study 3 Strokeapi-643214419No ratings yet
- Food Chemistry: Ibironke A. Ajayi, Rotimi A. Oderinde, Victor O. Taiwo, Emmanuel O. AgbedanaDocument8 pagesFood Chemistry: Ibironke A. Ajayi, Rotimi A. Oderinde, Victor O. Taiwo, Emmanuel O. AgbedanaIngrid DantasNo ratings yet
- Analysis of Sugars PDFDocument29 pagesAnalysis of Sugars PDFAbu RaihanNo ratings yet
- Ceutics FormulaDocument1 pageCeutics FormulaAyda SalehiNo ratings yet
- MtSinai PatientGuideDocument40 pagesMtSinai PatientGuideobada alrefaiNo ratings yet
- Tracking of Glycated Hemoglobin in The Original Cohort of The Framingham Heart StudyDocument7 pagesTracking of Glycated Hemoglobin in The Original Cohort of The Framingham Heart StudySanghita BiswasNo ratings yet
- Nutritional Calculator - Free (Only 50 Foods) : Designed byDocument2 pagesNutritional Calculator - Free (Only 50 Foods) : Designed bySrinivas Kumar MiriyalaNo ratings yet
- Randox IQC - LT027-Acusera-third-party-controls-DEC20Document120 pagesRandox IQC - LT027-Acusera-third-party-controls-DEC20Artinee JarusaksakulNo ratings yet
- Clotting Time PDFDocument17 pagesClotting Time PDFKhaled ZatariNo ratings yet
- Pediatric Reference Ranges Endocrinology 0981 PDFDocument14 pagesPediatric Reference Ranges Endocrinology 0981 PDFMMCSTORENo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument10 pagesHaematology: Investigation Observed Value Unit Biological Reference IntervalVanshitaNo ratings yet
- The Endocrine Pancreas: Regulation of Carbohydrate MetabolismDocument61 pagesThe Endocrine Pancreas: Regulation of Carbohydrate MetabolismNona AsolaNo ratings yet
- BF FDT Lyse: NO Tindakan Lab BMHP A Hematologi Jumlah Bmhp/TindakanDocument16 pagesBF FDT Lyse: NO Tindakan Lab BMHP A Hematologi Jumlah Bmhp/TindakanDewita Wulan PratiwiNo ratings yet
- 08 - Allowable Error Table 2014-FinalDocument14 pages08 - Allowable Error Table 2014-FinalFe Rackle Pisco JamerNo ratings yet
- AnnexD PhilHealthKonsultaBenefitTableDocument1 pageAnnexD PhilHealthKonsultaBenefitTableMaluso Water DistrictNo ratings yet
- Laboratory Title:: Practical 6: Qualitative Test For CarbohydrateDocument3 pagesLaboratory Title:: Practical 6: Qualitative Test For CarbohydrateThe seriNo ratings yet