You might also like
- Mould IdentificationDocument24 pagesMould Identificationanon_biochemistrystudentNo ratings yet
- Buller (1909) - Researches On Fungi 1Document326 pagesBuller (1909) - Researches On Fungi 1Attila Koszka100% (1)
- Dermatophytosis in Northern AfricaDocument8 pagesDermatophytosis in Northern Africaabznaim420No ratings yet
- Tinea Capitis Study in Children Under 13Document4 pagesTinea Capitis Study in Children Under 13TantriSaptennoPattiradjawaneNo ratings yet
- Emergence of Trichophyton mentagrophytes as a common cause of Tinea CorporisDocument5 pagesEmergence of Trichophyton mentagrophytes as a common cause of Tinea CorporisjmuhilanNo ratings yet
- TPMD 200176Document2 pagesTPMD 200176Marcelita DuwiriNo ratings yet
- Tinea Capitis in Adolescent: A Case Report: Laporan KasusDocument8 pagesTinea Capitis in Adolescent: A Case Report: Laporan KasusNadya Ananda SariNo ratings yet
- A Cross Sectional Study To Observe The Diversity of Fungal Species in Onychomycosis Isolated From A Tertiary Care Hospital in KarachiDocument4 pagesA Cross Sectional Study To Observe The Diversity of Fungal Species in Onychomycosis Isolated From A Tertiary Care Hospital in KarachiMini LaksmiNo ratings yet
- Recent Advances in The Diagnosis of DermatophytosisDocument11 pagesRecent Advances in The Diagnosis of DermatophytosishansmeetNo ratings yet
- Kredics Et Al 2015Document18 pagesKredics Et Al 2015Palanisamy ManikandanNo ratings yet
- Scabies in ChildrenDocument7 pagesScabies in ChildrenanantaNo ratings yet
- Tinea Capitis Among Children at One Suburban Primary School: in The City of Maputo, MozambiqueDocument3 pagesTinea Capitis Among Children at One Suburban Primary School: in The City of Maputo, MozambiqueTantriSaptennoPattiradjawaneNo ratings yet
- 5 Goffar Deardo SaragihDocument5 pages5 Goffar Deardo SaragihJoe BitchNo ratings yet
- A Case Report of Crusted ScabiesDocument7 pagesA Case Report of Crusted ScabiesKlinik Pratama Ar-Raudhah 129No ratings yet
- 2016 Piis1201971216310761Document4 pages2016 Piis1201971216310761Soraya Eugenia Morales LópezNo ratings yet
- Journal-Of-Dermatology-Research-And-Therapy-Ijdrt-6-090Document6 pagesJournal-Of-Dermatology-Research-And-Therapy-Ijdrt-6-090seydou.organismNo ratings yet
- Moshirfar Et Al. - 2019 - Biological Staining and Culturing in Infectious KeDocument7 pagesMoshirfar Et Al. - 2019 - Biological Staining and Culturing in Infectious KesyramadhantiNo ratings yet
- Epidemiology of dermatophytoses in TunisiaDocument6 pagesEpidemiology of dermatophytoses in TunisiasantiNo ratings yet
- Mangament TerapaiDocument9 pagesMangament TerapaiAnonymous gn7tMio2PNo ratings yet
- 648 FullDocument5 pages648 Fullibrahima1968No ratings yet
- Epidemiological Characterization of Dermatomycosis in EthiopiaDocument7 pagesEpidemiological Characterization of Dermatomycosis in EthiopiaMini LaksmiNo ratings yet
- Incidence and Prevalence of Dermatophytosis in and Around Chennai, Tamilnadu, IndiaDocument6 pagesIncidence and Prevalence of Dermatophytosis in and Around Chennai, Tamilnadu, IndiaYanna RizkiaNo ratings yet
- Jurnal TC KohDocument4 pagesJurnal TC KohariefNo ratings yet
- The Kerion An Angry Tinea Capitis PBDocument7 pagesThe Kerion An Angry Tinea Capitis PBprajnamitaNo ratings yet
- 35429-Article Text-126139-2-10-20180206Document5 pages35429-Article Text-126139-2-10-20180206Robertus RonnyNo ratings yet
- Review: Tinea Corporis: An Updated ReviewDocument22 pagesReview: Tinea Corporis: An Updated ReviewMade SetiadjiNo ratings yet
- 20 145 1 PBDocument9 pages20 145 1 PBChristo LimbongNo ratings yet
- Study On Pityriasis Versicolor in Patients Referred To Clinics in TabrizDocument5 pagesStudy On Pityriasis Versicolor in Patients Referred To Clinics in TabrizMiranda Yudhi CyubidubiduuNo ratings yet
- Jurnal DermatomDocument6 pagesJurnal DermatomEstyka RatuNo ratings yet
- Dermatophytes and Dermatophytosis in TheDocument17 pagesDermatophytes and Dermatophytosis in Theabznaim420No ratings yet
- Update On The Treatment of Molluscum Contagiosum in ChildrenDocument9 pagesUpdate On The Treatment of Molluscum Contagiosum in Childrensamsara vrindaNo ratings yet
- Accepted ManuscriptDocument7 pagesAccepted ManuscriptNaomiNo ratings yet
- Scabies: Application of The Novel Identify-Isolate-Inform Tool For Detection and ManagementDocument8 pagesScabies: Application of The Novel Identify-Isolate-Inform Tool For Detection and Managementraudhatul muttaqinNo ratings yet
- Artikel 3Document6 pagesArtikel 3sesiaNo ratings yet
- A Study On Clinico-Etiological Profile of Mycotic Keratitis in Tertiary Care Hospital at Government Medical College, Kota (Rajasthan)Document7 pagesA Study On Clinico-Etiological Profile of Mycotic Keratitis in Tertiary Care Hospital at Government Medical College, Kota (Rajasthan)IJAR JOURNALNo ratings yet
- Journal Reading - Update On The Management of Infectious KeratitisDocument23 pagesJournal Reading - Update On The Management of Infectious Keratitistasya noerchaerunisaNo ratings yet
- Revista Chilena de InfectologíaDocument28 pagesRevista Chilena de InfectologíadzenitNo ratings yet
- 1 s2.0 S1286457912001918 MainDocument8 pages1 s2.0 S1286457912001918 Mainabznaim420No ratings yet
- Clinicomycological Profile of Superficial Fungal Infections in North IndiaDocument8 pagesClinicomycological Profile of Superficial Fungal Infections in North IndiaasfwegereNo ratings yet
- Iran FungusDocument7 pagesIran FungusHaruka KanataNo ratings yet
- Otomycosis in CSOM Patients Effectively Treated with Clotrimazole Ear DropsDocument4 pagesOtomycosis in CSOM Patients Effectively Treated with Clotrimazole Ear DropsShovie Thalia MirandaNo ratings yet
- Ulkus 5Document7 pagesUlkus 5Vidya Ismi AuliaNo ratings yet
- Update SkrofulodermaDocument8 pagesUpdate SkrofulodermaPororo KewrenNo ratings yet
- Microbiologi of Chronic Suppurative Otitis MediaDocument3 pagesMicrobiologi of Chronic Suppurative Otitis MediaDwi Ayu NilamsariNo ratings yet
- Thesis Protocol For M.S. Degree (Ophthalmology)Document31 pagesThesis Protocol For M.S. Degree (Ophthalmology)zebaNo ratings yet
- Microbiological Profile and Antimicrobial Sensitivity Pattern of Culture Positive Bacterial Keratitis: A Prospective Observational StudyDocument5 pagesMicrobiological Profile and Antimicrobial Sensitivity Pattern of Culture Positive Bacterial Keratitis: A Prospective Observational StudyBombong NurpaginoNo ratings yet
- Eryth Ras MaDocument5 pagesEryth Ras MaGilar Kusuma HadiNo ratings yet
- Zoo 1Document3 pagesZoo 1nurul rezki fitrianiazisNo ratings yet
- Trop Med 140515Document10 pagesTrop Med 140515Arfa AlyaNo ratings yet
- Evaluation of A Commercial PCR Test For The Diagnosis of Dermatophyte Nail InfectionsDocument7 pagesEvaluation of A Commercial PCR Test For The Diagnosis of Dermatophyte Nail Infectionsckcy ahaiNo ratings yet
- Nama: Endah Suryani NPM: 0661 16 179 Kelas: KELAS E'16Document5 pagesNama: Endah Suryani NPM: 0661 16 179 Kelas: KELAS E'16Endah SuryaniNo ratings yet
- Jjurnal InternasionalDocument4 pagesJjurnal Internasionalckcy ahaiNo ratings yet
- Scabies Application of The No PDFDocument10 pagesScabies Application of The No PDFYosia KevinNo ratings yet
- Prevention, Diagnosis, and Management of Acute Postoperative Bacterial EndophthalmitisDocument16 pagesPrevention, Diagnosis, and Management of Acute Postoperative Bacterial EndophthalmitisNiñoTanNo ratings yet
- 298-787-1-SMDocument15 pages298-787-1-SMinstallment paymentNo ratings yet
- 1 jISHADocument5 pages1 jISHAFirman MufidNo ratings yet
- Severe DermatoDocument13 pagesSevere DermatoadriantiariNo ratings yet
- Insight Into ScabiesDocument3 pagesInsight Into ScabiesVicky Pérez KlalaNo ratings yet
- Tinea Pedis An UpdateDocument5 pagesTinea Pedis An UpdateRahmat MuliaNo ratings yet
- A Review of The Monkeypox Virus and A Recent Outbreak of Skin Rash Disease in Nigeria: Kabuga and El ZowalatyDocument9 pagesA Review of The Monkeypox Virus and A Recent Outbreak of Skin Rash Disease in Nigeria: Kabuga and El ZowalatyNers LollipopNo ratings yet
- Clinically Relevant Mycoses: A Practical ApproachFrom EverandClinically Relevant Mycoses: A Practical ApproachElisabeth PresterlNo ratings yet
- The Essential Facts of FungusDocument2 pagesThe Essential Facts of FungusCantika Quita100% (2)
- SinónimosDocument9 pagesSinónimossergioNo ratings yet
- Medical Mycology: Study of FungiDocument4 pagesMedical Mycology: Study of FungiJerson Aizpuro SuplementoNo ratings yet
- The DermaphocytesDocument11 pagesThe DermaphocytescatuiraneljhayyyNo ratings yet
- Dermatofitosis 2011 1Document35 pagesDermatofitosis 2011 1Carmen Cajina Doña MamiNo ratings yet
- New alpine lichen species from TasmaniaDocument8 pagesNew alpine lichen species from TasmaniaGabriel Felipe PenalozaNo ratings yet
- Basic Concepts in MycologyDocument1 pageBasic Concepts in MycologyAngeloMartinNo ratings yet
- Fusarium RoseumDocument5 pagesFusarium RoseumbenzzzxNo ratings yet
- Cutaneous and Subcutaneous mycoses-FMS2-2558Document68 pagesCutaneous and Subcutaneous mycoses-FMS2-2558Marl EstradaNo ratings yet
- 2010 2 Analiza Rizika I Sustav Osiguranja Sigurnosti Hrane U Proizvodnji Polutrajnih Kobasica PDFDocument7 pages2010 2 Analiza Rizika I Sustav Osiguranja Sigurnosti Hrane U Proizvodnji Polutrajnih Kobasica PDFDragana IlijevskaNo ratings yet
- Shiva Mushroom Farm Spawn Centre PDFDocument6 pagesShiva Mushroom Farm Spawn Centre PDFMahesh NaikNo ratings yet
- Filogenetica de Fungos ArtigoDocument187 pagesFilogenetica de Fungos ArtigoMartival SantosNo ratings yet
- Methods For Identification and Conservation of Macro Fungus: A Probable Global FoodDocument9 pagesMethods For Identification and Conservation of Macro Fungus: A Probable Global FoodAsaddul IzzanNo ratings yet
- Orange Berry RustDocument2 pagesOrange Berry RustsararmentaNo ratings yet
- OnionDocument20 pagesOnionAnurAg KerkettaNo ratings yet
- Armillaria SolidipesDocument9 pagesArmillaria SolidipesIzzah Akimoto AyumuNo ratings yet
- 19.5 Study GuideDocument3 pages19.5 Study GuideSaraNo ratings yet
- Declercq B. 2012 - Hymenoscyphus Iricolens, A New Species On Iris Pseudacorus. Sterbeeckia 31-34-36Document3 pagesDeclercq B. 2012 - Hymenoscyphus Iricolens, A New Species On Iris Pseudacorus. Sterbeeckia 31-34-36Bernard DeclercqNo ratings yet
- Kerapatan Spora 5Document13 pagesKerapatan Spora 5Nurul Dilla DillaNo ratings yet
- Soliman Et Al. 2016Document23 pagesSoliman Et Al. 2016Anonymous 9xXl8wmBNo ratings yet
- Phylum: Basidiomycota General CharacteristicsDocument4 pagesPhylum: Basidiomycota General CharacteristicsRui MonteiroNo ratings yet
- Deuteromycota EnglishDocument6 pagesDeuteromycota EnglishMuhammad Nur50% (2)
- Toxic Fungi of Western NADocument166 pagesToxic Fungi of Western NALuci FerNo ratings yet
- MYCV 311: Week 4Document5 pagesMYCV 311: Week 4Janine Alicia VargasNo ratings yet
- The Hereford Fungus EatersDocument6 pagesThe Hereford Fungus Eatersj. l. hooverNo ratings yet
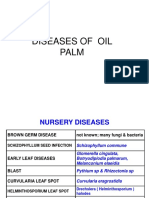
- Diseases of Oil Palm Pictures PpsDocument42 pagesDiseases of Oil Palm Pictures Ppsgafrnce60No ratings yet
- FungiDocument2 pagesFungiJuly RoldanNo ratings yet
- Mycology Fungi Flow ChartDocument4 pagesMycology Fungi Flow ChartS O50% (2)