You might also like
- Endoscopy in Pediatric Inflammatory Bowel DiseaseFrom EverandEndoscopy in Pediatric Inflammatory Bowel DiseaseLuigi Dall'OglioNo ratings yet
- DMCN 63 1351Document10 pagesDMCN 63 1351Jorge SilvaNo ratings yet
- Salivary Gland Botulinum Toxin Injections For Drooling in Children With Cerebral Palsy and Neurodevelopmental Disability A Systematic ReviewDocument11 pagesSalivary Gland Botulinum Toxin Injections For Drooling in Children With Cerebral Palsy and Neurodevelopmental Disability A Systematic Reviewsatyagraha84No ratings yet
- Otolaryngology Head and Neck Surgery 2014 Namin P76 7Document3 pagesOtolaryngology Head and Neck Surgery 2014 Namin P76 76mqpjqh2vqNo ratings yet
- Perioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceDocument10 pagesPerioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceBRENDA VANESSA TREVIZO ESTRADANo ratings yet
- Wabbels 2022Document11 pagesWabbels 2022Royner Edgardo Osorio ArauzNo ratings yet
- Gioacchi Ni 2015Document22 pagesGioacchi Ni 2015SaaraAlleyahAlAnaziNo ratings yet
- Prevalence of Malocclusion in Children With Sleep Disordered BreathingDocument4 pagesPrevalence of Malocclusion in Children With Sleep Disordered BreathingMu'taz ArmanNo ratings yet
- Nefertiti Lift BotoxDocument9 pagesNefertiti Lift BotoxAnamaria Zaccolo100% (2)
- PBD in Pediatric AchalasiaDocument6 pagesPBD in Pediatric AchalasiamuhammadfahmanNo ratings yet
- Neuromotor and Cognitive Functions in 4Document60 pagesNeuromotor and Cognitive Functions in 4ARICEL SALDIVIANo ratings yet
- Emerging Trends in Botulinum Neurotoxin A Resistance - An International Multidisciplinary Review and Consensus - Ho, 2022Document11 pagesEmerging Trends in Botulinum Neurotoxin A Resistance - An International Multidisciplinary Review and Consensus - Ho, 2022Rafael Autran Cavalcante AraújoNo ratings yet
- Nihms 1517802Document10 pagesNihms 1517802Asniar RNo ratings yet
- Adeno AnakDocument6 pagesAdeno Anakokky_rahmatNo ratings yet
- The Role of Doxycycline in The Management of CRSWPDocument6 pagesThe Role of Doxycycline in The Management of CRSWPLeonNo ratings yet
- Ultrasound-Guided Botulinum Toxin-A Injections Sialorrhea - BARBERO 2016Document7 pagesUltrasound-Guided Botulinum Toxin-A Injections Sialorrhea - BARBERO 2016Adriana BragaNo ratings yet
- Comparison of Clonidine and Fentanyl As An Adjuvant To Bupivacaine in Unilateral Spinal AnaesthesiaDocument11 pagesComparison of Clonidine and Fentanyl As An Adjuvant To Bupivacaine in Unilateral Spinal AnaesthesiaYadin SabudiNo ratings yet
- Treatment Outcomes of Oral Propranolol in The TreaDocument7 pagesTreatment Outcomes of Oral Propranolol in The TreabokobokobokanNo ratings yet
- Gow Gates Complications IIIDocument8 pagesGow Gates Complications IIIBeth AguiarNo ratings yet
- Management of Rare Causes of Pediatric Chronic Respiratory FailureDocument16 pagesManagement of Rare Causes of Pediatric Chronic Respiratory FailureISABEL SOFIA CABARCAS COGOLLONo ratings yet
- Sialoree BotoxDocument5 pagesSialoree BotoxJocul DivinNo ratings yet
- Jcpdigest 2015 7 42 7 640 646Document3 pagesJcpdigest 2015 7 42 7 640 646anshum guptaNo ratings yet
- 1 s2.0 S0302283822016803 MainDocument10 pages1 s2.0 S0302283822016803 MainDuda ShiraiwaNo ratings yet
- Bmjopen 2023 071959Document7 pagesBmjopen 2023 071959birkekocaunsalNo ratings yet
- Keywords:-Anaesthetics, Bupivacaine, Impaction, InferiorDocument8 pagesKeywords:-Anaesthetics, Bupivacaine, Impaction, InferiorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- International Journal of Pediatric Otorhinolaryngology: Ryan H. Belcher, James D. Phillips TDocument5 pagesInternational Journal of Pediatric Otorhinolaryngology: Ryan H. Belcher, James D. Phillips TMarcelaGutiérrezCarranzaNo ratings yet
- Cotofana 2021Document9 pagesCotofana 2021Emrys1987No ratings yet
- Univer Complu Madrid NBF Peri - Implant MucositisDocument10 pagesUniver Complu Madrid NBF Peri - Implant Mucositisjuan perezNo ratings yet
- Çocuklarda Sıvı Tedavisi Ile Pobk Arasındaki IlişkiDocument6 pagesÇocuklarda Sıvı Tedavisi Ile Pobk Arasındaki IlişkiAli ÖzdemirNo ratings yet
- Pediatric Chronic Sinusitis Diagnosis and ManagementDocument10 pagesPediatric Chronic Sinusitis Diagnosis and ManagementcaromoradNo ratings yet
- 2020 - Long-Term Non-Invasive Ventilation in Children - Current Use, Indications, and ContraindicationsDocument9 pages2020 - Long-Term Non-Invasive Ventilation in Children - Current Use, Indications, and ContraindicationsHack clashNo ratings yet
- Dapus Jurnal 2 Intravitreal Chemotherapy For Vitreous Disease inDocument7 pagesDapus Jurnal 2 Intravitreal Chemotherapy For Vitreous Disease inPutri kartiniNo ratings yet
- Congenital Nasolacrimal Duct Obstruction (CNLDO) - A ReviewDocument11 pagesCongenital Nasolacrimal Duct Obstruction (CNLDO) - A ReviewLovely PoppyNo ratings yet
- Journal Reading - Dr. Monika AyuningrumDocument12 pagesJournal Reading - Dr. Monika Ayuningrumamka chanNo ratings yet
- Surgical Intervention of Periocular Infantile Hemangiomas in the Era of β-BlockersDocument4 pagesSurgical Intervention of Periocular Infantile Hemangiomas in the Era of β-BlockersLuisa Fernanda ArboledaNo ratings yet
- Develop Med Child Neuro - 2018 - Swinney - Severity of Cerebral Palsy and Likelihood of Adverse Events After BotulinumDocument8 pagesDevelop Med Child Neuro - 2018 - Swinney - Severity of Cerebral Palsy and Likelihood of Adverse Events After BotulinumJorge SilvaNo ratings yet
- 10 1097@MD 0000000000008003Document6 pages10 1097@MD 0000000000008003asfwegereNo ratings yet
- SepDocument7 pagesSepyuyuNo ratings yet
- Lauder 2019Document12 pagesLauder 2019Julio AltamiranoNo ratings yet
- Iob Publication 1Document11 pagesIob Publication 1Nirmala JonnavithulaNo ratings yet
- Comparison of Repositioning Maneuvers For Benign Paroxysmal Positional Vertigo of Posterior Semicircular Canal: Advantages of Hybrid ManeuverDocument6 pagesComparison of Repositioning Maneuvers For Benign Paroxysmal Positional Vertigo of Posterior Semicircular Canal: Advantages of Hybrid ManeuverFayza RihastaraNo ratings yet
- 1 IiomainDocument6 pages1 IiomainyandaputriNo ratings yet
- Otitie Media Adhesiva JMCM - Volume 9 - Issue 1 - Pages 108-112Document5 pagesOtitie Media Adhesiva JMCM - Volume 9 - Issue 1 - Pages 108-112Teuku Ahmad HasanyNo ratings yet
- Randomized Controlled Trial of A Dichoptic Digital Therapeutic For Amblyopia - HTTPSWWW - Aaojournal.orgarticles0161-6420 (21) 00682-5fulltextDocument9 pagesRandomized Controlled Trial of A Dichoptic Digital Therapeutic For Amblyopia - HTTPSWWW - Aaojournal.orgarticles0161-6420 (21) 00682-5fulltextRael Rodrigues Dos SantosNo ratings yet
- E187 FullDocument7 pagesE187 FullVisaraNo ratings yet
- Opab 314Document7 pagesOpab 314Sebastian SalvadorNo ratings yet
- Sedation in BronchosDocument13 pagesSedation in BronchosEfrainNo ratings yet
- Evaluation of The Efficacy of Dentin Hypersensitivity Treatments-A Systematic Review and Follow Up AnalysisDocument39 pagesEvaluation of The Efficacy of Dentin Hypersensitivity Treatments-A Systematic Review and Follow Up AnalysisNaoki MezarinaNo ratings yet
- Threat or Not Threat PDADocument4 pagesThreat or Not Threat PDAijaldo ajahNo ratings yet
- Anoplastia Percutanea 2022Document11 pagesAnoplastia Percutanea 2022Sandra Cárdenas HilasacaNo ratings yet
- 2022 Article 6597Document7 pages2022 Article 6597joelruizmaNo ratings yet
- Ranibizumab Versus Verteporfin Photodynamic Therapy in Asian Patients With Myopic Choroidal NeovascularizationDocument10 pagesRanibizumab Versus Verteporfin Photodynamic Therapy in Asian Patients With Myopic Choroidal Neovascularizationmeris dindaNo ratings yet
- BR J Ophthalmol 1999 Das 1050 5Document7 pagesBR J Ophthalmol 1999 Das 1050 5xoxotheNo ratings yet
- Mccambridge 2017Document13 pagesMccambridge 2017Ana ValladaresNo ratings yet
- Aijcr 2011 04 021Document6 pagesAijcr 2011 04 021ishu sNo ratings yet
- Nose To Brain DdsDocument5 pagesNose To Brain DdsSoma YasaswiNo ratings yet
- Apnea Del SueñoDocument8 pagesApnea Del SueñoDiego PinedaNo ratings yet
- Analysis of Therapeutic Methods For Treating Vocal Process GranulomasDocument7 pagesAnalysis of Therapeutic Methods For Treating Vocal Process GranulomasgabrielaNo ratings yet
- Cochlear Implantation Under Local Anesthesia and Conscious Sedation: An Italian ExperienceDocument6 pagesCochlear Implantation Under Local Anesthesia and Conscious Sedation: An Italian ExperiencePritam PanigrahiNo ratings yet
- Aair 11 482 PDFDocument16 pagesAair 11 482 PDFRegina Dwindarti DarostyNo ratings yet
- Miller Trailblazer 280 NT ManualDocument50 pagesMiller Trailblazer 280 NT ManualGary Condict67% (3)
- What Is Related To Towns' Prospering and Decaying in Pennsylvania?Document8 pagesWhat Is Related To Towns' Prospering and Decaying in Pennsylvania?IEREKPRESSNo ratings yet
- 02 CY 2023 Query of PDMPDocument3 pages02 CY 2023 Query of PDMPPartha Sarathi DasNo ratings yet
- Group 3 ThesisDocument19 pagesGroup 3 ThesisSVPS100% (1)
- The Endocrine Pancreas: Regulation of Carbohydrate MetabolismDocument61 pagesThe Endocrine Pancreas: Regulation of Carbohydrate MetabolismNona AsolaNo ratings yet
- Gestational DiabetesDocument15 pagesGestational DiabetesAbdulJabar RiadhNo ratings yet
- How The First Nine Months Shape The Rest of Your LifeDocument3 pagesHow The First Nine Months Shape The Rest of Your Lifedonny pangilinanNo ratings yet
- Personality List of Discussion Topics ForDocument3 pagesPersonality List of Discussion Topics ForAbba JoyNo ratings yet
- Teacher-Made-Test BEVDocument3 pagesTeacher-Made-Test BEVMaureen Madriaga100% (1)
- A Clinician's Guide To Gender-Affirming Care Working With Transgender and Gender Nonconforming Clients by Sand C. Chang PHD 2018 PDFDocument314 pagesA Clinician's Guide To Gender-Affirming Care Working With Transgender and Gender Nonconforming Clients by Sand C. Chang PHD 2018 PDFmaquis87100% (6)
- Blantyre Coma ScaleDocument2 pagesBlantyre Coma ScaleBasant karn100% (6)
- RA11650Document22 pagesRA11650Ardeth Quiro NimenzoNo ratings yet
- 115 Cultural Safety Module and Self-Evaluation Assignment 2020 1Document8 pages115 Cultural Safety Module and Self-Evaluation Assignment 2020 1api-651972035No ratings yet
- Safety Data Sheet: Delo 400 LE SAE 15W-40Document8 pagesSafety Data Sheet: Delo 400 LE SAE 15W-40PavelNo ratings yet
- Client Counselling Problem 2020 (Team 047 N 048)Document2 pagesClient Counselling Problem 2020 (Team 047 N 048)Anay MehrotraNo ratings yet
- Kuliah 9 - Microorganisms As Xenobiotics Degraders - Ekologi Mikroorganisme 2020 - Ver1 Aoe PDFDocument36 pagesKuliah 9 - Microorganisms As Xenobiotics Degraders - Ekologi Mikroorganisme 2020 - Ver1 Aoe PDFizhamil hidayahNo ratings yet
- Upk Paket BDocument4 pagesUpk Paket BErla OktavianiNo ratings yet
- PICO Defining The Research QuestionDocument3 pagesPICO Defining The Research QuestionJuan MendozaNo ratings yet
- Content of The Dossier For Chemical Purity and Microbiological Quality, PA - PH - CEP (04) 1, 6R, December 2018Document16 pagesContent of The Dossier For Chemical Purity and Microbiological Quality, PA - PH - CEP (04) 1, 6R, December 2018Srinivasreddy ChallaNo ratings yet
- Minimal Beauty by Madeleine OliviaDocument47 pagesMinimal Beauty by Madeleine OliviaLucy May BarkerNo ratings yet
- Msds AntracolDocument9 pagesMsds AntracolLidya Nathalia Patandung100% (1)
- Calorimetría Indirecta EsencialDocument12 pagesCalorimetría Indirecta EsencialPaulina ToledoNo ratings yet
- Kelompok 1Document22 pagesKelompok 1teguhNo ratings yet
- Ascitic Fluid AnalysisDocument3 pagesAscitic Fluid AnalysisLohJNo ratings yet
- Policy 1 FIP PA LOL Flying 2022Document19 pagesPolicy 1 FIP PA LOL Flying 2022Mohammmad ArifNo ratings yet
- The Problem and The BackgroundDocument6 pagesThe Problem and The BackgroundMike jeron martinezNo ratings yet
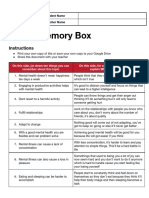
- Mental Health Memory BoxDocument2 pagesMental Health Memory Boxapi-551290426No ratings yet
- Risk Academy Free SlidesDocument20 pagesRisk Academy Free SlidesSrinath RNo ratings yet
- NCP New FormatDocument16 pagesNCP New FormatSophia Marie SoledadNo ratings yet
- Chapter 9 Notes Class 11Document5 pagesChapter 9 Notes Class 11Rachit KumarNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (29)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (5)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (27)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (59)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (45)