You might also like
- Life Process - Shobhit NirwanDocument36 pagesLife Process - Shobhit NirwanBhaskar 8287100% (2)
- 3f Aubf Lec Renal Function Tests PDFDocument11 pages3f Aubf Lec Renal Function Tests PDFBanana QNo ratings yet
- Disorders of Potassium: Dr. YabarowDocument43 pagesDisorders of Potassium: Dr. YabarowCabdiladif Ahmed McrfNo ratings yet
- Guyton & Hall Physio: Chapter 26 Urine Formation by The KidneysDocument66 pagesGuyton & Hall Physio: Chapter 26 Urine Formation by The KidneysMedSchoolStuff90% (21)
- HyperkalemiaDocument30 pagesHyperkalemiaAyanna100% (3)
- Benign Prostatic HyperplasiaDocument9 pagesBenign Prostatic HyperplasiaElizabeth Mapa100% (1)
- Fluid and Electrolyte ImbalanceDocument123 pagesFluid and Electrolyte ImbalanceBrealaiNo ratings yet
- MCQs in Fluid and Electrolyte Balance With AnswersDocument50 pagesMCQs in Fluid and Electrolyte Balance With Answersdrrajendrans80% (5)
- Pex 09 05Document4 pagesPex 09 05Pierre Rodriguez100% (7)
- Isosmotic Volume ContractionDocument9 pagesIsosmotic Volume ContractionFlower100% (1)
- 30 GuytonDocument7 pages30 GuytonBianca Louise Chan LimNo ratings yet
- Emergencies in Nephrology:: ObjectivesDocument9 pagesEmergencies in Nephrology:: ObjectivesAndy F MonroeNo ratings yet
- Chapter 37 Berne and LevyDocument4 pagesChapter 37 Berne and LevyJoezelleNo ratings yet
- Disorder of Potassium MetabolismDocument28 pagesDisorder of Potassium MetabolismSaif AliNo ratings yet
- Elektrolit DisorderDocument2,743 pagesElektrolit DisordervioletaNo ratings yet
- HyponatremiaDocument1 pageHyponatremiaLouay KilaNo ratings yet
- Potassium Homeostasis & DisordersDocument20 pagesPotassium Homeostasis & DisordersHassan SalamehNo ratings yet
- Genetic HypokalemiaDocument13 pagesGenetic HypokalemiabentoeNo ratings yet
- Dangerous Rhythms Tachycardia: Potassium Electrolyte HypokalemiaDocument7 pagesDangerous Rhythms Tachycardia: Potassium Electrolyte HypokalemiagorodoeNo ratings yet
- Electrolytes: Dedykusuma@ugm - Ac.idDocument20 pagesElectrolytes: Dedykusuma@ugm - Ac.idRama DhistaNo ratings yet
- Physiology 1 Fluid ElectrolyteDocument38 pagesPhysiology 1 Fluid ElectrolyteHaziq KamardinNo ratings yet
- Calcium, Magnesium, and Potassium Homeostasis: OutlineDocument10 pagesCalcium, Magnesium, and Potassium Homeostasis: OutlineMigs MedinaNo ratings yet
- MCQs in Fluid and Electrolyte Balance With AnswersDocument50 pagesMCQs in Fluid and Electrolyte Balance With AnswersAbdulkadir Waliyy Musa100% (2)
- Fluid and ElectrolyteDocument57 pagesFluid and ElectrolyteYuliana LatifNo ratings yet
- Maintenance FluidDocument27 pagesMaintenance FluidganeshyaeNo ratings yet
- 4 ElectrolyteDocument30 pages4 ElectrolytePesan IslamNo ratings yet
- Differential Diagnosis of Hyperkalemia: An Update To A Complex ProblemDocument9 pagesDifferential Diagnosis of Hyperkalemia: An Update To A Complex ProblemMariana CabralNo ratings yet
- Zhao Mingyao: BMC - Zzu. 2006-2-12Document32 pagesZhao Mingyao: BMC - Zzu. 2006-2-12api-19916399No ratings yet
- Intranscellular Fluid Interstitial Fluid Transcellular FluidDocument19 pagesIntranscellular Fluid Interstitial Fluid Transcellular FluidCharish Dwayne Bautista PondalesNo ratings yet
- PATH ImmuneDocument7 pagesPATH ImmuneDavid DvoskineNo ratings yet
- Desordenes de PotsioDocument30 pagesDesordenes de PotsioMarcela HincapiéNo ratings yet
- Regulation of Potassium HomeostasisDocument11 pagesRegulation of Potassium HomeostasisJuanaNo ratings yet
- Potassium BalanceDocument13 pagesPotassium BalancePhysiology by Dr Raghuveer100% (1)
- Aldosterone Regulation of Sodium: Atrial Natriuretic Peptide ANPDocument4 pagesAldosterone Regulation of Sodium: Atrial Natriuretic Peptide ANPHanoof GhaziNo ratings yet
- Disorders of Potassium Metabolism PresentationDocument20 pagesDisorders of Potassium Metabolism PresentationSolomon Fallah Foa SandyNo ratings yet
- Fluid and ElectrolyteDocument57 pagesFluid and ElectrolyteJustin Ahorro-DionisioNo ratings yet
- Body FluidsDocument34 pagesBody Fluidsdkphyhd99fNo ratings yet
- Nefrologia 30 Dias Electrolitos3Document31 pagesNefrologia 30 Dias Electrolitos3JUAN ANDRES GUARDIAS GARZONNo ratings yet
- Cell Injury Part-2Document18 pagesCell Injury Part-2Saipulla SaibuNo ratings yet
- Management of Hyperkalemia: by Dr. Orbunde Precious Washima Unit PresentationDocument26 pagesManagement of Hyperkalemia: by Dr. Orbunde Precious Washima Unit PresentationPeter ImojeNo ratings yet
- DKA Anesthesia Management. DR M MagdyDocument9 pagesDKA Anesthesia Management. DR M MagdyHany ElbarougyNo ratings yet
- Fluids & Electrolytes: Nio Cruzada Noveno, RN, MAN, MSNDocument66 pagesFluids & Electrolytes: Nio Cruzada Noveno, RN, MAN, MSNapi-19824701No ratings yet
- Lo 2 Week 4 Fms 3Document19 pagesLo 2 Week 4 Fms 3stephaaNo ratings yet
- Fluids and Electrolytes: 2. Interstitial SpaceDocument13 pagesFluids and Electrolytes: 2. Interstitial Spacehahahahaaaaaaa100% (1)
- Kuliah Mineral 2015-2016Document20 pagesKuliah Mineral 2015-2016molenNo ratings yet
- Hyperkalemia: Michael Levin, D.O. Medical Resident PGY II P.C.O.MDocument22 pagesHyperkalemia: Michael Levin, D.O. Medical Resident PGY II P.C.O.MsuviacesoNo ratings yet
- Plasma K Is Around 4mmol, So Relatively That's Low. Na Is 140mmolDocument24 pagesPlasma K Is Around 4mmol, So Relatively That's Low. Na Is 140mmoljavibruinNo ratings yet
- B.9 Situation - Care of Client With Problems in Fluid & Electrolyte BalanceDocument9 pagesB.9 Situation - Care of Client With Problems in Fluid & Electrolyte BalanceSOLEIL LOUISE LACSON MARBASNo ratings yet
- Fluid and Electrolyte Imbalances Part 1Document34 pagesFluid and Electrolyte Imbalances Part 1Gabrielle Frances FernandezNo ratings yet
- Lecture #4Document3 pagesLecture #4yeeticusfinchlmaoNo ratings yet
- Potassium HomeostasisDocument47 pagesPotassium HomeostasisMayuresh ChaudhariNo ratings yet
- Potassium Disorders: Syeda Shaheera ZaidiDocument60 pagesPotassium Disorders: Syeda Shaheera ZaidiMohammad AliNo ratings yet
- WEEK 5 Management of Patients With Fluids and ElectrolytesDocument89 pagesWEEK 5 Management of Patients With Fluids and ElectrolytesErica P. ManlunasNo ratings yet
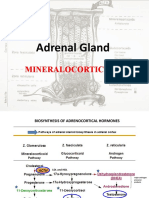
- Adrenal Gland by Dr. Rajnee IInd PartDocument30 pagesAdrenal Gland by Dr. Rajnee IInd Part9460106212No ratings yet
- FLE - Critical Thinking Questions - F & E AnswersDocument1 pageFLE - Critical Thinking Questions - F & E AnswersRich StrozewskiNo ratings yet
- HypokalemiaDocument1 pageHypokalemiaArif AlvaNo ratings yet
- Keseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicDocument79 pagesKeseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicdrroytambunanNo ratings yet
- Chapter30 PhysioDocument19 pagesChapter30 Physioناديه صاحبNo ratings yet
- Injuria Celular ReversibleDocument33 pagesInjuria Celular ReversibleCamila BuitragoNo ratings yet
- Chapter 27: Fluid and Electrolyte BalanceDocument26 pagesChapter 27: Fluid and Electrolyte BalanceMarwan M.No ratings yet
- MED - NE.1.18.Potassium Disorders (A2023)Document13 pagesMED - NE.1.18.Potassium Disorders (A2023)Ricky Justin NgoNo ratings yet
- 4 WaterDocument18 pages4 WaterJake RyanNo ratings yet
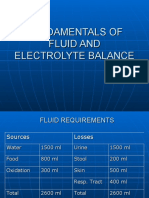
- Fundamentals of Fluid and Electrolyte BalanceDocument46 pagesFundamentals of Fluid and Electrolyte BalanceMelia Eka Rosita PharmacistNo ratings yet
- Fast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoFrom EverandFast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoNo ratings yet
- Fast Facts: Le déficit en pyruvate kinase pour les patients et les accompagnants: Une maladie génétique rare qui affecte les globules rouges Informations + Prise de contrôle = Meilleur résultatFrom EverandFast Facts: Le déficit en pyruvate kinase pour les patients et les accompagnants: Une maladie génétique rare qui affecte les globules rouges Informations + Prise de contrôle = Meilleur résultatNo ratings yet
- Diuretics 160418020107Document21 pagesDiuretics 160418020107P meruguNo ratings yet
- Multiple Choice Quiz - ExcretionDocument4 pagesMultiple Choice Quiz - ExcretionChantel AceveroNo ratings yet
- HomeostasisDocument18 pagesHomeostasisEmelia DeeNo ratings yet
- 1st Lecture On The Histology of Urinary System by DR RoomiDocument14 pages1st Lecture On The Histology of Urinary System by DR RoomiMudassar RoomiNo ratings yet
- Excretory Products and Their EliminationDocument6 pagesExcretory Products and Their EliminationHarshit AroraNo ratings yet
- Excretion Igcse BiologyDocument19 pagesExcretion Igcse BiologyJoshua ObayomiNo ratings yet
- CH 4-Absorption by Roots WORKSHEETDocument10 pagesCH 4-Absorption by Roots WORKSHEETFreya KotechaNo ratings yet
- Protein Uri ADocument2 pagesProtein Uri AAmelia PebriantiNo ratings yet
- Act 1 Urinary SystemDocument20 pagesAct 1 Urinary Systemisabellamarie.castillo.crsNo ratings yet
- OSMOREGULATIONDocument24 pagesOSMOREGULATIONGEETA MOHAN100% (3)
- Diuretics: Sumolly Anak DavidDocument29 pagesDiuretics: Sumolly Anak Davidfarmasi_hmNo ratings yet
- Sodium, Water and Potassium: Michael D. PenneyDocument39 pagesSodium, Water and Potassium: Michael D. PenneyChristianus LeonardNo ratings yet
- Life Processes 4Document18 pagesLife Processes 4Generic nameNo ratings yet
- List of AnticoagulantsDocument9 pagesList of Anticoagulantschristianz39100% (1)
- European J of Heart Fail - 2022 - Mullens - Renal Effects of Guideline Directed Medical Therapies in Heart Failure ADocument17 pagesEuropean J of Heart Fail - 2022 - Mullens - Renal Effects of Guideline Directed Medical Therapies in Heart Failure ALaura LizarazoNo ratings yet
- Acute Glomerulonephritis (AGN) : Universidad de ManilaDocument10 pagesAcute Glomerulonephritis (AGN) : Universidad de ManilaKristine_Bacan_2085No ratings yet
- Homeostasis and OsmoregulationDocument11 pagesHomeostasis and OsmoregulationMaria ChrisnaNo ratings yet
- Cloze Urinary SystemDocument2 pagesCloze Urinary SystemDarren AtwarooNo ratings yet
- AUBF Lec Renal Function I PDFDocument4 pagesAUBF Lec Renal Function I PDFBanana QNo ratings yet
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocument4 pagesPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNo ratings yet
- Group B - Sugar Solution 1 - Physio Ex - Exercise 9 - Activity 1Document4 pagesGroup B - Sugar Solution 1 - Physio Ex - Exercise 9 - Activity 1dktkaNo ratings yet
- Biology Quizs FNLDocument92 pagesBiology Quizs FNLAbdul WasayNo ratings yet
- Tubular Function (Distal Tubule)Document26 pagesTubular Function (Distal Tubule)Hakimah K. SuhaimiNo ratings yet
- BSC 6 Sem General Mammalian Physiology 2 Zoology Summer 2018Document1 pageBSC 6 Sem General Mammalian Physiology 2 Zoology Summer 2018Ujjwala KumbhalkarNo ratings yet
- Chapter FiveDocument155 pagesChapter Fivetadele10No ratings yet