You might also like
- Vein RomDocument4 pagesVein RomaksinuNo ratings yet
- 13f0 (1) - DikonversiDocument7 pages13f0 (1) - DikonversiAmyy NazmiNo ratings yet
- NURS4020 AshleyVigne Assessment2 Attemp1Document7 pagesNURS4020 AshleyVigne Assessment2 Attemp1ashleyNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument8 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- 42 PDFDocument5 pages42 PDFDaniela HernandezNo ratings yet
- Thu 2012Document5 pagesThu 2012Nadila Hermawan PutriNo ratings yet
- Dhanya Kerala 2021Document5 pagesDhanya Kerala 2021xyzNo ratings yet
- Incidence, Characteristics, and Predictive Factors For Medication Errors in Paediatric Anaesthesia: A Prospective Incident Monitoring StudyDocument8 pagesIncidence, Characteristics, and Predictive Factors For Medication Errors in Paediatric Anaesthesia: A Prospective Incident Monitoring StudyShaikh ZarinNo ratings yet
- Drug Errors: Consequences, Mechanisms, and Avoidance: Key PointsDocument7 pagesDrug Errors: Consequences, Mechanisms, and Avoidance: Key PointsRavikiran SuryanarayanamurthyNo ratings yet
- Imprtant Projects For Six Sigma HospitalDocument12 pagesImprtant Projects For Six Sigma Hospitalشادي الاخرسNo ratings yet
- Types of Medication Administration Errors and Comparisons Among NursingDocument7 pagesTypes of Medication Administration Errors and Comparisons Among NursingNadial uzmahNo ratings yet
- Kesalahan Obat Di Arab SaudiDocument8 pagesKesalahan Obat Di Arab SaudiEnggar Ardiani TagapNo ratings yet
- Observational Study of Safe Injection Practices in A Tertiary Care Teaching HospitalDocument5 pagesObservational Study of Safe Injection Practices in A Tertiary Care Teaching HospitalMuhammad HaezarNo ratings yet
- The Preparation and Administration of Intravenous Drugs Before and After Protocol ImplementationDocument8 pagesThe Preparation and Administration of Intravenous Drugs Before and After Protocol ImplementationIvanCompeanVazquezNo ratings yet
- Annals of Medicine and Surgery: Abraham Tarekegn Mersh, Debas Yaregal Melesse, Wubie Birlie ChekolDocument4 pagesAnnals of Medicine and Surgery: Abraham Tarekegn Mersh, Debas Yaregal Melesse, Wubie Birlie Chekoldwi sariNo ratings yet
- Medication Error Factors, Safety Guideline System, Flow of Drug Usage, and Code of Conduct To Prevent Medication ErrorDocument5 pagesMedication Error Factors, Safety Guideline System, Flow of Drug Usage, and Code of Conduct To Prevent Medication ErrorskyNo ratings yet
- Knowledge of Chemotherapy and Occupational Safety Measures Among Nurses in Oncology UnitsDocument7 pagesKnowledge of Chemotherapy and Occupational Safety Measures Among Nurses in Oncology UnitsIOM BNSNo ratings yet
- A Multicenter Point Prevalence Survey of Antibiotic Use in Haiti Juneaugust 2019 Findings and ImplicationsDocument2 pagesA Multicenter Point Prevalence Survey of Antibiotic Use in Haiti Juneaugust 2019 Findings and ImplicationsMentor Ali Ber LucienNo ratings yet
- 2018 - Wigiyantoro & DarmawanDocument11 pages2018 - Wigiyantoro & DarmawanazeemathmariyamNo ratings yet
- Evaluation of Drug Administration ErrorsDocument8 pagesEvaluation of Drug Administration ErrorsAchmad Indra AwaluddinNo ratings yet
- International Journal of Surgery Open: Mengesha Dessie AlleneDocument5 pagesInternational Journal of Surgery Open: Mengesha Dessie AllenebejarhasanNo ratings yet
- Drug use patterns at an orthopedic outpatient departmentDocument6 pagesDrug use patterns at an orthopedic outpatient departmentPromNo ratings yet
- Ebp 1Document4 pagesEbp 1sabitaNo ratings yet
- Pharmacy Education Article Page 107Document42 pagesPharmacy Education Article Page 107Cristine ChubiboNo ratings yet
- Irrational UseDocument8 pagesIrrational UseNilisha PradhanNo ratings yet
- Medicina 59 00713Document26 pagesMedicina 59 00713Ismaell LeitteNo ratings yet
- Anaesthesia - 2023 - Kinsella - Handling injectable medications in anaesthesiaDocument10 pagesAnaesthesia - 2023 - Kinsella - Handling injectable medications in anaesthesia177ervNo ratings yet
- A Prospective Study On Antibiotics-Associated Spontaneous Adverse Drug Reaction Monitoring and Reporting in A Tertiary Care HospitalDocument8 pagesA Prospective Study On Antibiotics-Associated Spontaneous Adverse Drug Reaction Monitoring and Reporting in A Tertiary Care HospitalNurul Hikmah12No ratings yet
- Beedemariam 2020.Document11 pagesBeedemariam 2020.Mart PerzNo ratings yet
- Antibiotic 02Document4 pagesAntibiotic 02Arslan ShahNo ratings yet
- Muzii Et Al., 2020Document9 pagesMuzii Et Al., 2020Jonathan LucisNo ratings yet
- ncc2021 1Document10 pagesncc2021 1api-519486875No ratings yet
- Point Prevalence Study of Antibiotics Use in Paediatric Wards of A Tertiary Health Facility in Kaduna NigeriaDocument8 pagesPoint Prevalence Study of Antibiotics Use in Paediatric Wards of A Tertiary Health Facility in Kaduna NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Antibiotic Use and Infection Rates in Periodontal Flap SurgeriesDocument7 pagesAntibiotic Use and Infection Rates in Periodontal Flap SurgeriesJoshua Diaz QuiquijanaNo ratings yet
- Roughead 2016Document10 pagesRoughead 2016Armando cortezNo ratings yet
- Worldviews Ev Based Nurs - 2009 - Demir - A Survey On Prevention of Surgical Infections in Operating TheatersDocument12 pagesWorldviews Ev Based Nurs - 2009 - Demir - A Survey On Prevention of Surgical Infections in Operating TheatersMelo Pérez Pamela J.No ratings yet
- Drug Utilization Study On Antibiotics Use in The Upper Respiratory Tract InfectionDocument4 pagesDrug Utilization Study On Antibiotics Use in The Upper Respiratory Tract InfectionNungki ArdilaNo ratings yet
- 395-Main Article-1737-1-10-20210603Document11 pages395-Main Article-1737-1-10-20210603فاتن محمدNo ratings yet
- Hewison NURSES IDENTIFICATION AND REPORTING OF MEDICATION ERRORS Journal Clinical NursingDocument17 pagesHewison NURSES IDENTIFICATION AND REPORTING OF MEDICATION ERRORS Journal Clinical NursingCatrin_HutaurukNo ratings yet
- Pharmacoepidemiology and Pharmacovigilance: Synergistic Tools to Better Investigate Drug SafetyFrom EverandPharmacoepidemiology and Pharmacovigilance: Synergistic Tools to Better Investigate Drug SafetyRating: 4.5 out of 5 stars4.5/5 (3)
- JurdingDocument9 pagesJurdingChristo LimbongNo ratings yet
- Drug Utilization Patterns Using Who Core Prescribing Indicators in Different Out Patient Departments at Secondary Care Hospital, KarimnagarDocument9 pagesDrug Utilization Patterns Using Who Core Prescribing Indicators in Different Out Patient Departments at Secondary Care Hospital, KarimnagarIJAR JOURNALNo ratings yet
- Pharmaco Epidemiology of Drugs Used in Post-CataraDocument5 pagesPharmaco Epidemiology of Drugs Used in Post-Catararirien refrina sariNo ratings yet
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- Inappropriateness in Laboratory Medicine An Elephant in The RoomDocument4 pagesInappropriateness in Laboratory Medicine An Elephant in The RoomomaromranNo ratings yet
- Toemj 5 25Document4 pagesToemj 5 25RPNo ratings yet
- Jcs 9 1Document8 pagesJcs 9 1kristina dewiNo ratings yet
- ISMP198 Periop Guidelns FINALDocument29 pagesISMP198 Periop Guidelns FINALHIRANGERNo ratings yet
- Medication ErrorsDocument7 pagesMedication ErrorsNelly CheptooNo ratings yet
- What Is The Epidemiology of MedicationDocument31 pagesWhat Is The Epidemiology of MedicationNadial uzmahNo ratings yet
- ContentServer - Asp 2Document13 pagesContentServer - Asp 2Nanda Nurdara TaharaNo ratings yet
- Prescription Completeness and Drug Use PatternDocument7 pagesPrescription Completeness and Drug Use Patternadane yehualawNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleFikri SatriaNo ratings yet
- Adverse Drug Reaction Monitoring DuringDocument7 pagesAdverse Drug Reaction Monitoring DuringmanguNo ratings yet
- Advanced Issue Resolution in Safety PharmacologyFrom EverandAdvanced Issue Resolution in Safety PharmacologyMary Jeanne KallmanNo ratings yet
- Incidence of Intravenous Drug Incompatibilities in Intensive Care UnitsDocument5 pagesIncidence of Intravenous Drug Incompatibilities in Intensive Care UnitsNeliydaMayantiNo ratings yet
- PDA Journal SeptemberDocument19 pagesPDA Journal SeptemberZia100% (1)
- 5390 20335 1 PBDocument4 pages5390 20335 1 PBSupun S WijekumaraNo ratings yet
- Schoten 2014Document9 pagesSchoten 2014abroud.amina.999No ratings yet
- Schwartz 2007Document8 pagesSchwartz 2007adriana Ortega CastilloNo ratings yet
- COVID 19 in Ecuador How The Pandemic Strained The 2020 International JournaDocument2 pagesCOVID 19 in Ecuador How The Pandemic Strained The 2020 International JournaYader Enrique Altamirano RamirezNo ratings yet
- Effectiveness of Bilateral Illioinguinal Illiohypogastric Ner - 2020 - InternatiDocument6 pagesEffectiveness of Bilateral Illioinguinal Illiohypogastric Ner - 2020 - InternatiYader Enrique Altamirano RamirezNo ratings yet
- International Journal of Surgery Open Editorial BoardDocument1 pageInternational Journal of Surgery Open Editorial BoardYader Enrique Altamirano RamirezNo ratings yet
- Corrigendum To Incidence and Factors Associated With Postoper - 2020 - InternatDocument1 pageCorrigendum To Incidence and Factors Associated With Postoper - 2020 - InternatYader Enrique Altamirano RamirezNo ratings yet
- E037737 FullDocument42 pagesE037737 FullYader Enrique Altamirano RamirezNo ratings yet
- Current Use of Neuromuscular Blocking Agents in Intensive Care UnitsDocument9 pagesCurrent Use of Neuromuscular Blocking Agents in Intensive Care UnitsYader Enrique Altamirano RamirezNo ratings yet
- Continuous Infusion Neuromuscular Blocking Agents (Nmbas) - Adult - Inpatient Clinical Practice GuidelineDocument24 pagesContinuous Infusion Neuromuscular Blocking Agents (Nmbas) - Adult - Inpatient Clinical Practice GuidelineYader Enrique Altamirano RamirezNo ratings yet
- Reversal of Neuromuscular Block: J.M. HunterDocument7 pagesReversal of Neuromuscular Block: J.M. HunterYader Enrique Altamirano RamirezNo ratings yet
- Neuromuscular Blocking Agents: PharmacologyDocument15 pagesNeuromuscular Blocking Agents: PharmacologyYader Enrique Altamirano RamirezNo ratings yet
- 1 s2.0 S240585722030067X MainDocument8 pages1 s2.0 S240585722030067X MainYader Enrique Altamirano RamirezNo ratings yet
- Pi Is 2058534921000172Document6 pagesPi Is 2058534921000172Yader Enrique Altamirano RamirezNo ratings yet
- Pharmacology of Neuromuscular Blocking DrugsDocument7 pagesPharmacology of Neuromuscular Blocking DrugsYader Enrique Altamirano RamirezNo ratings yet
- A Narrative Review On The Potential Benefits and Limitations of DeepDocument7 pagesA Narrative Review On The Potential Benefits and Limitations of DeepYader Enrique Altamirano RamirezNo ratings yet
- Bronchiolitis Obliterans PDFDocument7 pagesBronchiolitis Obliterans PDFSatnam KaurNo ratings yet
- Head Nursing ToolDocument26 pagesHead Nursing ToolJeneva L. LauzonNo ratings yet
- Care of A Bedridden Patient: Prepared by Jannet Reena PuraniDocument25 pagesCare of A Bedridden Patient: Prepared by Jannet Reena PuraniAnn Merlin Jobin100% (1)
- Case Study On Prostate CancerDocument16 pagesCase Study On Prostate Cancerferdz02100% (5)
- The Montgomery Borgatta Caregiver Burden ScaleDocument22 pagesThe Montgomery Borgatta Caregiver Burden ScalehjhjkNo ratings yet
- SorbitolDocument2 pagesSorbitolfara_1691100% (1)
- D-Dimer Antigen Current Concepts and Future Prospe-2Document40 pagesD-Dimer Antigen Current Concepts and Future Prospe-2fajar jamaloedinzNo ratings yet
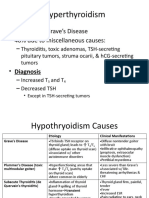
- Graves Disease and Hyperthyroidism Causes 60% of CasesDocument6 pagesGraves Disease and Hyperthyroidism Causes 60% of CasesLeitavia D.No ratings yet
- 3E - Agustin, Anne Julia - Group 1 - Case 7,8Document5 pages3E - Agustin, Anne Julia - Group 1 - Case 7,8Anne Julia AgustinNo ratings yet
- CVA Case ClerkingDocument11 pagesCVA Case ClerkingOtaiKatiNo ratings yet
- Professor Devendra Kumar Chhabra: TH THDocument2 pagesProfessor Devendra Kumar Chhabra: TH THVineet UttamNo ratings yet
- Reference RangesDocument8 pagesReference RangesKru PrimeNo ratings yet
- BSI MD Ivd Diagnostic Directive Guide Brochure UK enDocument8 pagesBSI MD Ivd Diagnostic Directive Guide Brochure UK enf.baxyNo ratings yet
- First Generation Anti-Depressants: TCAs and MAOIsDocument54 pagesFirst Generation Anti-Depressants: TCAs and MAOIssangha_mitra_2No ratings yet
- Fresenius 2008T Dialysis System - User's Troubleshooting ManualDocument20 pagesFresenius 2008T Dialysis System - User's Troubleshooting ManualCesar AlfaroNo ratings yet
- Case Study - Urinary Tract InfectionDocument10 pagesCase Study - Urinary Tract InfectionJiffy198867% (3)
- Book Eyelid Tumor)Document288 pagesBook Eyelid Tumor)evelyn100% (1)
- Low Back Pain Handbook. A Guide For The Practicing Clinician by Andrew J. Cole, M.D., F.a.C.S.M. and Stanley A. Herring, M.D., F.a.C.S.M. (Eds.)Document579 pagesLow Back Pain Handbook. A Guide For The Practicing Clinician by Andrew J. Cole, M.D., F.a.C.S.M. and Stanley A. Herring, M.D., F.a.C.S.M. (Eds.)David GermánNo ratings yet
- Patient Counseling FormDocument2 pagesPatient Counseling FormMarifuddin Hussaini50% (2)
- MCQ Pract Pharma 1Document9 pagesMCQ Pract Pharma 1Syamil AzharNo ratings yet
- Bovi-Shield Gold FP 5 VL5Document2 pagesBovi-Shield Gold FP 5 VL5טורו קוראזוןNo ratings yet
- Pengaruh Cognitive Behavioral Therapy (CBT) Terhadap Perubahan Kecemasan, Mekanisme Koping, Harga Diri Pada Pasien Gangguan Jiwa Dengan SkizofreniaDocument23 pagesPengaruh Cognitive Behavioral Therapy (CBT) Terhadap Perubahan Kecemasan, Mekanisme Koping, Harga Diri Pada Pasien Gangguan Jiwa Dengan Skizofreniaharyati soyNo ratings yet
- Monkeypox Contact Tracing Classification and Vaccination MatrixDocument2 pagesMonkeypox Contact Tracing Classification and Vaccination MatrixCemNo ratings yet
- CellulitisDocument16 pagesCellulitisMhOt AmAd100% (1)
- NURS 6521N Final Exam Question and Answers Feb 2020 (100/100)Document19 pagesNURS 6521N Final Exam Question and Answers Feb 2020 (100/100)Judy Durkin0% (1)
- Concept of Pregnancy Final NCM 107 07172019Document6 pagesConcept of Pregnancy Final NCM 107 07172019Jarod Hembrador100% (1)
- Prof J. Kasule, FRCS, FRCOG Department of Obstetrics and Gynaecology University of ZimbabweDocument17 pagesProf J. Kasule, FRCS, FRCOG Department of Obstetrics and Gynaecology University of ZimbabwedanielNo ratings yet
- Center For BrainHealthDocument5 pagesCenter For BrainHealthJames KuhnNo ratings yet
- IGCSE Excretion in Humans (Edited)Document59 pagesIGCSE Excretion in Humans (Edited)elizabethNo ratings yet
- American Journal of Emergency MedicineDocument7 pagesAmerican Journal of Emergency MedicineVirgi AgustiaNo ratings yet