You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- JRSHS Individual Team Technical Assistance PlanDocument7 pagesJRSHS Individual Team Technical Assistance PlanVictoria Beltran Subaran94% (16)
- An Instrument of Revival BABALOLADocument46 pagesAn Instrument of Revival BABALOLAGoriola David Gbolahan83% (6)
- Clsi Document c28 A2Document2 pagesClsi Document c28 A2Kristine Marie Pateño0% (1)
- Domain 1 Mock Test - Attempt ReviewDocument32 pagesDomain 1 Mock Test - Attempt ReviewPetRe Biong PamaNo ratings yet
- Ozark River Bank Cases: 20210821 - Case AnalysisDocument6 pagesOzark River Bank Cases: 20210821 - Case AnalysisTresna AswinNo ratings yet
- Disaster Risk Reduction Management Team Organizational Framework S.Y. 2021-2022Document1 pageDisaster Risk Reduction Management Team Organizational Framework S.Y. 2021-2022PetRe Biong PamaNo ratings yet
- Safety Assessment ToolsDocument3 pagesSafety Assessment ToolsPetRe Biong PamaNo ratings yet
- Schedule of Supervised Hand Washing and Disinfecting Activities Time DAY ActivityDocument1 pageSchedule of Supervised Hand Washing and Disinfecting Activities Time DAY ActivityPetRe Biong PamaNo ratings yet
- TEMPLATE A Teacheching and Non Teaching PersonnelDocument11 pagesTEMPLATE A Teacheching and Non Teaching PersonnelPetRe Biong PamaNo ratings yet
- Memo HOme VisitationDocument2 pagesMemo HOme VisitationPetRe Biong PamaNo ratings yet
- Guadalupe National High School: Class Program (F2F)Document5 pagesGuadalupe National High School: Class Program (F2F)PetRe Biong PamaNo ratings yet
- Annex C Parental Consent and Waiver FormDocument4 pagesAnnex C Parental Consent and Waiver FormMelodias VaughnNo ratings yet
- Guadalupe National High School: Class ProgramDocument3 pagesGuadalupe National High School: Class ProgramPetRe Biong PamaNo ratings yet
- DEPED DOH JMC No. 01 S. 2021Document27 pagesDEPED DOH JMC No. 01 S. 2021PetRe Biong PamaNo ratings yet
- Technical Assistance Plan AugustDocument1 pageTechnical Assistance Plan AugustRyan Bantiding100% (10)
- Guadalupe National High School: Class Program (F2F)Document4 pagesGuadalupe National High School: Class Program (F2F)PetRe Biong PamaNo ratings yet
- Guadalupe National High School: Class Program (F2F)Document4 pagesGuadalupe National High School: Class Program (F2F)PetRe Biong PamaNo ratings yet
- Pass Slip and LocatorDocument2 pagesPass Slip and LocatorPetRe Biong PamaNo ratings yet
- Annex C Parental Consent and Waiver FormDocument4 pagesAnnex C Parental Consent and Waiver FormMelodias VaughnNo ratings yet
- Insurance Commision Variable Insurance ContractsDocument11 pagesInsurance Commision Variable Insurance ContractsPetRe Biong PamaNo ratings yet
- Guadalupe National High School TeachingDocument16 pagesGuadalupe National High School TeachingPetRe Biong PamaNo ratings yet
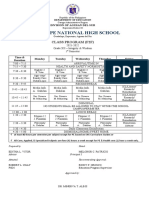
- CLASS PROGRAM G11 LevelDocument5 pagesCLASS PROGRAM G11 LevelPetRe Biong PamaNo ratings yet
- Domain 5 Mock Test - Attempt ReviewDocument26 pagesDomain 5 Mock Test - Attempt ReviewPetRe Biong Pama100% (1)
- Learners' Activity Sheets: Araling Panlipunan 10Document11 pagesLearners' Activity Sheets: Araling Panlipunan 10PetRe Biong PamaNo ratings yet
- Letter of Intent Enrichment ClassDocument10 pagesLetter of Intent Enrichment ClassPetRe Biong PamaNo ratings yet
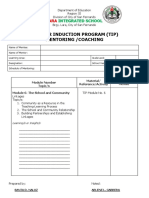
- Mentoring-Teachers - Technical-Assistance 2Document2 pagesMentoring-Teachers - Technical-Assistance 2Santa Dela Cruz NaluzNo ratings yet
- Domain 2 Mock Test - Attempt ReviewDocument28 pagesDomain 2 Mock Test - Attempt ReviewPetRe Biong PamaNo ratings yet
- LDM Form 2P - Supervisors - Practicum Portfolio Evaluation FormDocument140 pagesLDM Form 2P - Supervisors - Practicum Portfolio Evaluation FormPetRe Biong PamaNo ratings yet
- Domain 3 Mock Test Review: 44% ScoreDocument24 pagesDomain 3 Mock Test Review: 44% ScorePetRe Biong PamaNo ratings yet
- Domain 4 Mock Test - Attempt ReviewDocument22 pagesDomain 4 Mock Test - Attempt ReviewPetRe Biong PamaNo ratings yet
- (LDM 1 - 2-Supervisors) Guides On Practicum Portfolio-BuildingDocument7 pages(LDM 1 - 2-Supervisors) Guides On Practicum Portfolio-BuildingPetRe Biong PamaNo ratings yet
- LDM 2 Teachers Guides On Practicum Portfolio BuildingDocument8 pagesLDM 2 Teachers Guides On Practicum Portfolio BuildingNica Hernandez100% (1)
- DISGRACED Teacher S Pack.1 PDFDocument33 pagesDISGRACED Teacher S Pack.1 PDFSaad Imran δδNo ratings yet
- What We Can Learn From Japanese ManagementDocument14 pagesWhat We Can Learn From Japanese Managementsinan5858No ratings yet
- Meaning and Nature of MathematicsDocument3 pagesMeaning and Nature of MathematicsCyril KiranNo ratings yet
- Form: Contours and Areas V: Stefan ArteniDocument100 pagesForm: Contours and Areas V: Stefan Artenistefan arteniNo ratings yet
- Self DayaoskiiiDocument5 pagesSelf DayaoskiiiJoan Tabuena100% (1)
- Find The Thévenin Equivalent With Respect To The 7k Ohm ResistorDocument27 pagesFind The Thévenin Equivalent With Respect To The 7k Ohm ResistorVipan SharmaNo ratings yet
- De Onde Eu Te VejoDocument2 pagesDe Onde Eu Te VejoBianca Oliveira CoelhoNo ratings yet
- Just Say NO To Baby EinsteinDocument5 pagesJust Say NO To Baby Einsteinsmartypinto0% (1)
- Konsep Dasar Ilmu Biokimia Dan Biologi Molekuler Untuk Sistem SarafDocument31 pagesKonsep Dasar Ilmu Biokimia Dan Biologi Molekuler Untuk Sistem SarafdiandraNo ratings yet
- Pre Sequence Seq 1 2 3Document74 pagesPre Sequence Seq 1 2 3choaibirkiNo ratings yet
- Contemporary ArtDocument2 pagesContemporary ArtXpertz PrintingNo ratings yet
- Suretyship and Guaranty CasesDocument47 pagesSuretyship and Guaranty CasesFatima SladjannaNo ratings yet
- The Pen Pal ProjectDocument1 pageThe Pen Pal ProjectMelanie Yosiris Mayorga FonsecaNo ratings yet
- Ethics Final ModuleDocument27 pagesEthics Final ModuleEdmond TagubaNo ratings yet
- Tinea - The DermatophytesDocument67 pagesTinea - The Dermatophytesmansoor aliNo ratings yet
- Speaking Tasks 8 - B1+Document2 pagesSpeaking Tasks 8 - B1+Wayra EvelynNo ratings yet
- Hospital Visit ReportDocument8 pagesHospital Visit ReportSuraj JadhavNo ratings yet
- 9696 Geography Example Candidate Responses 2011 WEBDocument313 pages9696 Geography Example Candidate Responses 2011 WEBAsma Merchant67% (3)
- Measuring Speed of Light LabDocument5 pagesMeasuring Speed of Light LabTanzid SultanNo ratings yet
- Restrict Group Access in QV 9 Using ADDocument7 pagesRestrict Group Access in QV 9 Using ADBea BoocNo ratings yet
- Step-By-Step Guide to Praying the RosaryDocument3 pagesStep-By-Step Guide to Praying the Rosaryyeng0% (1)
- RitzeDocument4 pagesRitzeLalai IskolatongNo ratings yet
- 21st Century Literature Grade 11 21st Century Literature Grade 11 21st Century Literature Grade 11 CompressDocument75 pages21st Century Literature Grade 11 21st Century Literature Grade 11 21st Century Literature Grade 11 Compressdesly jane sianoNo ratings yet
- Elllo Mixer #99 Do You Enjoy CookingDocument2 pagesElllo Mixer #99 Do You Enjoy CookingEnrique GarciaNo ratings yet
- Freud BabaDocument11 pagesFreud Babapartha19881062No ratings yet
- A Literature Review On The Vehicle Routing Problem With Multiple Depepots PDFDocument15 pagesA Literature Review On The Vehicle Routing Problem With Multiple Depepots PDFcarandatruNo ratings yet
- Climate Resilient MaizeDocument12 pagesClimate Resilient MaizedonbosskissNo ratings yet