You might also like
- Complications Bariatric SurgeryDocument8 pagesComplications Bariatric SurgeryThita Orrego100% (1)
- Heart Failure Guide for NursesDocument54 pagesHeart Failure Guide for NursesKacelyn QuibanNo ratings yet
- Care of The Acutely Unwell FinalDocument100 pagesCare of The Acutely Unwell Finalgireeshsachin100% (1)
- HypertensionDocument5 pagesHypertensionCia Yee YeohNo ratings yet
- Danger Signs of PregnancyDocument3 pagesDanger Signs of PregnancyNesly Khyrozz LorenzoNo ratings yet
- Code Blue ManagemnetDocument36 pagesCode Blue ManagemnetPreethi BNo ratings yet
- Frequency Specific MicrocurrentDocument2 pagesFrequency Specific MicrocurrentAngela Pagliuso50% (2)
- GROUP 3 - CASE STUDY - TraumaDocument5 pagesGROUP 3 - CASE STUDY - TraumaDinarkram Rabreca EculNo ratings yet
- Case 8 NCP (Multiple Sclerosis)Document2 pagesCase 8 NCP (Multiple Sclerosis)je-ann catedralNo ratings yet
- JjjjokjhDocument4 pagesJjjjokjhWajiha Esmula TiuNo ratings yet
- Assess Patients HolisticallyDocument18 pagesAssess Patients HolisticallySavita Hanamsagar100% (1)
- Congestive Heart FailureDocument19 pagesCongestive Heart FailureIlavenil PanduranganNo ratings yet
- Head Injury Case StudyDocument10 pagesHead Injury Case StudyJayd Lorenz Vicente ChuanNo ratings yet
- Case StudyDocument34 pagesCase StudyBSNNursing101No ratings yet
- ChartingDocument41 pagesChartingArlene Saint AnthonieNo ratings yet
- Community Health Nursing Board ExamDocument15 pagesCommunity Health Nursing Board Examrhenier_ilado86% (14)
- Wender Utah PDFDocument3 pagesWender Utah PDFFco CanaleNo ratings yet
- ResumeDocument5 pagesResumeMal Di TaNo ratings yet
- Approach To Patient With Endocrine DisordersDocument2 pagesApproach To Patient With Endocrine DisordersSeff CausapinNo ratings yet
- Transitional Care Case Study-Pulling It All TogetherDocument13 pagesTransitional Care Case Study-Pulling It All TogethermatthewNo ratings yet
- Cardiac Tamponade and ManagementDocument42 pagesCardiac Tamponade and Managementأم حمدNo ratings yet
- VIOME+E-book Microbiom PDFDocument43 pagesVIOME+E-book Microbiom PDFNaša DjecaNo ratings yet
- By Dr. Nouran Abou Khedr: Xeroderma PigmentosumDocument6 pagesBy Dr. Nouran Abou Khedr: Xeroderma PigmentosumBahaa ShaabanNo ratings yet
- Vital Signs MeasurementDocument17 pagesVital Signs MeasurementEly TalledoNo ratings yet
- Case Study: Congestive Heart FailureDocument7 pagesCase Study: Congestive Heart FailureXI-E / 21 / MARY TRIANANo ratings yet
- NCP Acute Pain NCSDocument3 pagesNCP Acute Pain NCSPaolo Vittorio Perdigueros GonzalesNo ratings yet
- Acute BronchitisDocument38 pagesAcute BronchitisNikko MelencionNo ratings yet
- White Turqoise Creative Simple Medical Personnel Nurse ResumeDocument1 pageWhite Turqoise Creative Simple Medical Personnel Nurse ResumeRaymond EstrellaNo ratings yet
- Hypertension Case PresentationDocument32 pagesHypertension Case PresentationAnnaMaeGacutanMarantanNo ratings yet
- Nursing Assessment:: Intervention Rationale Independent InterventionsDocument2 pagesNursing Assessment:: Intervention Rationale Independent Interventionsnananana123No ratings yet
- Heart FailureDocument4 pagesHeart FailureDane WrightNo ratings yet
- Cardiac NSG DiagnosisDocument5 pagesCardiac NSG DiagnosisShreyas WalvekarNo ratings yet
- Standardized Toolbox for Pediac Surgery: Abdominal Masses of ChildhoodDocument30 pagesStandardized Toolbox for Pediac Surgery: Abdominal Masses of ChildhoodririlibertiNo ratings yet
- Administration of Inotropes Evidence Based Nursing PolicyDocument8 pagesAdministration of Inotropes Evidence Based Nursing PolicyRonald ThakorNo ratings yet
- Left-Sided Congestive Heart Failure Case PresentationDocument64 pagesLeft-Sided Congestive Heart Failure Case PresentationNicole Villanueva, BSN - Level 3ANo ratings yet
- Pericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerDocument2 pagesPericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerlhenNo ratings yet
- Pediatric Bronchitis Case PresentationDocument28 pagesPediatric Bronchitis Case PresentationJoshua DulayNo ratings yet
- Heart Failure and Hypertension CaseDocument2 pagesHeart Failure and Hypertension CasePaulo Arwin BaduriaNo ratings yet
- CASE STUDY FORMAT (Kidney Transplantation)Document12 pagesCASE STUDY FORMAT (Kidney Transplantation)ashnaNo ratings yet
- Congestive Heart FailureDocument14 pagesCongestive Heart FailureBella Trix PagdangananNo ratings yet
- Managing Respiratory Failure in Myasthenia Gravis and Guillain-Barré SyndromeDocument7 pagesManaging Respiratory Failure in Myasthenia Gravis and Guillain-Barré SyndromePutri Cindy Claudia PandoyoNo ratings yet
- Health Teachings On CHFDocument6 pagesHealth Teachings On CHFfLOR_ZIANE_MAENo ratings yet
- Generic Name Therapeutic Classification Pharmacologic ClassificationDocument3 pagesGeneric Name Therapeutic Classification Pharmacologic ClassificationAnselle CasilNo ratings yet
- MR Elamin ShockDocument70 pagesMR Elamin ShockMohammed Abd AlgadirNo ratings yet
- Assignmen 1 AnswersDocument3 pagesAssignmen 1 AnswersAlasl BobyNo ratings yet
- Case Presentation On Supraventricular TachycardiaDocument64 pagesCase Presentation On Supraventricular TachycardiaHazel AsperaNo ratings yet
- Nursing Process 3Document10 pagesNursing Process 3Shubhra Sheoran100% (1)
- NursingCare PlanDocument8 pagesNursingCare PlanSunSearra Kennedy RuffinNo ratings yet
- (Osborn) Chapter 56: Learning Outcomes (Number and Title)Document19 pages(Osborn) Chapter 56: Learning Outcomes (Number and Title)KittiesNo ratings yet
- Case Presentation OF Acute Tonsillitis: Nueva Ecija University of Science andDocument38 pagesCase Presentation OF Acute Tonsillitis: Nueva Ecija University of Science andBeverly DatuNo ratings yet
- Transurethral Resection of the Prostate (TURP) ExplainedDocument23 pagesTransurethral Resection of the Prostate (TURP) ExplainedColeen Comelle HuertoNo ratings yet
- Case Presentation IM DDHDocument12 pagesCase Presentation IM DDHAishwarya BharathNo ratings yet
- Nursing Management of Patient With Pericardial EffusionDocument2 pagesNursing Management of Patient With Pericardial EffusionAgung Alber0% (3)
- Nstemi: How To Risk Stratify?Document32 pagesNstemi: How To Risk Stratify?dhannibernadetNo ratings yet
- Anemia Anemia Describes The Condition in Which The Number of Red Blood Cells in The Blood Is Low. Probability & StatisticsDocument7 pagesAnemia Anemia Describes The Condition in Which The Number of Red Blood Cells in The Blood Is Low. Probability & StatisticsSahara GalayNo ratings yet
- Electrolyte ImbalanceDocument4 pagesElectrolyte ImbalanceDoneva Lyn MedinaNo ratings yet
- MARCOS - Legal Issues of ElderlyDocument2 pagesMARCOS - Legal Issues of ElderlyArian May MarcosNo ratings yet
- Acute Respiratory Distress SyndromDocument38 pagesAcute Respiratory Distress SyndrompatriaindraNo ratings yet
- Pathophysiology of ArrhythmiasDocument15 pagesPathophysiology of ArrhythmiasJonathan MontecilloNo ratings yet
- IV Fluid ChartDocument2 pagesIV Fluid Charthady920No ratings yet
- February 2024 OSHEMAC I Acceptance Letter and Registration FormDocument2 pagesFebruary 2024 OSHEMAC I Acceptance Letter and Registration FormadorabletwhindingwiNo ratings yet
- Types of Insulin PDFDocument3 pagesTypes of Insulin PDFRetno WulanNo ratings yet
- Patient DT STEMI CaseDocument18 pagesPatient DT STEMI CaseZNo ratings yet
- Hepatitis overview and nursing careDocument18 pagesHepatitis overview and nursing careAnne B. BuenvenidaNo ratings yet
- Intravenous Fluid Therapy: Types and UsesDocument11 pagesIntravenous Fluid Therapy: Types and UsesHayashi Breads MaaNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Healthcare Reflections, Insights, and Lessons: Proactive/ReactiveFrom EverandHealthcare Reflections, Insights, and Lessons: Proactive/ReactiveNo ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
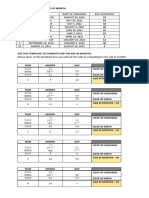
- Calculate Age Months TemplateDocument2 pagesCalculate Age Months TemplateJasmin T. RegaspiNo ratings yet
- Drug Study HeparinDocument2 pagesDrug Study HeparinJasmin T. RegaspiNo ratings yet
- Drug Study - FormatDocument2 pagesDrug Study - FormatJasmin T. RegaspiNo ratings yet
- Hypertension Nursing Care Plans: 6 Diagnoses & InterventionsDocument3 pagesHypertension Nursing Care Plans: 6 Diagnoses & InterventionsJasmin T. RegaspiNo ratings yet
- 2020 Breastfeeding WatermarkDocument83 pages2020 Breastfeeding WatermarkJasmin T. RegaspiNo ratings yet
- Data PersonilDocument74 pagesData Personilpanji_208No ratings yet
- Dengue Shock SyndromeDocument17 pagesDengue Shock SyndromehwelpNo ratings yet
- Kellett - Paranoid Personality Disorder Treatm.Document14 pagesKellett - Paranoid Personality Disorder Treatm.Caramel GazelleNo ratings yet
- DiethylcarbamazineDocument8 pagesDiethylcarbamazinePrakob GikokNo ratings yet
- What Are The Signs of Autism in GirlsDocument8 pagesWhat Are The Signs of Autism in GirlsAna Sofia Nunes JorgeNo ratings yet
- Health Insurance Guidelines 2020-21Document25 pagesHealth Insurance Guidelines 2020-21NIRAJ BAHEKARNo ratings yet
- Caliciviridae: A Family of Important Human and Animal VirusesDocument26 pagesCaliciviridae: A Family of Important Human and Animal VirusesabybrrNo ratings yet
- Quarter ApplicationDocument1 pageQuarter ApplicationSouvik DasNo ratings yet
- KRT Lucas Meliala, Guru Besar Luar Biasa Bagian Ilmu Penyakit SarafDocument43 pagesKRT Lucas Meliala, Guru Besar Luar Biasa Bagian Ilmu Penyakit SarafWawanHarimawanHardjowinotoNo ratings yet
- Hiv AidsDocument472 pagesHiv AidsDevendrapratapdpNo ratings yet
- The Montgomery Borgatta Caregiver Burden ScaleDocument22 pagesThe Montgomery Borgatta Caregiver Burden ScalehjhjkNo ratings yet
- Anorexia Nervosa PDFDocument6 pagesAnorexia Nervosa PDFmist73No ratings yet
- Metaplastic (Chronic) Atrophic Gastritis - UpToDate PDFDocument16 pagesMetaplastic (Chronic) Atrophic Gastritis - UpToDate PDFDinaNo ratings yet
- DRUG STUDY SpironolactoneDocument4 pagesDRUG STUDY SpironolactoneJerremy LuqueNo ratings yet
- Dust Work QuestionnaireDocument2 pagesDust Work QuestionnaireHykidNo ratings yet
- Pathophysiology of Congestive Heart Failure NarrativeDocument4 pagesPathophysiology of Congestive Heart Failure NarrativeAlfred BucabucaNo ratings yet
- Benha University Hospital, Egypt E-Mail: Elnashar53@Document58 pagesBenha University Hospital, Egypt E-Mail: Elnashar53@khadzx100% (3)
- Angiogenesis in CancerDocument4 pagesAngiogenesis in CanceranonymousNo ratings yet
- Acute pancreatitis symptoms, causes and diagnosisDocument12 pagesAcute pancreatitis symptoms, causes and diagnosisAmol DhopteNo ratings yet
- Fresenius 2008T Dialysis System - User's Troubleshooting ManualDocument20 pagesFresenius 2008T Dialysis System - User's Troubleshooting ManualCesar AlfaroNo ratings yet
- NAMA BARANG LIST AND PRICESDocument51 pagesNAMA BARANG LIST AND PRICESlevely rizkiNo ratings yet
- Cough NCPDocument2 pagesCough NCPMYLENE GRACE ELARCOSANo ratings yet