Professional Documents
Culture Documents
2022 - Efficacy and Safety of Intramuscular Administration of Tixagevimab-Cilgavimab For Early Outpatient Treatment of COVID-19 (TACKLE)
Uploaded by
rodrigo sacchiOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
2022 - Efficacy and Safety of Intramuscular Administration of Tixagevimab-Cilgavimab For Early Outpatient Treatment of COVID-19 (TACKLE)
Uploaded by
rodrigo sacchiCopyright:
Available Formats
Articles
Efficacy and safety of intramuscular administration of
tixagevimab–cilgavimab for early outpatient treatment of
COVID-19 (TACKLE): a phase 3, randomised, double-blind,
placebo-controlled trial
Hugh Montgomery, F D Richard Hobbs, Francisco Padilla, Douglas Arbetter, Alison Templeton, Seth Seegobin, Kenneth Kim,
Jesus Abraham Simón Campos, Rosalinda H Arends, Bryan H Brodek, Dennis Brooks, Pedro Garbes, Julieta Jimenez, Gavin C K W Koh,
Kelly W Padilla, Katie Streicher, Rolando M Viani, Vijay Alagappan, Menelas N Pangalos, Mark T Esser, on behalf of the TACKLE study group
Summary
Background Early intramuscular administration of SARS-CoV-2-neutralising monoclonal antibody combination, Lancet Respir Med 2022
tixagevimab–cilgavimab, to non-hospitalised adults with mild to moderate COVID-19 has potential to prevent disease Published Online
progression. We aimed to evaluate the safety and efficacy of tixagevimab–cilgavimab in preventing progression to June 7, 2022
https://doi.org/10.1016/
severe COVID-19 or death.
S2213-2600(22)00180-1
See Online/Comment
Methods TACKLE is an ongoing, phase 3, randomised, double-blind, placebo-controlled study conducted at 95 sites in https://doi.org/10.1016/
the USA, Latin America, Europe, and Japan. Eligible participants were non-hospitalised adults aged 18 years or older S2213-2600(22)00213-2
with a laboratory-confirmed SARS-CoV-2 infection (determined by RT-PCR or an antigen test) from any respiratory Department of Medicine,
tract specimen collected 3 days or less before enrolment and who had not received a COVID-19 vaccination. A University College London,
WHO Clinical Progression Scale score from more than 1 to less than 4 was required for inclusion and participants London, UK
(Prof H Montgomery MD);
had to receive the study drug 7 days or less from self-reported onset of mild to moderate COVID-19 symptoms or Nuffield Department of
measured fever. Participants were randomly assigned (1:1) to receive either a single tixagevimab–cilgavimab 600 mg Primary Care Health Sciences,
dose (two consecutive 3 mL intramuscular injections, one each of 300 mg tixagevimab and 300 mg cilgavimab) or University of Oxford, Oxford,
UK (Prof F D R Hobbs FMedSci);
placebo. Randomisation was stratified (using central blocked randomisation with randomly varying block sizes) by
Centro de Investigación en
time from symptom onset, and high-risk versus low-risk of progression to severe COVID-19. Participants, Cardiología y Metabolismo,
investigators, and sponsor staff involved in the treatment or clinical evaluation and monitoring of the participants Guadalajara, Jalisco, Mexico
were masked to treatment-group assignments. The primary endpoints were severe COVID-19 or death from any (F Padilla MD); Biometrics,
Vaccines and Immune
cause through to day 29, and safety. This study is registered with ClinicalTrials.gov, NCT04723394.
Therapies, BioPharmaceuticals
Research and Development,
Findings Between Jan 28, 2021, and July 22, 2021, 1014 participants were enrolled, of whom 910 were randomly AstraZeneca, Boston, MA, USA
assigned to a treatment group (456 to receive tixagevimab–cilgavimab and 454 to receive placebo). The mean age of (D Arbetter MPH); Biometrics,
Vaccines and Immune
participants was 46·1 years (SD 15·2). Severe COVID-19 or death occurred in 18 (4%) of 407 participants in the
Therapies (A Templeton PhD,
tixagevimab–cilgavimab group versus 37 (9%) of 415 participants in the placebo group (relative risk reduction 50·5% S Seegobin PhD), Clinical
[95% CI 14·6–71·3]; p=0·0096). The absolute risk reduction was 4·5% (95% CI 1·1–8·0; p<0·0001). Adverse events Pharmacology and Safety
occurred in 132 (29%) of 452 participants in the tixagevimab–cilgavimab group and 163 (36%) of 451 participants in Sciences
(R H Arends PhD*), Clinical
the placebo group, and were mostly of mild or moderate severity. There were three COVID-19-reported deaths in the
Development, Vaccines and
tixagevimab–cilgavimab group and six in the placebo group. Immune Therapies
(G C K W Koh PhD), and Vaccines
Interpretation A single intramuscular tixagevimab–cilgavimab dose provided statistically and clinically significant and Immune Therapies
(M N Pangalos PhD)
protection against progression to severe COVID-19 or death versus placebo in unvaccinated individuals and safety BioPharmaceuticals Research
was favourable. Treating mild to moderate COVID-19 earlier in the disease course with tixagevimab–cilgavimab and Development,
might lead to more favourable outcomes. AstraZeneca, Cambridge, UK;
ARK Clinical Research,
Long Beach, CA, USA
Funding AstraZeneca. (K Kim MD); Köhler & Milstein
Research/Hospital Agustín
Copyright © 2022 Published by Elsevier Ltd. All rights reserved. O’Horán, Mérida, Yucatán,
Mexico (J A S Campos MD);
Development Operations
Introduction variants emerge that might confer decreased vaccine (B H Brodek BSc), Patient
COVID-19 vaccines are effective at preventing symptomatic effectiveness.1,3,4 Safety, Chief Medical Office
and severe COVID-19;1 however, some populations remain SARS-CoV-2-neutralising monoclonal antibodies and (D Brooks MD), Clinical
at risk as SARS-CoV-2 continues to circulate.2 Older adults, antiviral therapies have been shown to be effective in Pharmacology and
Quantitative Pharmacology,
individuals with multiple comorbidities, and those who the treatment of non-hospitalised adults with COVID-19 Clinical Development, Vaccines
are immunocompromised are at risk of severe COVID-19 who are at high risk of progression to severe COVID-19 and Immune Therapies
outcomes from breakthrough infections, especially as new and death.5–9 Further evidence suggests that earlier (P Garbes MD, J Jimenez BSc,
www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1 1
Articles
R M Viani MD), Translational
Medicine, Vaccines and Research in context
Immune Therapies
(K Streicher PhD), Late-stage Evidence before this study with mild to moderate COVID-19 at high risk of progression
Development, Respiratory and Before the TACKLE study began (January, 2021), monoclonal to severe disease, who had not received a COVID-19 vaccine.
Immunology (V Alagappan MD), antibodies for the prevention and treatment of COVID-19 were Tixagevimab–cilgavimab is a long-acting antibody, with
and Vaccines and Immune
in early stages of development and, as a consequence, there longer half-life compared with other monoclonal antibodies
Therapies (M T Esser PhD),
BioPharmaceuticals Research were few published clinical trials. Since then, randomised, published so far. Tixagevimab–cilgavimab was the first
and Development, placebo-controlled, phase 3 clinical trials have been published monoclonal antibody combination to receive US Food and
AstraZeneca, Gaithersburg, for different monoclonal antibodies. A literature search of Drug Administration authorisation for use in COVID-19
MD, USA; Clinical
PubMed from date of inception to Jan 11, 2022, using the prevention, providing extended protection from a single
Development, Late-stage
Development, Vaccines and terms “SARS-CoV-2” or “COVID-19” and “monoclonal intramuscular dose. Other authorised anti-SARS-CoV-2
Immune Therapies, antibodies” or “mAbs” with the filters of “randomised monoclonal antibodies are indicated to be administered
BioPharmaceuticals Research controlled trial” and “clinical trial, phase 3”, and no language intravenously and subcutaneously. It is therefore of interest
and Development,
AstraZeneca, Durham, NC, USA
restrictions, identified 117 peer-reviewed publications related to evaluate the efficacy of intramuscular tixagevimab–
(K W Padilla PharmD) to the efficacy and safety of monoclonal antibodies in patients cilgavimab in treating mild to moderate COVID-19.
*Affiliation at time this work was with COVID-19. Of these, only five reported on use in the
Implications of all the available evidence
conducted outpatient treatment setting, and none reported on
The TACKLE results add to the growing evidence supporting
Correspondence to: monoclonal antibodies using an intramuscular route of
tixagevimab–cilgavimab use as treatment against SARS-CoV-2
Dr Mark Esser, Vaccines and administration.
Immune Therapies, in different settings and provide additional support beyond the
BioPharmaceuticals Research Added value of this study emergency use authorisation for prevention of COVID-19.
and Development, AstraZeneca, This study provides evidence of the efficacy and safety of a Further studies of tixagevimab–cilgavimab treatment are
Gaithersburg, MD, USA
mark.esser@astrazeneca.com
single 600 mg intramuscular dose of tixagevimab–cilgavimab needed among individuals who have received COVID-19
for the treatment of COVID-19 in non-hospitalised adults vaccination.
administration of SARS-CoV-2-neutralising monoclonal Methods
antibodies and antivirals leads to more favourable Study design
clinical outcomes.6,9 However, effectiveness of some TACKLE is an ongoing, phase 3, randomised, double-
SARS-CoV-2-neutralising monoclonal antibodies might blind, placebo-controlled, multicentre study. The trial is
be limited by the emergence of new SARS-CoV-2 being conducted at 95 sites in the USA, Latin America,
variants.8,10,11 Therefore, additional COVID-19 treatment Europe, and Japan. The proportion of hospital versus
See Online for appendix options are needed in populations at increased risk of non-hospital study sites is included in the appendix (p 7).
severe disease to mitigate the risk for severe outcomes The study was conducted in accordance with the Good
and reduce the burden on health-care systems, and in Clinical Practice guidelines and the Declaration of
preparation for the possible emergence of more malign Helsinki, Council for International Organizations of
variants of concern. Medical Sciences International Ethical guidelines,
Tixagevimab–cilgavimab (AZD7442, Catalent, applicable International Conference on Harmonisation
Bloomington, IN, USA) is a combination of two fully Good Clinical Practice guidelines, and all applicable laws
human, extended half-life SARS-CoV-2-neutralising and regulations. The protocol, protocol amendments, and
monoclonal antibodies that simultaneously bind to all other relevant documentation were reviewed and
distinct, non-overlapping epitopes of the viral spike approved by an institutional review board or ethics
protein receptor-binding domain.12 Tixagevimab– committee. The protocol (including amendments) and
cilgavimab has been shown to have neutralisation statistical analysis plan are in the appendix (pp 21–205).
activity in vitro against the original SARS-CoV-2 and
variants of concern.12 Tixagevimab–cilgavimab can be Participants
administered by intramuscular injection and has Eligible participants were non-hospitalised adults
received authorisation in various countries, including (definition of hospitalisation in the appendix p 9) aged
US Food and Drug Administration emergency use 18 years or older with a documented laboratory-confirmed
authorisation for the prevention of COVID-19 in SARS-CoV-2 infection, as determined by RT-PCR (testing
specific adults and children (aged 12 years and older for viral RNA) or an antigen test (testing for presence of
weighing at least 40 kg).13 SARS-CoV-2 proteins) from any respiratory tract
This ongoing phase 3 trial (TACKLE) aims to evaluate specimen collected 3 days or less before enrolment
the safety and efficacy of a single 600-mg intramuscular (day 1). A WHO Clinical Progression Scale score of more
dose of tixagevimab–cilgavimab for the treatment of than 1 to less than 4 (appendix p 15) was required for
COVID-19 in non-hospitalised adults (≥18 years) with inclusion. Participants had to receive study drug 7 days or
mild to moderate COVID-19 to prevent progression to less (inclusive; day 1 symptom count started from the first
severe COVID-19 or death. day of symptoms) from self-reported onset of mild to
2 www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1
Definition of being at high-risk of progression to severe COVID-19
••
Persons aged ≥65 years at randomisation.
Persons aged <65 years and having ≥1 of the following conditions:
– Cancer
– Chronic lung disease or moderate to severe asthma Articles
– Obesity (body mass index ≥30; may be based on self-report of recent height and weight measurement)
– Hypertension
– Cardiovascular disease (including history of smoke)
– Diabetes
– Chronic kidney disease
– Chronic liver disease
– Immunocompromised state from solid organ transplant, blood or bone marrow transplant, immune deficiencies, human
immunodeficiency virus, use of corticosteroids, or use of other immunosuppressive medicines
– Sickle cell disease
– Smoking (current or former)
moderate COVID-19 symptoms or measured fever. was distributed as an open-label product vial, and placebo
Peripheral saturation of arterial blood with oxygen was normal saline solution provided by the site. Both
(oxygen saturation) of 92% or more obtained at rest by were handled by an unmasked pharmacist at the study
study staff within 24 h before enrolment (day 1) was site who received a notification on what treatment to
required. Participants could not be involved in another assign for each participant. Syringe masking was done to
clinical trial for the treatment of COVID-19 or SARS-CoV-2 maintain masking.
during the study period until reaching hospitalisation or
28 days after study entry, whichever was earliest. Procedures
Participants were excluded if they had a history of On day 1, participants were given either tixagevimab–
hospitalisation or were currently hospitalised for cilgavimab as a single 600 mg dose (two consecutive
COVID-19, or if they had a current need for hospitalisation 3 mL intramuscular injections, one each of 300 mg
or immediate medical attention in a clinic or emergency tixagevimab and 300 mg cilgavimab) or saline placebo
room service in the clinical opinion of the site investigator. (0·9% NaCL; two consecutive 3 mL intramuscular
Due to local public health guidelines, some sites in Japan injections).
and Russia were required to hospitalise participants for The first 20 participants who received the study drug
isolation purposes upon testing positive for COVID-19; (approximately ten allocated to tixagevimab–cilgavimab
these participants were excluded from the primary and approximately ten allocated to placebo) formed
analysis, but were included in the full analysis set (all a sentinel group (randomly assigned 1:1 without
randomly assigned participants who received study drug) stratification) and underwent safety monitoring for 4 h
and the third supportive estimand of the primary analysis. post-dose and daily follow-up for the first 4 days after
Participants could be enrolled if the only reason for receiving the study drug. An independent Data Safety
hospitalisation related to a local policy-driven need for Monitoring Board reviewed safety data through to day 8
isolation. Participants were excluded if they had history of and provided a recommendation to continue or to halt
hypersensitivity, infusion-related reaction, or severe dosing of additional participants. The next 80 participants
adverse reaction following administration of a monoclonal received the study drug with safety monitoring for 2 h
antibody, or if they had previously received an post-dose. Subsequent participants received the study drug
investigational or licensed vaccine or other monoclonal with safety monitoring for 1 h post-dose. Further details on
antibody or biologic indicated for the prevention of study drug allocation, post-dose follow-up, and criteria for
SARS-CoV-2 or COVID-19 before study entry, or if study suspension are provided in the appendix (pp 11–12).
administration of these products was expected Participants will be monitored for safety purposes for
immediately after enrolment. Full inclusion and exclusion 456 days after receiving the study drug, to allow
criteria are provided in the appendix (pp 7–11). All assessment of safety over 5 half-lives for tixagevimab–
participants provided written informed consent. cilgavimab (approximately 450 days). The primary
analysis was conducted 30 days after approximately
Randomisation and masking 43 primary endpoint events had been observed, and
All participants were centrally randomly assigned (1:1) to additional analysis will be conducted after all participants
receive either tixagevimab–cilgavimab or placebo using have been followed up through to day 169. A final analysis
interactive response technology. Randomisation was will be conducted once all participants have completed
stratified (using central blocked randomisation) by time the study at day 457. The Data Safety Monitoring Board
from symptom onset (≤5 days vs >5 days), and high-risk will continue to monitor safety throughout the study.
versus low-risk of progression to severe COVID-19 Participants were recruited into one of two independent
(including those aged ≥65 years, immunocompromised cohorts: cohort 1 (approximately 300 participants) and
individuals, and those with comorbidities, such as cancer cohort 2 (up to approximately 1400 participants. Clinical
and chronic diseases). At least 60% of enrolled participants assessments included supplemental oxygen use recorded
were required to meet the protocol definition of being at at screening and at each in-person visit. Clinical
high risk. Full definition of individuals at high risk are assessment at in-person follow-up visits was done at days
included in the appendix (p 11). An external third-party 1, 3, 6, 15, 29, 85, 169, and 366 for cohort 1, and days 1, 6,
vendor (Signant Health; Blue Bell, PA, USA) was 29, 85, 169, and 366 for cohort 2. At study entry, if
responsible for creating and housing the randomisation peripheral oxygen saturation was less than 92% on usual
scheme. A method of randomly varying block sizes with supplemental oxygen requirements, the participant was
1:1 randomisation of treatment within each block of cells referred for emergency department evaluation and did not
was used. The participants, investigators, and sponsor receive the study drug, and after day 1 to day 29, peripheral
staff involved in the treatment or clinical evaluation and oxygen saturation measurements of less than 96% were
monitoring of the participants were masked to treatment- reviewed and referred for medical attention. Severe
group assignments. Masked study site staff could enrol COVID-19 was assessed for each participant.
participants. Study drug containers were not numbered For safety assessments, a complete physical exami-
before sending to the study sites; tixagevimab–cilgavimab nation was done at screening and at day 366. Adverse
www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1 3
Articles
events were reported by the participant; the investigator sequencing, mid-turbinate nasal swabs and plasma were
and any designees were responsible for detecting, collected on days 1, 3, 6, 15, and 29 for cohort 1 and days 1,
documenting, and recording events that met the 6, and 29 for cohort 2 for qualitative and quantitative
definition of an adverse event. Non-serious adverse SARS-CoV-2 RNA assessment.
events were collected from receipt of the study drug Clinical samples were screened for antidrug antibody
throughout the study, up to and including the last visit. assessment (at days 1, 29, 85, 169, 366, and optional at
Serious adverse events and adverse events of special day 457) against tixagevimab and cilgavimab separately
interest were (and will continue to be) recorded from the using an enhanced chemiluminescence solution-phase
time of signing of the informed consent form throughout bridging method. Samples were reported screen positive
the study, up to and including the last visit. for antidrug antibody in the screening assay if the mean
Full methods for complete physical examinations, enhanced chemiluminescence value was at or above the
virological, and antidrug antibody assessments are value of the plate-specific cut point factor.
provided in the appendix (pp 12–13). Targeted physical
examination was done at each in-person visit (days 1, 3, 6, Outcomes
15, 29, 85, and 169 for cohort 1, days 1, 6, 29, 85, and 169 The primary efficacy endpoint was a composite of either
for cohort 2). A complete physical examination was done severe COVID-19 or death from any cause through to
at day 366 and included, but was not limited to, day 29, with severe COVID-19 being defined as a
assessment of height, bodyweight, general appearance, minimum of either pneumonia (fever, cough, tachypnoea
head, ears, eyes, nose, throat, neck, skin, in addition to or dyspnoea, and lung infiltrates) or hypoxaemia (oxygen
cardiovascular, respiratory, abdominal, and nervous saturation <90% in room air, severe respiratory distress,
systems. For virological assessments including viral or both), plus a WHO Clinical Progression Scale score of
5 or more.14 The treating principal investigators were
responsible for determining whether participants met the
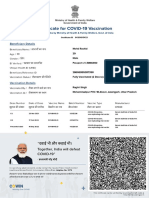
1014 participants enrolled* criteria of severe COVID-19 based on specific clinical
parameters. Each reported event was reviewed by the
104 not randomly assigned masked AstraZeneca Global Study Team to confirm the
82 screen failure principal investigator’s classification of a participant as
15 participant withdrawal
7 other
having severe COVID-19, as well as confirming participant
hospitalisations where severe COVID-19 was not reported.
Independent adjudication of these results was deemed
910 randomly assigned
unnecessary since misclassification of events was unlikely
based on the defined clinical criteria, the clinical
experience of the treating principal investigators, and
456 assigned to tixagevimab–cilgavimab 454 assigned to placebo masked oversight from the Global Study Team.
The primary safety endpoints were adverse events,
serious adverse events, and adverse events of special
4 did not receive treatment 3 did not receive treatment
interest throughout the study. Adverse events of special
interest included anaphylaxis and other serious
452 received tixagevimab–cilgavimab 451 received placebo hypersensitivity reactions, including immune complex
disease and injection site reactions.
16 participants withdrawn 19 participants withdrawn Secondary endpoints at day 29 included the incidence
from study from study of respiratory failure, levels of SARS-CoV-2 RNA in nasal
7 participant withdrawal 7 participant withdrawal swabs, and incidence of antidrug antibodies to
6 deaths 5 deaths†
2 lost to follow-up 2 lost to follow-up tixagevimab–cilgavimab in serum. Respiratory failure
1 physician decision 2 adverse event was defined as a requirement for mechanical ventilation,
3 other
extracorporeal membrane oxygenation, non-invasive
ventilation, or high-flow nasal cannula oxygen delivery.
452 included in full analysis set 451 included in full analysis set The key secondary endpoint was a composite of death
413 included in primary efficacy analysis 421 included in primary efficacy analysis from any cause or hospitalisation for COVID-19
(modified full analysis set)‡ (modified full analysis set)‡
452 included in primary safety analysis 451 included in primary safety analysis complications or sequalae to day 169. Other secondary
(safety analysis set) (safety analysis set) endpoints were whether tixagevimab–cilgavimab reduces
the progression of participant-reported COVID-19-
Figure 1: Trial profile associated symptoms to day 29, the differences in
*Informed consent received. †This differs from the initial number of deaths shown in table 3 because one death symptom duration between tixagevimab–cilgavimab and
occurred after the data cutoff, but the adverse event began before the data cutoff, thus the outcome was recorded.
This death is excluded from the figure because the record itself is after the data cutoff. ‡Participants excluded from placebo to day 29, and the single-dose pharmacokinetics
the primary analysis modified full analysis set comprised those hospitalised at baseline for isolation purposes of tixagevimab–cilgavimab. See appendix p 12 for full
(in Japan and Russia) or those randomly assigned after 7 days of symptom onset. details of secondary endpoints.
4 www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1
Articles
Exploratory endpoints included hospitalisation for any cause in the tixagevimab–cilgavimab group relative
COVID-19 disease or its complications through to to the placebo group.
day 29 (post hoc), and baseline and emergent viral The primary efficacy endpoint was calculated for the
resistance to tixagevimab–cilgavimab per viral genotypic modified full analysis set, which comprised all
analysis (prespecified). participants in the full analysis set (all randomly assigned
The study has a follow-up period of 457 days. Here, we participants who received study drug) who received study
report data from the primary data cutoff (Aug 21, 2021), drug 7 days or less from symptom onset and were not
at which time all ongoing study participants had hospitalised at baseline (up to and including day 1) for
completed at least 29 days of study follow-up. The key isolation purposes. Data collected following an
secondary endpoint of a composite of death from any intercurrent event (receipt of COVID-19 treatment
cause or hospitalisation for COVID-19 complications or product before day 29 without already having met the
sequalae to day 169 is not yet available and will be
analysed using a later data cutoff and reported
Tixagevimab– Placebo Total
elsewhere. Analyses of other secondary endpoints cilgavimab (n=451) (N=903)
including the progression of participant-reported (n=452)
COVID-19-associated symptoms and differences in Age, years 46·3 (15·4) 45·9 (15·0) 46·1 (15·2)
symptom duration will also be reported elsewhere. Age group, years
Analyses through to the end of the study (day 457) will ≥18 to <65 393 (87%) 394 (87%) 787 (87%)
be done after the final database lock after the last patient ≥65 to <75 38 (8%) 46 (10%) 84 (9%)
last visit.
≥75 21 (5%) 11 (2%) 32 (4%)
Sex
Statistical analysis
Female 239 (53%) 216 (48%) 455 (50%)
For the sample size, up to approximately 1700 participants
Male 213 (47%) 235 (52%) 448 (50%)
were planned to be randomly assigned to receive a single
Ethnicity
600-mg dose of tixagevimab–cilgavimab administered
Hispanic or Latino 230 (51%) 238 (53%) 468 (52%)
intramuscularly (up to approximately 850 participants)
Not Hispanic or Latino 222 (49%) 213 (47%) 435 (48%)
or placebo (up to approximately 850 participants).
Race
Enrolment was planned to stop once approximately
White 285 (63%) 274 (61%) 559 (62%)
43 primary events had been observed in the primary
American Indian or Alaska Native 100 (22%) 115 (26%) 215 (24%)
analysis population. This is an event-driven study with a
Asian 30 (7%) 21 (5%) 51 (6%)
primary analysis initiated 30 days after approximately
43 primary endpoints had been confirmed in the primary Black or African American 16 (4%) 20 (4%) 36 (4%)
analysis population. The study had 90% or more power Unknown, not reported, multiple, or missing data 21 (5%) 21 (5%) 42 (5%)
to detect a relative risk (RR) reduction of 65% in the Body-mass index, kg/m² 28·9 (5·5) 29·2 (6·6) 29·0 (6·0)
incidence of severe COVID-19 or death between the Time from symptom onset, days 4·9 (1·6) 5·0 (1·6) 5·0 (1·6)
study groups, based on the assumption that severe Serum for SARS-CoV-2 serology
COVID-19 or death in the placebo group would be 4·6%. Positive 60 (13%) 67 (15%) 127 (14%)
These assumptions reflected a protocol amendment Negative 384 (85%) 374 (83%) 758 (84%)
(version 7·0, July 5, 2021), following observed event rates Missing data 8 (2%) 10 (2%) 18 (2%)
of 4·6% to 5·8% in control groups from published At high risk of progression to severe COVID-19* 404 (89%) 405 (90%) 809 (90%)
studies.5,7 Accordingly, statistical power was reduced Risk factors for severe COVID-19
from 95% to 90% to accommodate the decrease in One or more risk factor 400 (89%) 399 (89%) 799 (89%)
expected event rate while maintaining a reasonable Obesity, body mass-index >30 kg/m² 195 (43%) 193 (43%) 388 (43%)
sample size and required number of events for analysis. Smoking 180 (40%) 184 (41%) 364 (40%)
Further details on protocol amendments, in addition to Hypertension 135 (30%) 121 (27%) 256 (28%)
protocol deviations, are provided in the appendix (p 7). Diabetes 53 (12%) 55 (12%) 108 (12%)
For the primary efficacy endpoint, the RR reduction in Chronic lung disease or asthma 58 (13%) 50 (11%) 108 (12%)
incidence of severe COVID-19 or death from any cause in Cardiovascular disease 42 (9%) 38 (8%) 80 (9%)
the tixagevimab–cilgavimab group relative to the placebo Cancer 18 (4%) 15 (3%) 33 (4%)
group was calculated using a Cochran-Mantel-Haenszel Chronic kidney disease 10 (2%) 9 (2%) 19 (2%)
(CMH) test. The primary efficacy endpoint was a binary Chronic liver disease 7 (2%) 13 (3%) 20 (2%)
response, and the CMH test was used to investigate Immunocompromised state 22 (5%) 23 (5%) 45 (5%)
treatment effect stratified by the two stratification factors
Data are mean (SD) or n (%). *High risk of progression defined as at least one risk factor, including age (≥65 years old)
at randomisation. Efficacy was estimated by the common or having at least one comorbidity (cancer, chronic lung disease, obesity, hypertension, cardiovascular disease,
RR or risk ratio from the CMH test. The RR diabetes, chronic kidney disease, chronic liver disease, immunocompromised state, sickle cell disease, or smoking).
reduction = 100 × (1 – RR) represented the percentage
Table 1: Participant demographics and baseline clinical characteristics in the full analysis set
reduction in incidence of severe COVID-19 or death from
www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1 5
Articles
Population Tixagevimab– Placebo RR reduction (95% CI) p value
cilgavimab
Primary efficacy endpoints and supportive estimands
Primary endpoint: severe COVID-19 Modified full analysis set* 18/407 (4%) 37/415 (9%) 50·5% (14·6–71·3) 0·0096
or death from any cause through to
day 29
First supportive estimand: severe Non-hospitalised participants who 9/253 (4%) 27/251 (11%) 66·9% (31·1–84·1) 0·0017
COVID-19 or death from any cause received study drug ≤5 days from
through to day 29 symptom onset (early intervention
analysis set)
Second supportive estimand: severe Modified full analysis set* 12/407 (3%) 33/415 (8%) 63·0% (29·4–80·6) 0·0015
COVID-19 or death from any cause
from day 4 through to day 29
Third supportive estimand: severe Full analysis set† 24/446 (5%) 41/444 (9%) 41·6% (5·0–64·1) 0·028
COVID-19 or death from any cause
through to day 29
Fourth supportive estimand: severe Non-hospitalised participants, who 14/347 (4%) 36/345 (10%) 61·3% (29·7–78·7) 0·0011
COVID-19 or death from any cause were seronegative at baseline and
through to day 29 received study drug ≤7 days from
symptom onset (seronegative
analysis set)
Secondary and exploratory endpoints
Secondary endpoint: prevention of Modified full analysis set 3/405 (1%) 11/412 (3%) 71·9% (0·3–92·1) 0·036
respiratory failure
Exploratory: hospitalisation for Modified full analysis set 17/413 (4%) 40/421 (10%) ·· ··
COVID-19 including complications
through to day 29
Data are n/N (%). RR=relative risk. Results from a Cochran-Mantel-Haenszel test stratified by time from symptom onset (≤5 days vs >5 days) and risk of progression to severe
COVID-19 (high risk vs low risk). RR reduction represents the percentage reduction in incidence of severe COVID-19 or death from any cause in the tixagevimab–cilgavimab
group relative to the placebo group. A RR reduction >0 represents favourable efficacy in the tixagevimab–cilgavimab group. For the primary outcome and supportive
estimands, p<0·05 indicates a statistically significant result; missing response data were not imputed. For the secondary outcome, p<0·05 indicates a nominally statistically
significant result, as this analysis was not included in the multiple testing hierarchy. *Six patients from each group had missing data and were not included in this analysis.
†Six patients in the tixagevimab–cilgavimab group and seven patients in the placebo group had missing data and were not included in this analysis.
Table 2: Primary efficacy endpoints and supportive analyses, and secondary efficacy endpoints
primary efficacy endpoint) were analysed using an analysis was done in participants in the modified full
intention-to-treat strategy, therefore, no censoring was analysis set who were seronegative for SARS-CoV-2 at
done for the intercurrent event. baseline.
To support the primary endpoint, Kaplan-Meier curves The primary endpoint and four supportive estimands
were used to summarise time to severe COVID-19 or were tested sequentially in a hierarchical order to control
death from any cause during the first 28 days post-dose for multiplicity; p values for secondary endpoint analyses
for each randomly assigned group. A stratified log-rank should be considered nominal. Analyses used for all
test was conducted to assess the difference between secondary endpoints reported in this manuscript and
groups. A Cox proportional hazards model was used to further information on the supportive estimands are
obtain a hazard ratio (HR) and respective 95% CIs, with shown in the appendix (pp 13–14). Secondary endpoints
the stratification factors included as covariates. with binary outcomes were analysed using CMH as in
Supportive analyses of the primary endpoint the primary efficacy analysis, and those with time-to-
(supportive estimands) were done using the same event outcomes were compared using Kaplan-Meier.
statistical methodology as described for the primary Viral load was analysed using a mixed model for repeated
efficacy endpoint. The first supportive estimand (early measures, for which the least squares mean differences
intervention) analysis included all participants in the were reported. The change from baseline of SARS-CoV-2
modified full analysis set who received dosing up to and RNA, and RNA levels at each treatment visit from nasal
including 5 days from symptom onset. The second swabs were summarised using descriptive statistics.
supportive estimand analysis was done in the modified The safety analysis was done in the safety analysis set,
full analysis set and only considered events occurring which included all participants who received the study
from day 4 through to day 29. The third supportive drug. Erroneously treated participants were analysed
estimand analysis was done in the full analysis set according to the treatment they actually received. No
(ie, including participants who might have been excluded statistical testing was done for the safety endpoints. SAS
from the primary analysis due to being hospitalised for (version 9.4) was used for all statistical analysis. This trial
isolation purposes). The fourth supportive estimand is registered with ClinicalTrials.gov, NCT04723394.
6 www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1
Articles
Role of the funding source older. 455 (50%) participants were female, 448 (50%) were
The funder of the study was responsible for manufacturing male, and 559 (62%) were White.
tixagevimab–cilgavimab, for designing the study, for In the primary efficacy analysis, severe COVID-19 or
acquiring, analysing, and interpreting the data, for death occurred in 18 (4%) of 407 participants in the
writing the report, and reviewing the manuscript. tixagevimab–cilgavimab group versus 37 (9%) of
415 participants in the placebo group (RR reduction 50·5%
Results [95% CI 14·6–71·3]; p=0·0096; table 2). Six participants
Between Jan 28, 2021, and July 22, 2021, 1014 participants from each group were not included in the primary
were enrolled, of whom 910 were randomly assigned to a analysis due to missing data (ie, 407 and 415 were
treatment group (456 to receive tixagevimab–cilgavimab included rather than 413 and 421). The absolute risk
and 454 to receive placebo). 413 participants in the reduction was 4·5% (95% CI 1·1–8·0; p<0·0001). The
tixagevimab–cilgavimab group and 421 in the placebo four supportive analyses of the primary efficacy endpoint
group were included in the modified full analysis set also showed significant reductions in the development of
(figure 1). 43 participants in the tixagevimab–cilgavimab severe COVID-19 or death with tixagevimab–cilgavimab
group and 33 in the placebo group were excluded from versus placebo (table 2).
the primary analysis because they were either hospitalised Kaplan-Meier probability of severe COVID-19 or death
at baseline for isolation purposes (in Japan and Russia), from any cause occurring up to day 29 is summarised in
or were randomly assigned after 7 days of symptom onset. figure 2A. The supplementary Cox Regression analysis
Median safety follow-up was 84·0 days (tixagevimab– showed a 51% reduction in the risk for severe COVID-19
cilgavimab IQR 31·0–86·0, placebo IQR 30·0–86·0) in or death from any cause for tixagevimab–cilgavimab
both treatment groups. versus placebo (figure 2A). Additional supportive
Baseline clinical characteristics were similar between analysis of the primary efficacy endpoint by time from
the groups (table 1). Mean age was 46·1 years (SD 15·2) symptom onset showed reduction in severe COVID-19
and 116 (13%) of 903 participants were aged 65 years or or death with tixagevimab–cilgavimab compared with
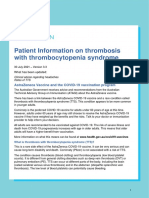
A
100 Treatment group
99
Probability of severe COVID-19 or death (%)
Tixagevimab–cilgavimab
98 Placebo
10 HR 0·49 (95% CI 0·28–0·86); p=0·010
9
8
7
6
5
4
3
2
1
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29
Time since receiving study drug (days)
Number at risk
Tixagevimab–cilgavimab 413 412 409 407 402 399 396 396 394 394 394 394 394 392 392 391 391 390 390 390 389 389 389 389 389 388 386 385 376 0
Placebo 421 420 417 415 410 403 391 389 386 383 381 381 381 381 380 379 379 379 379 378 378 378 377 377 377 376 375 370 365 0
B
Time from symptom Number of participants with event RR reduction (95% CI)
onset to random
assignment Tixagevimab– Placebo, n/N (%)
cilgavimab, n/N (%)
≤1 day 0/6 0/6 NE (NE)
≤2 days 0/29 3/34 (9%) 100% (NE)
≤3 days 1/90 (1%) 8/84 (10%) 88·0% (9·4–98·4)
≤4 days 4/172 (2%) 17/157 (11%) 78·4% (37·4–92·6)
≤5 days 9/253 (4%) 27/251 (11%) 66·9% (31·1–84·1)
≤6 days 11/329 (3%) 32/345 (9%) 64·1% (29·9–81·6)
≤7 days 18/407 (4%) 37/415 (9%) 50·5% (14·6–71·3)
0 20 40 60 80 100
Favours tixagevimab–cilgavimab
(Figure 2 continues on next page)
www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1 7
Articles
C
Number of participants with event RR reduction (95% CI)
Tixagevimab– Placebo, n/N (%)
cilgavimab, n/N (%)
Age
<65 years 10/359 (3%) 29/364 (8%) 65·1% (29·6 to 82·7)
≥65 years 8/48 (17%) 8/51 (16%) –6·9% (–159·9 to 56·0)
<75 years 12/389 (3%) 35/405 (9%) 64·3% (32·3 to 81·2)
≥75 years 6/18 (33%) 2/10 (20%) –49·0% (–424·9 to 57·7)
<80 years 15/398 (4%) 36/410 (9%) 57·2% (23·2 to 76·2)
≥80 years 3/9 (33%) 1/5 (20%) NE (NE)
Sex
Figure 2: Analysis of the
composite primary endpoint Male 10/186 (5%) 21/211 (10%) 44·9% (–12·8 to 73·1)
of severe COVID-19 or death Female 8/221 (4%) 16/204 (8%) 52·9% (–7·5 to 79·4)
from any cause up to day 29 Race
after receiving study drug American Indian or Alaskan Native 2/97 (2%) 14/113 (12%) 84·3% (25·0 to 96·7)
(A) Kaplan-Meier plot of time Asian 0/10 1/9 (11%) NE (NE)
to severe COVID-19 or death
Black or African American 0/15 1/19 (5%) 100 (NE)
from any cause through to
day 29 in the modified full Hawaiian or other Pacific Islanders 0/0 0/0 NE (NE)
analysis set. p value is based on White 15/265 (6%) 18/253 (7%) 19·4% (–55·7 to 58·3)
log-rank test stratified by time Other 0/0 0/0 NE (NE)
from symptom onset (≤5 days Ethnicity
vs >5 days), when applicable, Hispanic or Latino 8/218 (4%) 25/230 (11%) 66·5% (26·0 to 84·9)
and risk of progression to
Not Hispanic or Latino 10/189 (5%) 12/185 (7%) 18·7% (–81·0 to 63·5)
severe COVID-19 (high risk vs
low risk). Total number of Region
patients censored: USA 2/62 (3%) 2/36 (6%) 30·3% (–359·7 to 89·4)
tixagevimab–cilgavimab group Europe 11/173 (6%) 11/175 (6%) –3·5% (–129·0 to 53·2)
n=389, placebo group n=378. Latin America 5/166 (3%) 24/201 (12%) 74·5% (32·8 to 90·3)
(B) Forest plot of RR reduction Asia 0/6 0/3 NE (NE)
estimates for severe COVID-19
Risk group
or death from any cause
High 17/364 (5%) 33/371 (9%) 47·5% (7·5 to 70·2)
through to day 29 by time from
symptom onset at random Low 1/43 (2%) 4/44 (9%) 75·4% (–115·1 to 97·2)
assignment. Day 1 symptom COVID-19 comorbidity
count started from the first day ≥1 15/360 (4%) 33/365 (9%) 53·9% (16·6 to 74·5)
of symptoms. RR reductions 0 3/47 (6%) 4/50 (8%) 21·0% (–209·4 to 79·8)
represent the percentage
Baseline vitamin D
reduction in incidence of severe
<30 ng/mL 15/270 (6%) 25/276 (9%) 39·5% (–12·8 to 67·6)
COVID-19 or death from any
cause in the tixagevimab– ≥30 ng/mL 2/72 (3%) 3/74 (4%) 32·1% (–270·0 to 87·5)
cilgavimab group relative to Baseline zinc
placebo. A RR reduction >0 <100 µg/dL 15/301 (5%) 26/296 (9%) 44·1% (–4·3 to 70·0)
represents favourable efficacy ≥100 µg/dL 2/33 (6%) 2/38 (5%) 19·1% (–427·8 to 87·6)
in the tixagevimab–cilgavimab
Standard of care
group. (C) Forest plot of RR
Antiviral 0/0 0/0 NE (NE)
reduction estimates for severe
COVID-19 or death from any Antiviral, not active against COVID-19 2/15 (13%) 0/12 NE (NE)
cause through to day 29 by Antibiotic 2/24 (8%) 5/32 (16%) 65·5% (–99·6 to 94·0)
participant subgroup in the Immune–based 2/7 (29%) 0/3 NE (NE)
modified full analysis set. Corticosteroids 1/11 (9%) 1/14 (7%) –18·2% (–2988·5 to 95·5)
Arrows denote 95% CI bounds
Adjunctive 8/183 (4%) 23/206 (11%) 61·2% (14·4 to 82·4)
that are lower than the scale
Other 1/36 (3%) 0/42 NE (NE)
shown. Results in panel C were
from a Cochran-Mantel- None 7/209 (3%) 13/189 (7%) 49·0% (–25·1 to 79·2)
Haenszel test with stratification Baseline serum SARS-CoV-2 antibody
factors used in the primary Positive 4/52 (8%) 1/62 (2%) –436·2% (–5515·2 to 48·8)
analysis. For the subgroups of Negative 14/347 (4%) 36/345 (10%) 61·3% (29·7 to 78·7)
age, risk of progression was not
a stratification factor. If there
–450 –400 –350 –300 –250 –200 –150 –100 –50 0 50 100
was no stratification factor, a
χ² test was used. HR=hazard Favours placebo Favours tixagevimab–cilgavimab
ratio. NE=not evaluable. RR reduction (%)
RR=relative risk.
8 www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1
Articles
placebo in the 7 days after symptom onset. The greatest
Tixagevimab– Placebo
reductions in development of severe COVID-19 or death cilgavimab (n=451)
were observed when tixagevimab–cilgavimab was (n=452)
administered as early as possible after symptom onset, Any adverse event* 132 (29%) 163 (36%)
as shown by the RR reductions at 3 days or less Mild 67 (15%) 65 (14%)
(prespecified subgroup), 5 days or less and, at 7 days or Moderate 34 (8%) 50 (11%)
less (prespecified subgroup) from symptom onset Severe 22 (5%) 30 (7%)
(figure 2B). Total deaths 6 (1%) 6 (1%)†
For most participant subgroups, reductions in the Acute myocardial infarction or acute left ventricular failure 1 (<1%) 0
risk of developing severe COVID-19 or death with
Sudden cardiac death 1 (<1%) 0
tixagevimab–cilgavimab were consistent with the
COVID-19 pneumonia with outcome of death 2 (<1%) 4 (1%)
primary analysis (figure 2C). Most events were observed
COVID-19 with outcome of death 1 (<1%) 1 (<1%)
in participants at high risk of progression to severe
COVID-19 pneumonia, superinfection bacterial, or septic shock 0 1 (<1)
COVID-19 (figure 2C). Although the number of events
Malignant disease progression 1 (<1) 0
was low in participants at low risk of progression to
Any serious adverse event including death 33 (7%) 54 (12%)
severe COVID-19, a large but not statistically significant
Any treatment-related adverse event‡ 23 (5%) 21 (5%)
RR reduction with tixagevimab–cilgavimab was
Any adverse event leading to study withdrawal§ 5 (1%) 7 (2%)
observed in this group. There was a low proportion of
Common adverse events
seropositive participants, those aged 75 years or older,
COVID-19 pneumonia 26 (6%) 49 (11%)
and those on corticosteroids at baseline (table 1,
Headache 5 (1%) 2 (<1%)
figure 2C) and concomitantly a small number of events
in these subgroups, resulting in low RR reductions Any adverse event of special interest 15 (3%) 15 (3%)
with wide 95% CIs. Injection site pain 8 (2%) 10 (2%)
There was a significant reduction in respiratory failure Injection site erythema 2 (<1%) 2 (<1%)
in participants in the tixagevimab–cilgavimab group Injection site discomfort 2 (<1%) 1 (<1%)
compared with the placebo group (table 2). Injection site bruising 1 (<1%) 1 (<1%)
Antidrug antibody data were available in a subset of Injection site haematoma 1 (<1%) 1 (<1%)
participants up to 84 days after receiving the study drug. Injection site induration 1 (<1%) 0
Treatment-emergent antidrug antibodies to tixagevimab– Injection site inflammation 1 (<1%) 0
cilgavimab occurred in six (5%) of 134 participants, with Injection site nodule 1 (<1%) 0
a low median titre of 120, which was very close to the Injection site warmth 0 1 (<1%)
lower limit of quantification of the antidrug antibody *Each participant is counted only once (based on their maximum reported intensity) within a treatment group.
assay of 3·348 log10 copies per mL (2228 copies per mL). †This differs from the initial number of deaths shown in figure 1 because one death occurred after the data cutoff, but
Further details on the antidrug antibody assay are shown the adverse event began before the data cutoff, thus the outcome was recorded. This death is excluded from figure 1
because the record itself is after the data cutoff. ‡Possibly related, as assessed by the investigator. Includes adverse
in the appendix (p 13). events that occurred through to the end of the study. §Two participants in the placebo group discontinued from the
There was a greater reduction in viral shedding for study due to adverse events. Percentages are based on the total numbers of participants in the treatment group.
tixagevimab–cilgavimab versus placebo between baseline Participants with multiple events of the same preferred term are counted only once in that preferred term. Participants
with events in more than one preferred term within the same system organ class are counted only once in that system
and day 6 (appendix p 19), with mean change in log10 viral organ class row. Includes adverse events that occurred through to the end of the study. Adverse events of special
RNA from baseline to day 6 of –1·9 (95% CI –1·7 to –2·1) interest includes injection site reactions and anaphylaxis and other serious hypersensitivity reactions, including
in the tixagevimab–cilgavimab groups versus –1·5 immune complex disease. See details in protocol section 8·3·4 in the appendix (p 21).
(–1·3 to –1·7) in the placebo group. Table 3: Adverse events in the safety analysis set
Adverse events were reported by 132 (29%) of
452 participants in the tixagevimab–cilgavimab group
and 163 (36%) of 451 in the placebo group. The most In prespecified exploratory analysis, viral sequencing
common adverse event in both groups was COVID-19 in 413 tixagevimab–cilgavimab participants, and
pneumonia (table 3). Serious adverse events were 421 placebo participants, indicated that the alpha (B.1.1.7)
reported by 33 (7%) participants in the tixagevimab– SARS-CoV-2 variant was the most prevalent through to
cilgavimab group and 54 (12%) in the placebo group. day 29 (258 [60%] of 834 sequenced samples), followed by
The most common serious adverse event was COVID-19 gamma (P.1; 84 [20%]), delta (B.1.617.2; 66 [15%]), lambda
pneumonia (appendix p 18). Most adverse events (C.37; 20 [5%]), mu (B.1.621; two [1%]), and beta
were mild or moderate in severity (table 3). The (B.1.351; one [<1%]; appendix p 17).
most common adverse event of special interest was In the post-hoc exploratory analysis, fewer participants
injection site pain (table 3). Investigators reported were hospitalised for COVID-19 in the tixagevimab–
three (1%) COVID-19 deaths in the tixagevimab– cilgavimab group versus the placebo group across all
cilgavimab group compared with six (1%) in the placebo reported hospital settings (table 2; appendix p 16). Fewer
group; deaths due to any cause were reported for participants in the tixagevimab–cilgavimab group
six (1%) participants in each treatment group (table 3). compared with the placebo group were admitted to the
www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1 9
Articles
intensive care unit due to COVID-19, required admission Although other SARS-CoV-2-neutralising monoclonal
to an inpatient hospital setting, required acute hospital antibodies have shown effectiveness against COVID-19
care at home (acute hospital care at home occurred if in the treatment setting,5,6 the intramuscular admin-
physician determines condition is appropriate for acute istration of tixagevimab–cilgavimab might offer clinical
in-patient hospitalisation, and if patients were evaluated advantages, especially in outpatient and primary care
daily), or were admitted to the emergency department for settings. Tixagevimab–cilgavimab was specifically
longer than 24 h (appendix p 16). formulated for intramuscular administration, which
allows for early intervention and ease of access,
Discussion facilitating its use in the real world. The extended half-
Findings from the TACKLE study suggest that a single, life of 90 days of tixagevimab–cilgavimab (compared
intramuscular, 600 mg dose of tixagevimab–cilgavimab with the shorter half-lives of 18–32 days of other
was associated with statistically and clinically significant SARS-CoV-2-neutralising monoclonal antibodies24,25),
protection against the development of severe COVID-19 resulting from specific YTE genetic modifications (that
or death in non-hospitalised unvaccinated adults with result in Met252Tyr/Ser254Thr/Thr256Glu),12 could
mild to moderate COVID-19. Additional prespecified potentially also confer long-term protection against
analyses showed that earlier treatment with tixagevimab– symptomatic COVID-19, as shown in the PROVENT
cilgavimab led to more favourable outcomes (reduced study.23 Although antiviral therapies are effective in the
risk for progression to severe COVID-19 and death). treatment of COVID-19,8,9 multiple treatment options
Tixagevimab–cilgavimab had a favourable safety profile are needed in the armamentarium against COVID-19
and was well tolerated. due to the risk of resistance occurring against any
Treatments are needed for individuals who develop specific drug.26
SARS-CoV-2 breakthrough infections and are at high risk In addition to the YTE modifications, tixagevimab and
for severe disease, hospitalisation, and death, such as older cilgavimab also include triple amino acid modifications,
adults, those with multiple comorbidities, and individuals designed to reduce both Fc receptor interactions and the
with impaired immune systems.5,15–18 Additionally, cases of theoretical risk of antibody-enhanced disease. Indeed,
prolonged and unresolved SARS-CoV-2 infection have non-human primate studies of tixagevimab–cilgavimab
been reported in immunocompromised individuals, confirmed that the triple amino acid modification ablates
which might result in the emergence of new variants.19 all downstream Fc-effector functions (cellular responses
Furthermore, a substantial proportion of the global and complement cascade), with no effect on neutralisation
population remain unvaccinated20 and are at increased risk activity or clearance of SARS-CoV-2.12 This is supported by
of hospitalisation and mortality from COVID-19 compared the faster reductions in SARS-CoV-2 viral RNA from
with vaccinated individuals.18,21,22 This study showed a nasal swabs with tixagevimab–cilgavimab versus placebo
reduced risk of progression to severe COVID-19 or death shown in TACKLE.
with tixagevimab–cilgavimab in a population where The strengths of this study include a population with
approximately 90% of participants were at high risk of high prevalence of comorbidities considered to be risk
severe COVID-19, including older adults, those with factors for progression of COVID-19. The diversity of the
comorbidities such as hypertension, diabetes, chronic study population is shown by the large proportion of
lung disease, cardiovascular disease, and cancer, or Hispanic and American Indian and Alaska Native
individuals who were immunocompromised. As such, participants, reflecting the large contribution to the study
these data support the potential of tixagevimab–cilgavimab population from Latin America, including Mexico. These
to provide a new treatment option for individuals who data consistently showed that more hospitalisations
require protection from severe COVID-19 outcomes. occurred in the placebo group than the tixagevimab–
The incidence of adverse events was similar in the cilgavimab group, regardless of hospital setting (which
tixagevimab–cilgavimab and placebo groups, with most ranged from the emergency room to intensive care
being mild or moderate in severity. Specifically, the units), supporting tixagevimab–cilgavimab utility across
incidence of injection site pain was similar in both a variety of health-care settings.
groups. Although all-cause mortality was similar between The limitations of this study include a low proportion
the groups, there were fewer COVID-19-reported deaths of Black and African American and Asian participants,
in the tixagevimab–cilgavimab group than the placebo especially given the disproportionate effect of COVID-19
group. Overall, these safety results are consistent with among these populations.27 The study was also limited by
the phase 3 PROVENT and STORM CHASER trials of the exclusion of individuals previously vaccinated against
tixagevimab–cilgavimab.13,23 Safety monitoring for COVID-19, and the low number of immunocompromised
tixagevimab–cilgavimab will continue in the ongoing individuals and older adults. Although increased age is a
sponsor-funded TACKLE, PROVENT (NCT04625725), major risk factor for severe COVID-19, recruitment of
and STORM CHASER (NCT04625972) trials, as well as those older than 65 years was limited, mainly due to
the collaborative ACTIV-2 (NCT04518410), ACTIV-3 prioritisation of older adults for vaccination when the
(NCT04501978), and DisCoVeRy (NCT04315948) trials. study was enrolling. Due to these limited numbers of
10 www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1
Articles
participants, there was a small number of events for discussion of the manuscript, and the form of the presentation.
several findings, resulting in wide 95% CIs. Other RHA contributed to the dose selection, pharmacokinetics, and antidrug
antibody analyses. BHB contributed to project delivery and
limitations include the absence of formal and specific administration, and resources. DB contributed to the data analysis,
assessment for COVID-19 deaths beyond investigator interpretation, and study design. PG contributed to data analysis,
decision. The duration of available data limited interpretation, project administration, and supervision. JJ contributed to
interpretation of safety (median follow up 84·0 days) and the study design and data collection and quality. GCKWK contributed to
the review and agreement of the statistical analysis plan, the review of
some secondary endpoints. Although this study did not study results, and agreement on interpretation, including additional
measure T cells or assess antibody-dependent cellular analyses required and key conclusions. KWP was directly involved in
cytotoxicity, previous evidence suggests that antibodies data curation, investigation, methodology (of amendments), project
against tixagevimab–cilgavimab show little to no administration, and as the clinical scientist for TACKLE, directly
assessed and verified the quality of the data (in a masked fashion).
antibody-dependent cellular cytotoxicity activity.12 Efficacy KS contributed to the conceptualisation of the study, investigation,
against the omicron (B.1.1.529) SARS-CoV-2 variant and validation of the data. RMV was involved in the study design,
cannot be derived from this study given the study period collection and interpretation of data, and data checking of information.
reported; however, tixagevimab–cilgavimab has been VA contributed to the study design, study execution, data collection,
data analysis, and interpretation of the manuscript. MNP contributed to
shown to retain neutralising activity against omicron in study conceptualisation and design, data analysis and interpretation,
vitro. Despite reduction in neutralisation against the funding acquisition, project administration, and resourcing. MTE was
omicron BA.1 subvariant, the half maximal inhibitory involved in the study design, collection, analysis, and interpretation of
concentration values ranged from 51 to 277 ng/mL.10–12 data, as well as conceptualisation, formal analysis, methodology, project
administration, supervision, and data checking of information provided
Other SARS-CoV-2 neutralising monoclonal antibodies in the manuscript. Ultimate responsibility for opinions, conclusions,
have been shown to differ in neutralising abilities for and data interpretation lies with the authors. All authors were involved
variants of concern such as omicron.10,11 Further in-vitro in the drafting and critical revision of the manuscript. All authors
approved the final version of the manuscript and were responsible for
studies showed minimal loss of neutralising activity
the final decision to submit for publication.
against the (now dominant) omicron BA.2 subvariant
Declaration of interests
compared with wild-type SARS-CoV-2 (5-fold reduction
HM has received consultation fees from AstraZeneca and is supported
in live virus assays and 3-fold reduction in pseudovirus by the UK National Institute for Health Research’s Comprehensive
assays).28 Further evidence is expected from planned real- Biomedical Research Centre at University College London Hospitals.
world studies that will assess the effects of tixagevimab– He has consulted for Millfield Medical Ltd on the development of a new
continuous positive airway pressure machine. JASC reports serving on
cilgavimab with COVID-19 vaccination, including its use,
advisory boards for Pfizer and Eli Lilly; and serving on advisory boards
effectiveness, and acceptability in clinical practice, in and as a speaker for AstraZeneca and Roche. FDRH reports funding
immunocompromised individuals with breakthrough from AstraZeneca to cover meeting attendances and operationalisation
infections, and against omicron. of TACKLE in the UK as UK principal investigator. He has received
funding by UK Research and Innovation and National Institute for
To our knowledge, data from TACKLE are the first from Health and Care Research (NIHR) for national Urgent Public Health
an outpatient treatment study of a long-acting monoclonal COVID-19 trials, and as Director of the NIHR Applied Research
antibody combination with intramuscular administration Collaboration, Oxford Thames Valley, and investigator on the Oxford
for treating mild to moderate COVID-19. These results Biomedical Research Centre and NIHR MedTech. FP has received
personal fees and grants from Amgen, AstraZeneca, Boehringer
show that tixagevimab–cilgavimab provided statistically Ingelheim, Ferrer, Kowa, Medix, Merck, Merck Sharp and Dohme,
and clinically significant protection against the Novartis, Pfizer, Sanofi, Servier, and Silanes. KK has received research
development of severe COVID-19 or death in unvaccinated grants for the conduct of the TACKLE trial, reports funding from
individuals and was well tolerated. Tixagevimab– Regeneron, Eli Lilly, Merck, Pfizer, and Adagio, and serves as a speaker
for Regeneron. DA, AT, SS, RHA, BHB, DB, PG, JJ, GCKWK, KWP,
cilgavimab administered intramuscularly presents a RMV, KS, VA, MNP, and MTE are employees of, and hold or may hold
potential additional option for treating mild to moderate stock in, AstraZeneca.
COVID-19 in individuals at high risk, and contributes to Data sharing
the armamentarium against COVID-19, which is crucial Data underlying the findings described in this manuscript may be
for reducing the burden on health-care systems. requested in accordance with AstraZeneca’s data sharing policy
described at https://astrazenecagrouptrials.pharmacm.com/ST/
Contributors
Submission/Disclosure. AstraZeneca Group of Companies allows
All authors contributed to data interpretation, writing, and editing of the
researchers to submit a request to access anonymised participant-level
manuscript, and all reviewed and approved the manuscript for
clinical data, aggregate clinical or genomics data (when available),
submission. All authors had access to the raw study data. Data in the
and anonymised clinical study reports through the Vivli web-based data
manuscript were verified by DA, SS, AT, RHA, KS, RMV, PG, VA, KWP,
request platform.
GCKWK, BHB, and MTE. HM was International co-ordinator for the
TACKLE trial and contributed to the data interpretation and writing of Acknowledgments
the manuscript. FDRH contributed to study design, study permissions, We thank the trial participants, their families, and all investigators
interpretation of the data, drafting and editing of the manuscript, and involved in this study. Yee-Man Ching, of AstraZeneca facilitated author
operationalisation of TACKLE in the UK. FP contributed to the discussions, coordinated manuscript development and critically For Good Clinical Practice
supervision, validation, and visualisation of the data. DA, AT, and SS reviewed the manuscript. Marius Albulescu and Karen Near of guidelines see http://annals.org/
contributed to the study design concept, statistical analysis plan, and the AstraZeneca were involved in the study design of TACKLE. Medical aim/article/2424869/good-
interpretation of results. KK contributed to the group discussion of the writing support was provided by India Wright and editorial support was publication-practice-
manuscript. JASC contributed intellectual participation in the structure provided by Sharmin Saleque, Joe Alling, Cellan Ellis, and communicating-company-
of the manuscript, reviewing of literature, revision of statistical analysis, Matthew Stone, all of Core Medica, London, UK, supported by sponsored-medical-research-
data interpretation, the selection of the graphic information, the group AstraZeneca according to Good Publication Practice guidelines. gpp3
www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1 11
Articles
References 16 Agrawal U, Katikireddi SV, McCowan C, et al. COVID-19 hospital
1 Piechotta V, Harder T. Waning of COVID-19 vaccine effectiveness: admissions and deaths after BNT162b2 and ChAdOx1 nCoV-19
individual and public health risk. Lancet 2022; 399: 887–89. vaccinations in 2·57 million people in Scotland (EAVE II):
2 Limb M. Covid-19: Scientists and medics warn that it is too soon to a prospective cohort study. Lancet Respir Med 2021; 9: 1439–49.
lift all restrictions in England. BMJ 2022; 376: o469. 17 Hippisley-Cox J, Coupland CA, Mehta N, et al. Risk prediction of
3 Juthani PV, Gupta A, Borges KA, et al. Hospitalisation among covid-19 related death and hospital admission in adults after
vaccine breakthrough COVID-19 infections. Lancet Infect Dis 2021; COVID-19 vaccination: national prospective cohort study. BMJ 2021;
21: 1485–86. 374: n2244.
4 Dessie ZG, Zewotir T. Mortality-related risk factors of COVID-19: 18 Egan C, Turtle L, Thorpe M, Harrison EM, Semple MG,
a systematic review and meta-analysis of 42 studies and 423,117 Docherty AB. Hospital admission for symptomatic COVID-19 and
patients. BMC Infect Dis 2021; 21: 855. impact of vaccination: analysis of linked data from the Coronavirus
5 Dougan M, Nirula A, Azizad M, et al. Bamlanivimab plus Clinical Information Network and the National Immunisation
etesevimab in mild or moderate COVID-19. N Engl J Med 2021; Management Service. Anaesthesia 2022; 77: 605–08.
385: 1382–92. 19 Kemp SA, Collier DA, Datir RP, et al. SARS-CoV-2 evolution during
6 Gupta A, Gonzalez-Rojas Y, Juarez E, et al. Early treatment for treatment of chronic infection. Nature 2021; 592: 277–82.
COVID-19 with SARS-CoV-2 neutralizing antibody sotrovimab. 20 Our World in Data. Coronavirus (COVID-19) vaccinations. 2022.
N Engl J Med 2021; 385: 1941–50. https://ourworldindata.org/covid-vaccinations (accessed
7 Weinreich DM, Sivapalasingam S, Norton T, et al. REGEN-COV March 18, 2022).
antibody combination and outcomes in outpatients with COVID-19. 21 Danza P, Koo TH, Haddix M, et al. SARS-CoV-2 infection and
N Engl J Med 2021; 385: e81. hospitalization among adults aged ≥18 years, by vaccination status,
8 National Institutes of Health. Therapeutic management of before and during SARS-CoV-2 B.1.1.529 (omicron) variant
nonhospitalized adults with COVID-19. 2022. https://www. predominance—Los Angeles County, California, November 7, 2021–
covid19treatmentguidelines.nih.gov/management/clinical- January 8, 2022. MMWR Morb Mortal Wkly Rep 2022; 71: 177–81.
management/nonhospitalized-adults--therapeutic- 22 Iacobucci G. Covid-19: How is vaccination affecting hospital
management/?utm_source=site&utm_medium=home&utm_ admissions and deaths? BMJ 2021; 374: n2306.
campaign=highlights (accessed March 18, 2022). 23 Levin MJ, Ustianowski A, De Wit S, et al. Intramuscular AZD7442
9 Hammond J, Leister-Tebbe H, Gardner A, et al. Oral nirmatrelvir (tixagevimab–cilgavimab) for prevention of COVID-19. N Engl J Med
for high-risk, nonhospitalized adults with COVID-19. N Engl J Med 2022; published online April 20. https://doi.org/10.1056/
2022; 386: 1397–408. NEJMoa2116620.
10 VanBlargan LA, Errico JM, Halfmann PJ, et al. An infectious 24 O’Brien MP, Forleo-Neto E, Musser BJ, et al. Subcutaneous
SARS-CoV-2 B.1.1.529 omicron virus escapes neutralization by REGEN-COV antibody combination to prevent COVID-19.
therapeutic monoclonal antibodies. Nat Med 2022; 28: 490–95. N Engl J Med 2021; 385: 1184–95.
11 Dejnirattisai W, Huo J, Zhou D, et al. SARS-CoV-2 25 US Food and Drug Administration. Fact sheet for health care
Omicron-B.1.1.529 leads to widespread escape from neutralizing providers: emergency use authorization (EUA) of bamlanivimab
antibody responses. Cell 2022; 185: 467–84.e15. and etesevimab. 2021. https://www.fda.gov/media/145802/
12 Loo YM, McTamney PM, Arends RH, et al. The SARS-CoV-2 download (accessed March 14, 2022).
monoclonal antibody combination, AZD7442, is protective in 26 Scientific Advisory Group for Emergencies. NERVTAG: antiviral
nonhuman primates and has an extended half-life in humans. drug resistance and the use of directly acting antiviral drugs (DAAs)
Sci Transl Med 2022; 14: eabl8124. for COVID-19, 8 December 2021. 2021. https://www.gov.uk/
13 US Food and Drug Administration. Fact sheet for healthcare government/publications/nervtag-antiviral-drug-resistance-and-the-
providers: emergency use authorization for Evusheld™ use-of-directly-acting-antiviral-drugs-daas-for-covid-19-8-
(tixagevimab co-packaged with cilgavimab). 2021. https://www.fda. december-2021/
gov/media/154701/download (accessed March 6, 2022). nervtag-antiviral-drug-resistance-and-the-use-of-directly-acting-
antiviral-drugs-daas-for-covid-19-8-december-2021 (accessed
14 WHO Working Group on the Clinical Characterisation
March 18, 2022).
Management of COVID-19 Infection. A minimal common outcome
measure set for COVID-19 clinical research. Lancet Infect Dis 2020; 27 Phiri P, Delanerolle G, Al-Sudani A, Rathod S. COVID-19 and
20: e192–97. Black, Asian, and minority ethnic communities: a complex
relationship without just cause. JMIR Public Health Surveill 2021;
15 Antonelli M, Penfold RS, Merino J, et al. Risk factors and disease
7: e22581.
profile of post-vaccination SARS-CoV-2 infection in UK users of the
COVID Symptom Study app: a prospective, community-based, 28 Iketani S, Liu L, Guo Y, et al. Antibody evasion properties of
nested, case-control study. Lancet Infect Dis 2022; 22: 43–55. SARS-CoV-2 omicron sublineages. Nature 2022; 604: 553–56.
12 www.thelancet.com/respiratory Published online June 7, 2022 https://doi.org/10.1016/S2213-2600(22)00180-1
You might also like
- Infections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumFrom EverandInfections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- 2022 ProventDocument13 pages2022 ProventMARIA LEIVANo ratings yet
- Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine CandidatesDocument12 pagesSafety and Immunogenicity of Two RNA-Based Covid-19 Vaccine CandidatesOKE channelNo ratings yet
- Efficacy and Safety of The CVnCoV SARS CoV 2 MRNA Vaccine Candidate in Ten Countries in Europe and Latin America HERALDDocument12 pagesEfficacy and Safety of The CVnCoV SARS CoV 2 MRNA Vaccine Candidate in Ten Countries in Europe and Latin America HERALDMerel GewoonNo ratings yet
- VACUNADocument12 pagesVACUNACARMEN ROGELIO QUINTERO VEGANo ratings yet
- Fase II: Oxford y AstraZeneca Publicaron en The Lancet Que Lograron 99% de Eficacia en Su Vacuna Contra El COVID-19Document15 pagesFase II: Oxford y AstraZeneca Publicaron en The Lancet Que Lograron 99% de Eficacia en Su Vacuna Contra El COVID-19Urgente24No ratings yet
- Articles: BackgroundDocument12 pagesArticles: BackgroundBudi Haryadi PNo ratings yet
- Capstone 2Document11 pagesCapstone 2mauriciosagredoNo ratings yet
- Safety and Immunogenicity of One Versus Two Doses of BNT162b2Document14 pagesSafety and Immunogenicity of One Versus Two Doses of BNT162b2Simona VisanNo ratings yet
- Lectura de InmunologiaDocument10 pagesLectura de InmunologiaLuzmarina LinoNo ratings yet
- Jama Naggie 2022 Oi 220112 1665760895.44932Document9 pagesJama Naggie 2022 Oi 220112 1665760895.44932Jeancarlo Ore LazoNo ratings yet
- Pi IsDocument19 pagesPi IsJohnnathan MolinaNo ratings yet
- Outpatient Treatment of COVID-19 and Incidence of post-COVID-19 Condition Over 10 MonthsDocument11 pagesOutpatient Treatment of COVID-19 and Incidence of post-COVID-19 Condition Over 10 MonthsStavya DubeyNo ratings yet
- Final-efficacy-analysis,-interim-safety-analysis,-Document12 pagesFinal-efficacy-analysis,-interim-safety-analysis,-Gêmili BalbinotNo ratings yet
- Jama Naggie 2023 Oi 230017 1676655303.18801Document10 pagesJama Naggie 2023 Oi 230017 1676655303.18801Mahmoud AbouelsoudNo ratings yet
- (Channon-Wells, 2023) Immunoglobulin, Glucocorticoid, or CombinationDocument16 pages(Channon-Wells, 2023) Immunoglobulin, Glucocorticoid, or CombinationwiraNo ratings yet
- Duration of Protection Against Mild and Severe Disease by Covid-19 VaccinesDocument11 pagesDuration of Protection Against Mild and Severe Disease by Covid-19 VaccinesPercy CcalachuaNo ratings yet
- Paper Alumnos 3 PDFDocument10 pagesPaper Alumnos 3 PDFVictor Martinez HagenNo ratings yet
- Safety, Immunogenicity, and Efficacy of The BNT162b2 Covid-19 Vaccine in AdolescentsDocument12 pagesSafety, Immunogenicity, and Efficacy of The BNT162b2 Covid-19 Vaccine in AdolescentsCristhian RamírezNo ratings yet
- Nejmoa 2115869Document11 pagesNejmoa 2115869carb0ne14rNo ratings yet
- Ivermectin JournalDocument11 pagesIvermectin JournalShahidatul Aqmal SahidinNo ratings yet
- 1 s2.0 S1473309922003450 MainDocument9 pages1 s2.0 S1473309922003450 Maincathylamont816No ratings yet
- .RCT - Covid - Week 6Document10 pages.RCT - Covid - Week 6Hưng QuếNo ratings yet
- Articles: BackgroundDocument12 pagesArticles: BackgroundCésar Aguirre RomeroNo ratings yet
- Covid 19 y Vacuna PfizerDocument13 pagesCovid 19 y Vacuna PfizerSMIBA MedicinaNo ratings yet
- Efficacy and Safety of A RecombinantDocument13 pagesEfficacy and Safety of A RecombinantSofyanNo ratings yet
- New England Journal Medicine: The ofDocument13 pagesNew England Journal Medicine: The ofSorina ElenaNo ratings yet
- GlofitamabDocument12 pagesGlofitamabsuperequsNo ratings yet
- Nejmoa 2107934Document10 pagesNejmoa 2107934Vj McNo ratings yet
- Nejm DeltaDocument10 pagesNejm DeltaTim MooreNo ratings yet
- Articles: BackgroundDocument11 pagesArticles: Backgroundjose steven garciaNo ratings yet
- Journal of Infection: Letter To The EditorDocument3 pagesJournal of Infection: Letter To The Editorjose steven garciaNo ratings yet
- PIIS0140673620312083Document10 pagesPIIS0140673620312083kayegi8666No ratings yet
- Original Investigation: Key PointsDocument14 pagesOriginal Investigation: Key PointsFernando GómezNo ratings yet
- Rosas, Et AllDocument14 pagesRosas, Et AllrezaNo ratings yet
- PIIS014067362101429XDocument10 pagesPIIS014067362101429XRosamel FierroNo ratings yet
- Pi is 2213260022000595Document10 pagesPi is 2213260022000595Gustavo VitoriaNo ratings yet
- Jama Al Kaabi 2021 Oi 210057 1621966324.79302Document11 pagesJama Al Kaabi 2021 Oi 210057 1621966324.79302Rafiq Khanani DUHSNo ratings yet
- 10 1001@jama 2020 10044Document11 pages10 1001@jama 2020 10044Rodrigo Ehécatl Torres NevárezNo ratings yet
- Safety and Impact of Anti-COVID-19 Vaccines in Psoriatic Patients Treated With Biologics: A Real Life ExperienceDocument4 pagesSafety and Impact of Anti-COVID-19 Vaccines in Psoriatic Patients Treated With Biologics: A Real Life ExperiencePande Agung MahariskiNo ratings yet
- P009 Assessing The Status Quo Ulcerative Colitis.10Document2 pagesP009 Assessing The Status Quo Ulcerative Colitis.10Santiago ZamudioNo ratings yet
- Plasma Conv Full ArticleDocument9 pagesPlasma Conv Full ArticlemahamedicNo ratings yet
- Jamainternal Gupta 2020 Oi 200087 1612820283.07938Document11 pagesJamainternal Gupta 2020 Oi 200087 1612820283.07938veranisa suciaNo ratings yet
- VasculitisDocument12 pagesVasculitisMaite OrellanaNo ratings yet
- Early Treatment For Covid-19 With SARS-CoV-2Document10 pagesEarly Treatment For Covid-19 With SARS-CoV-2Rice FarmerNo ratings yet
- COVID-19 Vaccination of Patients With Chronic Immune-Mediated Inflammatory DiseaseDocument6 pagesCOVID-19 Vaccination of Patients With Chronic Immune-Mediated Inflammatory DiseaseSangeetha VijianNo ratings yet
- Corticosteroids For Bacterial Meningitis in Adults in Sub-Saharan AfricaDocument10 pagesCorticosteroids For Bacterial Meningitis in Adults in Sub-Saharan AfricaMutiara KhalishNo ratings yet
- Sinovac JournalDocument10 pagesSinovac JournalGeulissa AddiniNo ratings yet
- Sputnik V en The LancetDocument11 pagesSputnik V en The LancetLARED21No ratings yet
- Nejmoa 2209760Document11 pagesNejmoa 2209760Gaspar PonceNo ratings yet
- Jama Caricchio 2021 Oi 210064 1626283669.23567Document10 pagesJama Caricchio 2021 Oi 210064 1626283669.23567eastareaNo ratings yet
- Articles: BackgroundDocument11 pagesArticles: BackgroundCRS1973No ratings yet
- PIIS2213858722001589Document10 pagesPIIS2213858722001589frehanyaqNo ratings yet
- Jama 2020 17022Document13 pagesJama 2020 17022wiwiNo ratings yet
- Treatment With Tocilizumab or Corticosteroids For COVID 2021 Clinical MicroDocument9 pagesTreatment With Tocilizumab or Corticosteroids For COVID 2021 Clinical MicroSusanyi ErvinNo ratings yet
- Effectiveness of BNT162b2 Vaccine Against Critical Covid-19 in AdolescentsDocument11 pagesEffectiveness of BNT162b2 Vaccine Against Critical Covid-19 in AdolescentsSuwandi ChangNo ratings yet
- Antibody Response + Booster Dose+lucasDocument3 pagesAntibody Response + Booster Dose+lucaslucasbochniabuenoNo ratings yet
- Hodgkin Lymphoma: A Comprehensive OverviewFrom EverandHodgkin Lymphoma: A Comprehensive OverviewAndreas EngertNo ratings yet
- AACR 2022 Proceedings: Part A Online-Only and April 10From EverandAACR 2022 Proceedings: Part A Online-Only and April 10No ratings yet
- FDA Draft GuidanceDocument19 pagesFDA Draft Guidancerodrigo sacchiNo ratings yet
- How To Read Meta-AnalysisDocument9 pagesHow To Read Meta-Analysisrodrigo sacchiNo ratings yet
- Mean or Median SurvivalDocument10 pagesMean or Median Survivalrodrigo sacchiNo ratings yet
- 2022 - Cytokine Hemoadsorption During Cardiac Surgery Versus Standard Surgical Care For Infective Endocarditis (REMOVE) - Results From A Multicenter, Randomized, Controlled Trial - BDocument2 pages2022 - Cytokine Hemoadsorption During Cardiac Surgery Versus Standard Surgical Care For Infective Endocarditis (REMOVE) - Results From A Multicenter, Randomized, Controlled Trial - Brodrigo sacchiNo ratings yet
- Modulating The Endocannabinoid Pathway As Treatment For Peripheral Neuropathic Pain A Selected Review of Preclinical StudiesDocument6 pagesModulating The Endocannabinoid Pathway As Treatment For Peripheral Neuropathic Pain A Selected Review of Preclinical Studiesrodrigo sacchiNo ratings yet
- Compare & Contrast Graphic OrganizerDocument3 pagesCompare & Contrast Graphic OrganizerMochi-chanNo ratings yet
- CertificateDocument1 pageCertificateR. Ayyanuperumal AyyanuperumalNo ratings yet
- COVID-19 Bivalent Booster Recommendations for Ages 5Document5 pagesCOVID-19 Bivalent Booster Recommendations for Ages 5Nathaniel LaranjoNo ratings yet
- Certificat de Vaccinare Vaccination CertificateDocument1 pageCertificat de Vaccinare Vaccination CertificateOlga StratanNo ratings yet
- CBSE School Code List 2021 All States & Region, Find It HereDocument17 pagesCBSE School Code List 2021 All States & Region, Find It HereAditya KeshriNo ratings yet
- AstraZeneca COVID-19 vaccine informed consentDocument1 pageAstraZeneca COVID-19 vaccine informed consentJohn BNo ratings yet
- Coronavirus Vaccine Manufacturing Failures of Emergent BioSolutionsDocument28 pagesCoronavirus Vaccine Manufacturing Failures of Emergent BioSolutionsDan Stanton100% (1)
- MSU Vaccine Mandate LawsuitDocument151 pagesMSU Vaccine Mandate LawsuitWWMTNo ratings yet
- 6th Sem Project - NISHADocument57 pages6th Sem Project - NISHANisha SindhuNo ratings yet
- CertificateDocument1 pageCertificateRanjana RanjanaNo ratings yet
- Discussion TextDocument1 pageDiscussion Textsamuel gunawanNo ratings yet
- Certificate for COVID-19 Vaccination in IndiaDocument1 pageCertificate for COVID-19 Vaccination in IndiaTausif KhanNo ratings yet
- Patient Information Sheet On Astrazeneca Covid 19 Vaccine and Thrombosis With Thrombocytopenia Syndrome Tts - 0Document4 pagesPatient Information Sheet On Astrazeneca Covid 19 Vaccine and Thrombosis With Thrombocytopenia Syndrome Tts - 0Bemen BesadaNo ratings yet
- Coronavirus: The Commission Signs First Contract With AstrazenecaDocument2 pagesCoronavirus: The Commission Signs First Contract With AstrazenecaΤσιμπινός ΣπύροςNo ratings yet
- COVID-19 Vaccination Certificate from India's Ministry of HealthDocument1 pageCOVID-19 Vaccination Certificate from India's Ministry of Healthbliss bNo ratings yet
- Antibody Responses To Natural Sars-Cov-2 Infection or After Covid-19 VaccinationDocument14 pagesAntibody Responses To Natural Sars-Cov-2 Infection or After Covid-19 VaccinationGus FerryNo ratings yet
- PSJLC DELTA Class Vaccination FormatDocument6 pagesPSJLC DELTA Class Vaccination FormatServus DeiNo ratings yet
- Malaysian COVID-19 Vaccination Digital Certificate DetailsDocument2 pagesMalaysian COVID-19 Vaccination Digital Certificate DetailsKASTURI MUSANo ratings yet
- Covid-19 Vaccination in IndiaDocument6 pagesCovid-19 Vaccination in IndiaIJRASETPublicationsNo ratings yet
- GCC Structural Steel Supervisor ProfileDocument22 pagesGCC Structural Steel Supervisor ProfileAllwinNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsKirubairajNo ratings yet
- COVID 19 Vaccine Comparison ChartDocument2 pagesCOVID 19 Vaccine Comparison ChartNuklear AdiwenaNo ratings yet
- Annex To Vaxzevria Art.5.3 - Visual Risk Contextualisation: 23 April 2021 Corr EMA/234525/2021 European Medicines AgencyDocument12 pagesAnnex To Vaxzevria Art.5.3 - Visual Risk Contextualisation: 23 April 2021 Corr EMA/234525/2021 European Medicines AgencyLEONARDO CIMBERLENo ratings yet
- Covid Vaccine Status Class MasandiganDocument4 pagesCovid Vaccine Status Class MasandiganServus DeiNo ratings yet
- Vaccination CertificateDocument1 pageVaccination CertificateRAVICHANDRAN TNo ratings yet
- 13 Apr 2021: UPSC Exam Comprehensive News Analysis: A. GS 1 RelatedDocument12 pages13 Apr 2021: UPSC Exam Comprehensive News Analysis: A. GS 1 RelatedArpita Sen BhattacharyaNo ratings yet
- The "Killer Vaccine" Worldwide. 7.9 Billion PeopleDocument21 pagesThe "Killer Vaccine" Worldwide. 7.9 Billion PeoplePedroNo ratings yet
- Newsletter: WHO PharmaceuticalsDocument27 pagesNewsletter: WHO PharmaceuticalsGammachuu Leejjiisa Mul'ataa SabbooqaaNo ratings yet
- Digital COVID Certificate Certificat Digital CovidDocument2 pagesDigital COVID Certificate Certificat Digital CovidБорис РэйлянуNo ratings yet
- dm2023 0146Document12 pagesdm2023 0146RvBombetaNo ratings yet