Professional Documents
Culture Documents
A Drug Burden Index To Define The Functional Burden of Medications in Older People
Uploaded by
Ridzqie DibyantariOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
A Drug Burden Index To Define The Functional Burden of Medications in Older People
Uploaded by
Ridzqie DibyantariCopyright:
Available Formats
ORIGINAL INVESTIGATION
A Drug Burden Index to Define the Functional
Burden of Medications in Older People
Sarah N. Hilmer, MD, PhD; Donald E. Mager, PharmD, PhD; Eleanor M. Simonsick, PhD; Ying Cao, MB;
Shari M. Ling, MD; B. Gwen Windham, MD; Tamara B. Harris, MD, MS; Joseph T. Hanlon, PharmD, MS;
Susan M. Rubin, MPH; Ronald I. Shorr, MD, MS; Douglas C. Bauer, MD, MPH; Darrell R. Abernethy, MD, PhD
Background: Older people carry a high burden of illness formance on the Digit Symbol Substitution Test (anticho-
for which medications are indicated, along with increased linergic exposure, 34.5 vs 35.5, P=.045; sedative exposure,
risk of adverse drug reactions. We developed an index to de- 34.0 vs 35.5, P=.01). Associations were strengthened when
termine drug burden based on pharmacologic principles. exposure was calculated by principles of dose response.
We evaluated the relationship of this index to physical and An increase of 1 U in drug burden index was associated
cognitive performance apart from disease indication. with a deficit of 0.15 point (P⬍.001) on the physical func-
tion scale and 1.5 points (P=.01) on the Digit Symbol Sub-
Methods: Data from the Health, Aging, and Body Com- stitution Test. These values were more than 3 times those
position Study on 3075 well-functioning community- associated with a single comorbid illness.
dwelling persons aged 70 to 79 years were analyzed by mul-
tiple linear regression to assess the cross-sectional association Conclusions: The drug burden index demonstrates that
of drug burden index with a validated composite continu- anticholinergic and sedative drug exposure is associ-
ous measure for physical function, and with the Digit Sym-
ated with poorer function in community-dwelling older
bol Substitution Test for cognitive performance.
people. This pharmacologic approach provides a useful
Results: Use of anticholinergic and sedative medica-
evidence-based tool for assessing the functional effect of
tions was associated with poorer physical performance score exposure to medications in this population.
(anticholinergic exposure, 2.08 vs 2.21, P⬍.001; seda-
tive exposure, 2.09 vs 2.19, P⬍.001) and cognitive per- Arch Intern Med. 2007;167:781-787
O
LDER PEOPLE CARRY BOTH be consistent with current practices in clini-
Author Affiliations: Laboratory a high burden of illness cal decision making.8
of Clinical Investigation and for which medications are The use of drugs with central nervous
Clinical Research Branch,
indicated and an incom- system depressant effects is associated
Intramural Research Program,
National Institute on Aging, pletely understood in- with an estimated 50% increased risk of
Baltimore and Bethesda, Md creased risk of adverse drug reactions.1-3 Evi- falling in older people.9,10 Hip fracture
(Drs Hilmer, Mager, Simonsick, dence to guide prescribing is limited by the has been associated with the use of bar-
Ling, Windham, Harris, and exclusion of older adults with multiple biturates,11 benzodiazepines,12 tricyclic
Abernethy); Division of Clinical medical conditions from participation in antidepressants,13 antipsychotics,13 and
Pharmacology, The Johns selective serotonin reuptake inhibitors.14
Hopkins University, Baltimore
(Dr Cao); Division of Geriatric
For editorial comment Memory test scores are lower in people
taking benzodiazepines. 15 Benzodiaz-
Medicine, University of see page 753 epine use has been associated with lower
Pittsburgh, Pittsburgh, Pa
(Dr Hanlon); Prevention functional status in cross-sectional
controlled clinical trials. Determination of
Sciences Group and Department studies16 and with decline in physical
potentially inappropriate medication use in performance after 4 years.17 High serum
of Medicine, University of
older people is guided predominantly by ex- anticholinergic activity, a measure of
California, San Francisco
(Ms Rubin and Dr Bauer); and pert consensus statements such as the up- peripheral blood anticholinergic burden,
Department of Preventive dated Beers criteria.4 Use of medications de- has been associated with decreased Mini-
Medicine, University of scribed as inappropriate by the Beers criteria Mental State Examination scores 18 in
Tennessee at Memphis has been associated with adverse health out- community-dwelling older people.
(Dr Shorr). Dr Hilmer is now comes in nursing home residents5 and with Balancing the risks of polypharmacy with
with the Department of poorer self-perceived health6 but not with underuse of potentially beneficial drugs in
Medicine, University of Sydney,
decline in self-reported function.7 Devel- older people presents a major challenge. The
Sydney, Australia; Dr Mager is
now with the Department of
opment of an evidence-based approach to association between polypharmacy and in-
Pharmaceutical Sciences, guide appropriate medication use, linking creased risk of inappropriate prescribing19
University at Buffalo, State clinically relevant data such as functional and adverse drug events20,21 has been well
University of New York. measures to medication exposure, would described. Number of medications has also
(REPRINTED) ARCH INTERN MED/ VOL 167, APR 23, 2007 WWW.ARCHINTERNMED.COM
781
©2007 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ by a University of Iowa User on 12/12/2014
been correlated with markers of frailty, such as involun- individuals taking a sedative drug, 12 did not have dose or fre-
tary weight loss and impaired balance.22 However, aware- quency recorded and were treated in the same way.
ness that polypharmacy carries risk is insufficient because
it provides no guidance for identifying the drugs that should MEDICATION BURDEN
be reduced or eliminated to minimize drug-related risk. A
more sophisticated model than simply counting the num- With the use of data from existing studies on the effects of medi-
ber of concurrent medications may assist physicians in the cations on physical and mental function in older people, a for-
risk-benefit assessment when prescribing for older mula for drug burden was derived. Medications were charac-
people.23,24 terized with respect to risk into 3 groups: (1) drugs with
anticholinergic effects, (2) drugs with sedative effects, and (3)
One potential methodologic improvement would in-
total number of medications. Each of these has been associ-
volve testing associations of potentially harmful drugs with ated with increased risk of adverse drug events, falls, and con-
physical or cognitive function in healthier older adults. fusion in older people, and these factors were used in our equa-
Physical and cognitive function represent important di- tion for total drug burden (TDB):
mensions of life quality for older adults that are neces-
sary for independent living.25,26 Performance measures (1) TDB = BAC + BS + BNW,
of lower-extremity function predict disability and mor-
tality. 27,28 Examination of associations in a higher- where AC indicates anticholinergic; B, burden; NW, total num-
functioning population minimizes the potential for the ber of drugs with no anticholinergic or sedative effects; and S, seda-
diseases for which the drugs are prescribed, rather than tive. Medications with clinically significant anticholinergic or seda-
the drugs themselves, to influence outcomes. tive effects were identified by means of Mosby’s Drug Consult30 and
In this study we describe and report an index for “drug the Physicians’ Desk Reference.31 Medications with both anticho-
burden” developed according to pharmacologic prin- linergic and sedative effects were classified as anticholinergic.
ciples that has been applied to a community-dwelling popu- We hypothesized that BAC and BS may be proportional to a
linear additive model of pharmacological effect (E):
lation of persons aged 70 to 79 years (the Health, Aging,
and Body Composition [Health ABC] Study cohort) to ex- E D
(2) = ,
amine the association between medication use and physi- α DR50 + D
cal and cognitive performance. This drug burden index pro-
where ␣ is a proportionality constant, D is the daily dose, and
vides insight into potential drug-related sources of impaired
DR50 is the daily dose to achieve 50% of maximal contributory
function in older adults. This index is proposed as a tool effect at steady state.
that, if validated in other populations, will provide an evi- Because a general DR50 of anticholinergic or sedative effect is
dence-based guide for prescribing in older people. not identifiable and the need for normalizing doses remains, we
redefined DR50 to represent a recommended minimum daily dose
METHODS (␦) as approved by the US Food and Drug Administration:
E D
STUDY POPULATION (3) = .
α δ+D
The Health ABC study population consists of 3075 community- This expression represents a hyperbolic function ranging in value
resident Medicare recipients aged 70 to 79 years, recruited from from 0 to 1 for each drug that will shift depending on the choice
April 1997 to June 1998 from the areas around Pittsburgh, Pa, of ␦. This expression has a pharmacologic basis, whereby effect
and Memphis, Tenn. To participate, subjects were required to intensities ranging from 20% to 80% of maximal will be di-
report no difficulty in walking one-quarter mile, climbing 10 rectly proportional to the logarithm of dose.32
steps, or performing activities of daily living. Baseline assess- Although anticholinergic and sedative drugs act on mul-
ments consisted of a questionnaire administered during a home tiple receptor types and subtypes, we hypothesized that their
visit followed by further questioning and objective assess- cumulative effect would be linear, rather than one of drug syn-
ments during a clinic visit.29 ergism.33 Thus, a simple linear additive model was used to es-
timate the total BAC and BS. We hypothesized that both the pres-
ence of a medication from these groups and the degree of
MEDICATION INVENTORY
exposure to drugs in these groups would be negatively associ-
ated with objective measures of function.
A medication inventory was conducted by research personnel dur-
Both prescription and over-the-counter drugs were included
ing the baseline clinic visit. Participants were instructed to bring
in the analysis. Topical preparations without significant sys-
all prescription and over-the-counter medications used in the past
temic effects were excluded. Analyses were performed with and
2 weeks with them to the clinic visit. The researchers took a struc-
without “as-needed” medications. Where a dose was missing for
tured medication history to confirm the medications actually taken
an anticholinergic or sedative medication (n=18 medications),
by the participants in the previous 2 weeks. For each medication,
the median dose for the population was used in the calculations.
the name, Iowa Drug Information System ingredient code, route
Finally, a composite “drug burden” equation was developed.
of administration, and dose and frequency in which the medica-
The weight assigned to each of the 3 components was based on
tion was taken were recorded. Of the 3075 subjects, 338 had a medi-
the strength of association of each individual component with
cation inventory that reported no medications. Ten did not have
Health ABC score and Digit Symbol Substitution Test (DSST).
a medication inventory recorded and were assumed to be taking
no medications. Of the 775 individuals who reported taking an
anticholinergic drug, 29 did not have dose or frequency recorded. COVARIATES
When numbers of anticholinergic drugs were counted, these 29
individuals were included; however, for calculation of drug bur- Prevalent medical conditions were determined from self-report
den, they were considered to have zero drug burden. Of the 433 of physician diagnoses, assessments, and medication use.29,34 A
(REPRINTED) ARCH INTERN MED/ VOL 167, APR 23, 2007 WWW.ARCHINTERNMED.COM
782
©2007 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ by a University of Iowa User on 12/12/2014
comorbidity score was calculated as the sum of the number of each
of the following conditions: cancer, osteoporosis, osteoarthritis, Table 1. Baseline Characteristics
cerebrovascular disease, cardiac disease, peripheral vascular dis- of Health ABC Study Population
ease, hypertension, diabetes mellitus, pulmonary disease, and vi-
sual impairment. Hospitalization in the previous 12 months was Characteristic Value*
also included. The presence or absence of cognitive impairment Age, y 73.6 ± 2.9
(TengandChui’smodifiedMini-MentalStatusExamination35 score Sex, % male 48
⬍80), depression (Center for Epidemiological Studies–Depression Ethnicity, % black 42
Scale36 score ⬎15), and anxiety (Hopkins Symptom Checklist37 Secondary education, % completed 75
response for fear, tense, or nervous included at least 1 moderate Site, % Memphis, Tenn 50
or at least 2 mild) were separate covariates. Comorbidity score 2.0 ± 1.3
Sociodemographic characteristics (age, race, sex, study site, Depression, anxiety, or cognitive impairment, % 23.8
and high school completion) were also included as covariates Health ABC score 2.2 ± 0.6
because these factors have been associated with health, medi- DSST score 35.2 ± 14.8
cation use, and physical and cognitive performance.29,34 No. of medications excluding those with 3.1 ± 3.3
anticholinergic and sedative effects
Exposed to anticholinergic medications, % 25
OUTCOME MEASURES Exposed to sedative medications, % 14
Drug burden index 0.18 ± 0.35
Physical Function
Abbreviations: DSST, Digit Symbol Substitution Test; Health ABC, Health,
Aging, and Body Composition.
Physical function was determined with the Health ABC perfor-
*Data are mean ± SD unless otherwise stated.
mance score, a modification of the Established Populations for
Epidemiologic Studies of the Elderly summary performance score,
developed for use with higher-functioning older adults.29 The
performance battery comprises 4 timed tests: time to complete fects as well) and 14% had been exposed to sedative drugs
5 chair stands; time held for 3 progressively more difficult stands:
semi-tandem, full tandem, and single-leg up; and gait speed over
(Table 1). Drug assignment to anticholinergic or seda-
6 m on a normal and a narrow (20-cm wide) course. Ratio scores tive groups, the Iowa Drug Information System code, the
from 0 to 1 were calculated for each test, where 1 represents the recommended minimum daily dose (␦), and number of
maximal performance of a healthy older adult. Participants un- individuals exposed to each drug are available on re-
able to perform a test were assigned a score of 0. Ratio scores for quest from the authors.
each test were summed to create a continuous scale from 0 to 4, Findings from the analyses of covariance between ex-
with higher scores representing better function. posure to medications with anticholinergic and seda-
tive properties and Health ABC and DSST scores, adjust-
Attention and Concentration ing for age, sex, race, education, study site, and
comorbidity, are presented in Figure 1. In contrast to
Attention and concentration were assessed by means of the DSST no exposure, any exposure to medications with anticho-
as adapted from the Wechsler Adult Intelligence Scale.38 The DSST linergic and sedative effects was associated with poorer
measurespsychomotorperformance,concentration,andshort-term physical performance score (anticholinergic exposure,
memory, reflected in speed of motor response, recognition of sen-
sory information, and visuomotor coordination. The score repre-
2.08 vs 2.21, P⬍.001; sedative exposure, 2.09 vs 2.19,
sents the number of correct symbols written within 90 seconds. P⬍.001) and cognitive performance on DSST score (an-
ticholinergic exposure, 34.5 vs 35.5, P=.045; sedative ex-
posure, 34.0 vs 35.5, P =.01) (Figure 1A). The inclusion
STATISTICAL ANALYSES of “as-needed” medications had minimal effect on the as-
sociations. Associations persisted when the number of
The relationships between each factor in our hypothesized drug
drugs with anticholinergic or sedative effects was con-
burden index and Health ABC physical function score and DSST
score, controlling for comorbidities and sociodemographic char- sidered (Figure 1B and C) and were stronger when ex-
acteristics, were assessed by means of analysis of covariance and posure was calculated with the principles of dose-
multiple linear regression analysis. The individual contribution response and maximal effect (Figure 1D and E).
of each hypothesized factor in the drug burden index to the func- Figure 2 presents the relationships between total
tional outcomes was used to make a weighted equation for total number of drugs, with and without drugs with anticho-
drug burden. The association of this calculated total drug bur- linergic and sedative effects, and physical and cognitive
den with function was assessed by multiple linear regression. performance scores. The trend toward poorer physical
Statistical analyses were performed with SAS statistical soft- function with increasing number of medications was no
ware (version 9.1; SAS Institute Inc, Cary, NC). All tests were longer observed when drugs with sedative and anticho-
2-tailed, and P⬍.05 was considered statistically significant.
linergic actions were excluded. There was no associa-
tion between number of drugs and DSST, with a trend
RESULTS toward higher cognitive performance with exposure to
increasing numbers of drugs.
At baseline, Health ABC Study participants were aged As described in the “Methods” section, the total drug
73.6±2.9 years, 48% were men, 42% were black, 50% were burden equation was derived from the associations found
from each site, and 75% had completed high school. With between its components and functional performance. The
respect to drug exposure, 25% had been exposed to an- sedative burden and the anticholinergic burden were
ticholinergic drugs (including those with sedative ef- equally weighted because they had similar associations
(REPRINTED) ARCH INTERN MED/ VOL 167, APR 23, 2007 WWW.ARCHINTERNMED.COM
783
©2007 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ by a University of Iowa User on 12/12/2014
2.6 50
A Scheduled Dose
Scheduled Dose and as Needed
45
Health ABC Score 2.4
40
DSST Score
2.2
∗ ∗ ∗ †
∗ 35 † † †
2.0
30
1.8
25
1.6 20
No Yes No Yes No Yes No Yes
Anticholinergic Exposure Sedative Exposure Anticholinergic Exposure Sedative Exposure
50 50
B Health ABC Score C Health ABC Score
2.6 2.6
DSST Score DSST Score
45 45
2.4 2.4
40 40
Health ABC Score
Health ABC Score
DSST Score
DSST Score
2.2 2.2
35 35
‡
2.0 2.0
30 30
1.8 25 1.8 25
1.6 20 1.6 20
0 1 2 3 4 0 1 2 3 4
No. of Medications With Anticholinergic Effects No. of Medications With Sedative Effects
n = 2300 629 116 23 7 n = 2642 360 60 12 1
50 50
D Health ABC Score E Health ABC Score
2.6 2.6
DSST Score DSST Score
45 45
2.4 2.4
40 40
Health ABC Score
Health ABC Score
DSST Score
DSST Score
2.2 2.2 ‡
35 35
‡
2.0 2.0 ‡
30 30
1.8 25 1.8 25
‡
1.6 20 1.6 20
0 0.5 1.0 1.5 0 0.5 1.0 1.5
Anticholinergic Burden Sedative Burden
n = 2329 525 165 56 n = 2654 315 78 28
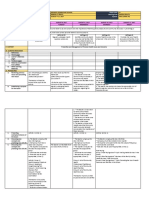
Figure 1. Association between exposure to drugs with anticholinergic or sedative effects and physical function or cognition, controlling for comorbidities and
sociodemographic factors by means of analysis of covariance. A, Subjects who were exposed to drugs with anticholinergic or sedative effects had significantly lower
Health, Aging, and Body Composition (Health ABC) scores and Digit Symbol Substitution Test (DSST) scores than those who were not exposed. Similar results were
seen when as-needed medications were included. *P⬍.001 and †P⬍.05 for differences in Health ABC and DSST scores with exposure to medications.
B and C, Anticholinergic and sedative burden, respectively, calculated as the number of drugs in each class. Weak associations with physical function and cognition are
shown. D and E, Anticholinergic and sedative burdens, respectively, calculated by means of standardized doses of the drugs and the principles of maximal effect. The
associations with physical function and cognition are stronger. The anticholinergic and sedative burdens are rounded in intervals of 0.5 and capped at 1.5. In B through
E, error bars show 95% confidence intervals. ‡P⬍.05 for the difference between the marked point and the previous point on the graph.
with physical and cognitive outcomes. Total number of sedative load. Thus, the equation for total drug burden,
drugs, when sedatives and anticholinergics were ex- TDB (equation 1), was reduced to TDB=BAC ⫹ BS, where
cluded, did not correlate with physical performance or BAC and BS are each the linear additive sum of D/(␦ ⫹ D)
cognition. Consequently, total number of drugs was con- for every anticholinergic or sedative drug to which the
sidered an interactive variable with anticholinergic and subject is exposed (equation 3).
(REPRINTED) ARCH INTERN MED/ VOL 167, APR 23, 2007 WWW.ARCHINTERNMED.COM
784
©2007 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ by a University of Iowa User on 12/12/2014
A 50 B Health ABC Score 50
2.6 2.6 DSST Score
45 45
2.4 2.4
40 ∗ 40
Health ABC Score
Health ABC Score
DSST Score
DSST Score
2.2 2.2
35 35
∗
2.0 2.0
30 30
1.8 25 1.8 25
1.6 20 1.6 20
0 5 10 15 20 25 30 0 5 10 15 20
BN BNW
n = 348 1615 875 187 39 8 3 n = 918 1541 503 92 21
Figure 2. Association of Health, Aging, and Body Composition (Health ABC) physical function score and Digit Symbol Substitution Test (DSST) score with the
total number of drugs (BN) (A) or the total number of drugs excluding those with anticholinergic or sedative effects (BNW) (B), rounded to the nearest 5. Error bars
show 95% confidence intervals. *P⬍.05 for the difference between the marked point and the previous point on the graph.
On testing the association between drug burden and
function, increasing anticholinergic and sedative drug bur- Table 2. Multiple Regression Analyses for Association
of Drug Burden With Physical Function (Health ABC Score)
den was associated with poorer physical function, as and DSST Score*
shown in the regression table (Table 2) (Figure 3).
Each additional unit of drug burden had a negative effect Parameter
on physical function (measured by Health ABC score) Factor Estimate t Pr ⬎|t | R2
similar to that of 3 additional physical comorbidities, and Model for Health ABC Score
a greater effect than anxiety, depression, or cognitive im- Age −0.04 −12.18 ⬍.001
pairment. Each additional unit of drug burden had a nega- Sex, F −0.27 −15.34 ⬍.001
tive effect on DSST similar to that of 4 additional physi- Race, black −0.24 −12.20 ⬍.001
cal comorbidities, and half the effect of anxiety, depression, Study site, Memphis, −0.04 −2.34 ⬍.05
or cognitive impairment. Tenn
Secondary education, −0.16 −6.91 ⬍.001
absent
COMMENT Comorbidity −0.05 −7.30 ⬍.001
Anxiety, depression, or −0.09 −5.67 ⬍.001
In this study of well-functioning community-dwelling older cognitive impairment
people, the degree of exposure to medications with anti- Drug burden −0.15 −5.73 ⬍.001
cholinergic or sedating effects was associated with poorer 0.23
performance on physical mobility and cognitive tasks. Using Model for DSST Score
the definition of drug burden developed herein that ac- Age −0.78 −10.60 ⬍.001
counts for dose and frequency of use to determine expo- Sex, F 3.84 9.07 ⬍.001
sure strengthens the association. This association was not Race, black −10.77 −23.25 ⬍.001
Study site, Memphis −3.92 −9.16 ⬍.001
attributable to sociodemographic factors or comorbidity. Secondary education, −10.62 −19.83 ⬍.001
The total number of drugs taken was not associated with absent
poorer objective functioning when drugs with anticho- Comorbidity −0.36 −2.24 ⬍.05
linergic and sedative effects were excluded. Anxiety, depression, or −3.07 −8.08 ⬍.001
The lack of association between total medications and cognitive impairment
Drug burden −1.51 −2.50 .01
function is of particular interest because previous stud-
0.40
ies39 have shown an association between number of medi-
cations and falls, and an intervention that reduced the num- Abbreviations: DSST, Digit Symbol Substitution Test; Health ABC, Health,
ber of medications decreased the likelihood of falling in Aging, and Body Composition.
community-dwelling older persons.39 Our data indicate that *The parameter estimates tell the amount of change in functional score that
when drugs that impair function are excluded, the asso- would be predicted by a 1-U change in the predictor. The t and Pr ⬎|t | columns
provide the t value and 2-tailed P value used in testing the null hypothesis that
ciation of number of drugs taken with poorer function is the parameter estimate is 0. The R 2 is the proportion of variance in the
lost. This may be influenced by the association with better functional score that can be predicted from the independent variables.
function of some drugs, such as angiotensin-converting en-
zyme inhibitors, hydroxymethylglutaryl coenzyme A re-
ductase inhibitors, and testosterone, in older people. role of dose in adverse outcomes associated with benzo-
The model of drug burden described herein incorpo- diazepines has been demonstrated empirically for seda-
rates dose-response relationships and empirical data. The tion,2 falls,15,17 and injuries.39 These studies either looked
(REPRINTED) ARCH INTERN MED/ VOL 167, APR 23, 2007 WWW.ARCHINTERNMED.COM
785
©2007 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ by a University of Iowa User on 12/12/2014
over time.27 The significant association of drug burden
Health ABC Score 50 with poorer physical function (Figure 3) is similar in mag-
2.6 DSST Score nitude (0.2 SD, statistically small) to the difference in
45 physical function scores in individuals with and with-
2.4
out diabetes mellitus from the Health ABC Study popu-
40 lation,42 suggesting a clinically relevant degree of change.
The DSST is a well-established measure of cognition in-
Health ABC Score
DSST Score
2.2 ∗
35 fluenced by drug use.43 Health ABC and DSST scores, the
∗ 2 outcomes used in this study, were independent of each
2.0
30 other, with only 10% covariance on linear regression
∗ analysis. Despite incorporating most factors known to in-
1.8 25
fluence function, this model captures only 23% of the vari-
ability in Health ABC functional score and 40% in the
1.6 20
DSST, which may reflect the well-recognized, poorly un-
0 1 2 3 derstood significant interindividual variability in older
Drug Burden people.44
n = 2077 882 104 12 We have established an association between increas-
ing drug burden index and function in a cross-sectional
Figure 3. Association of increasing drug burden with decreasing scores for data set from which the index was derived. The strength
physical function and cognition. Drug burden was rounded to integers and of the association with these outcomes could be further
capped at 3 (1 subject had a drug burden ⬎3). Error bars show 95%
confidence intervals. *P⬍.05 for the difference between the marked point tested in the Health ABC Study cohort and other popu-
and the previous point on the graph. Health ABC indicates Health, Aging, and lations of older people by means of cross-sectional and
Body Composition; DSST, Digit Symbol Substitution Test. longitudinal data analysis. Analysis of associations be-
tween drug burden index at baseline and future func-
for a linear dose-response effect or used number of drugs tion, and change in drug burden index and change in func-
prescribed as a surrogate for dose. Our calculation of drug tion over time, may clarify this relationship.
burden incorporated a classic dose-response relation- Finally, the study’s careful adjustment for comorbid
ship assuming linear additive effects.32 illnesses is required on the basis of the established
There are limitations to this pharmacologic model as relationship between comorbidity and functional limi-
an index of drug burden. The substitution of the mini- tations.42,45,46 This study’s rigorous assessment of medi-
mum efficacious dose for the dose that gives 50% of the cal conditions as potential confounders increases our
effect is an estimate. The degree of error in this estimate confidence with which the relationship between drug
probably varies among drugs and among subjects with burden and functional limitations can be reported.
different pharmacokinetic and pharmacodynamic pro- Future studies will be required to determine the asso-
files. It is possible that the accuracy of our model could ciation between drug burden and function in frail
be further improved by including drug-drug interac- older people.
tions, considering the relative affinity of different drugs
for cholinergic receptors, and including the complexi- CONCLUSIONS
ties of drug synergism.33 However, the drug burden in-
dex calculated by this relatively straightforward model
This study demonstrates that objective mobility and cog-
has an effect on physical function and cognition as mea-
nitive performance in well-functioning older people is as-
sured by the DSST that is comparable to and indepen-
sociated with a drug burden index that accounts for the
dent of that of physical or mental comorbidity.
degree of exposure to drugs with anticholinergic and seda-
This study’s focus on high-functioning, community-
tive effects. These findings provide a basis for evaluating
resident older adults provides a unique perspective from
drug burden when prescribing for even high-functioning
which drug burden is examined. The recording of ac-
older people in the community. The drug burden index
tual medication use was based on inspection of all medi-
could be easily calculated by means of prescribing soft-
cations brought by the subject during a clinic visit. This
ware to inform prescribers of the likely functional impli-
gives more accurate information on exposure than does
cations of an older person’s medications.
information obtained from databases, medical records,
The drug burden calculated in this study correlates
pharmacy records, or subject questionnaires or inter-
well with objective functional measures, providing an evi-
views.40,41 The outcomes used in this study were both ob-
dence base for the association between medication use
jective and clinically relevant. Objective measures of physi-
and functional impairment in high-functioning older
cal function are superior to self-reported function,
people. Provided that this correlation is also found in other
particularly to differentiate among well-functioning sub-
populations, the calculation of drug burden may be use-
jects who are independent in activities of daily living. The
ful in predicting the effects of medication on function and
Health ABC Study performance scale distinguishes the
therefore guide prescribing for older people.
physical functional capacity of older people at the higher
end of the functional spectrum29 and is based on the Es-
tablished Populations for Epidemiologic Studies of the Accepted for Publication: November 16, 2006.
Elderly scale, which has been shown to predict nursing Correspondence: Darrell R. Abernethy, MD, PhD, Labo-
home admission, mortality, and disability in older people ratory of Clinical Investigation, National Institute on Ag-
(REPRINTED) ARCH INTERN MED/ VOL 167, APR 23, 2007 WWW.ARCHINTERNMED.COM
786
©2007 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ by a University of Iowa User on 12/12/2014
ing, Gerontology Research Center, 5600 Nathan Shock 18. Mulsant BH, Pollock BG, Kirshner M, Shen C, Dodge H, Ganguli M. Serum an-
ticholinergic activity in a community-based sample of older adults: relationship
Dr, Baltimore, MD 21224-6825 (abernethyd@grc.nia.nih
with cognitive performance. Arch Gen Psychiatry. 2003;60:198-203.
.gov). 19. Goulding MR. Inappropriate medication prescribing for elderly ambulatory care
Author Contributions: Study concept and design: Hilmer, patients. Arch Intern Med. 2004;164:305-312.
Mager, Ling, Windham, Hanlon, Shorr, and Abernethy. Ac- 20. Field TS, Gurwitz JH, Avorn J, et al. Risk factors for adverse drug events among
quisition of data: Simonsick, Harris, Rubin, Bauer, and nursing home residents. Arch Intern Med. 2001;161:1629-1634.
21. Field TS, Gurwitz JH, Harrold LR, et al. Risk factors for adverse drug events among
Abernethy. Analysis and interpretation of data: Hilmer, Mager,
older adults in the ambulatory setting. J Am Geriatr Soc. 2004;52:1349-1354.
Simonsick, Cao, Ling, Hanlon, Shorr, and Abernethy. Draft- 22. Agostini JV, Han L, Tinetti ME. The relationship between number of medications
ing of the manuscript: Hilmer, Mager, Hanlon, and Abernethy. and weight loss or impaired balance in older adults. J Am Geriatr Soc. 2004;
Critical revision of the manuscript for important intellectual 52:1719-1723.
content: Hilmer, Mager, Simonsick, Cao, Ling, Windham, 23. Higashi T, Shekelle PG, Solomon DH, et al. The quality of pharmacologic care
Harris, Hanlon, Rubin, Shorr, Bauer, and Abernethy. Sta- for vulnerable older patients. Ann Intern Med. 2004;140:714-720.
24. Gurwitz JH. Polypharmacy: a new paradigm for quality drug therapy in the elderly?
tistical analysis: Hilmer and Cao. Obtained funding: Harris Arch Intern Med. 2004;164:1957-1959.
and Abernethy. Administrative, technical, and material sup- 25. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the
port: Simonsick, Harris, Rubin, and Abernethy. Study su- aged: the index of ADL: a standardized measure of biological and psychosocial
pervision: Mager, Simonsick, and Abernethy. function. JAMA. 1963;185:914-919.
Financial Disclosure: None reported. 26. Ikegami N. Functional assessment and its place in health care. N Engl J Med.
1995;332:598-599.
Funding/Support: This study was supported by the In- 27. Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity
tramural Research Program of the National Institutes of function in persons over the age of 70 years as a predictor of subsequent disability.
Health, National Institute on Aging, and National Insti- N Engl J Med. 1995;332:556-561.
tute on Aging Contracts NO1-AG-6-2101, NO1-AG-6- 28. Melzer D, Lan TY, Guralnik JM. The predictive validity for mortality of the index
2103, and NO1-AG-6-2106. of mobility-related limitation: results from the EPESE study. Age Ageing. 2003;
32:619-625.
29. Simonsick EM, Newman AB, Nevitt MC, et al. Measuring higher level physical
REFERENCES function in well-functioning older adults: expanding familiar approaches in the
Health ABC study. J Gerontol A Biol Sci Med Sci. 2001;56:M644-M649.
30. Nissen D, ed. Mosby’s Drug Consult. St Louis, Mo: Mosby Inc; 2004.
1. Steel K, Gertman PM, Crescenzi C, Anderson J. Iatrogenic illness on a general
31. Duplay D, ed. Physicians’ Desk Reference. 58th ed. Montvale, NJ: Thomson PDR;
medical service at a university hospital. N Engl J Med. 1981;304:638-642.
2004.
2. Greenblatt DJ, Allen MD. Toxicity of nitrazepam in the elderly: a report from the
32. Levy G. Kinetics of pharmacologic effects. Clin Pharmacol Ther. 1966;7:362-372.
Boston Collaborative Drug Surveillance Program. Br J Clin Pharmacol. 1978;
33. Tallarida RJ. Drug synergism: its detection and applications. J Pharmacol Exp
5:407-413.
3. Montamat SC, Cusack BJ, Vestal RE. Management of drug therapy in the elderly. Ther. 2001;298:865-872.
N Engl J Med. 1989;321:303-309. 34. Rosano C, Simonsick EM, Harris TB, et al. Association between physical and cog-
4. Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers nitive function in healthy elderly: the Health, Aging and Body Composition Study.
criteria for potentially inappropriate medication use in older adults: results of a US Neuroepidemiology. 2005;24:8-14.
consensus panel of experts. Arch Intern Med. 2003;163:2716-2724. 35. Teng EL, Chui HC. The Modified Mini-Mental State (3MS) examination. J Clin
5. Lau DT, Kasper JD, Potter DE, Lyles A, Bennett RG. Hospitalization and death Psychiatry. 1987;48:314-318.
associated with potentially inappropriate medication prescriptions among el- 36. Weissman MM, Sholomskas D, Pottenger M, Prusoff BA, Locke BZ. Assessing
derly nursing home residents. Arch Intern Med. 2005;165:68-74. depressive symptoms in five psychiatric populations: a validation study. Am J
6. Fu AZ, Liu GG, Christensen DB. Inappropriate medication use and health out- Epidemiol. 1977;106:203-214.
comes in the elderly. J Am Geriatr Soc. 2004;52:1934-1939. 37. Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L. The Hopkins Symp-
7. Hanlon JT, Fillenbaum GG, Kuchibhatla M, et al. Impact of inappropriate drug tom Checklist (HSCL): a measure of primary symptom dimensions. Mod Probl
use on mortality and functional status in representative community dwelling elders. Pharmacopsychiatry. 1974;7:79-110.
Med Care. 2002;40:166-176. 38. Wechsler D. WAIS-R Manual. Cleveland, Ohio: Psychologic Corp; 1981.
8. Sackett DL, Rosenberg WM. The need for evidence-based medicine. J R Soc Med. 39. Tinetti ME, Baker DI, McAvay G, et al. A multifactorial intervention to reduce the
1995;88:620-624. risk of falling among elderly people living in the community. N Engl J Med. 1994;
9. Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a sys- 331:821-827.
tematic review and meta-analysis, I: psychotropic drugs. J Am Geriatr Soc. 1999; 40. Ray WA, Griffin MR. Use of Medicaid data for pharmacoepidemiology. Am J
47:30-39. Epidemiol. 1989;129:837-849.
10. Ensrud KE, Blackwell TL, Mangione CM, et al. Central nervous system-active medi- 41. Moore N, Pierfitte C, Pehourcq F, Lagnaoui R, Begaud B. Comparison of patient
cations and risk for falls in older women. J Am Geriatr Soc. 2002;50:1629-1637. questionnaires, medical records, and plasma assays in assessing exposure to
11. Macdonald JB, Macdonald ET. Barbiturates and fractures. Br Med J. 1977;2:891. benzodiazepines in elderly subjects. Clin Pharmacol Ther. 2001;69:445-450.
12. Ray WA, Griffin MR, Downey W. Benzodiazepines of long and short elimination 42. De Rekeneire N, Resnick HE, Schwartz AV, et al. Diabetes is associated with sub-
half-life and the risk of hip fracture. JAMA. 1989;262:3303-3307. clinical functional limitation in nondisabled older individuals: the Health, Aging,
13. Ray WA, Griffin MR, Schaffner W, Baugh DK, Melton LJ III. Psychotropic drug and Body Composition study. Diabetes Care. 2003;26:3257-3263.
use and the risk of hip fracture. N Engl J Med. 1987;316:363-369. 43. Greenblatt DJ, Harmatz JS, Dorsey C, Shader RI. Comparative single-dose ki-
14. Liu B, Anderson G, Mittmann N, To T, Axcell T, Shear N. Use of selective serotonin- netics and dynamics of lorazepam, alprazolam, prazepam, and placebo. Clin Phar-
reuptake inhibitors of tricyclic antidepressants and risk of hip fractures in el- macol Ther. 1988;44:326-334.
derly people. Lancet. 1998;351:1303-1307. 44. Gurwitz JH, Avorn J. The ambiguous relation between aging and adverse drug
15. Hanlon JT, Horner RD, Schmader KE, et al. Benzodiazepine use and cognitive func- reactions. Ann Intern Med. 1991;114:956-966.
tion among community-dwelling elderly. Clin Pharmacol Ther. 1998;64:684-692. 45. Guralnik JM, LaCroix AZ, Abbott RD, et al. Maintaining mobility in late life, I: demo-
16. Ried LD, Johnson RE, Gettman DA. Benzodiazepine exposure and functional sta- graphic characteristics and chronic conditions. Am J Epidemiol. 1993;137:
tus in older people. J Am Geriatr Soc. 1998;46:71-76. 845-857.
17. Gray SL, Penninx BW, Blough DK, et al. Benzodiazepine use and physical per- 46. Fried LP, Bandeen-Roche K, Kasper JD, Guralnik JM. Association of comorbid-
formance in community-dwelling older women. J Am Geriatr Soc. 2003;51: ity with disability in older women: the Women’s Health and Aging Study. J Clin
1563-1570. Epidemiol. 1999;52:27-37.
(REPRINTED) ARCH INTERN MED/ VOL 167, APR 23, 2007 WWW.ARCHINTERNMED.COM
787
©2007 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ by a University of Iowa User on 12/12/2014
You might also like
- Surviving Cancer, COVID-19, and Disease: The Repurposed Drug RevolutionFrom EverandSurviving Cancer, COVID-19, and Disease: The Repurposed Drug RevolutionNo ratings yet
- Ioi15013 1013 1019Document7 pagesIoi15013 1013 1019Sundas EjazNo ratings yet
- Artigo 2Document13 pagesArtigo 2Paulo TononNo ratings yet
- STart StroppDocument1 pageSTart StroppHoang Mai NguyenNo ratings yet
- Potentially Inappropriate Medications Defined by STOPP Criteria and The Risk of Adverse Drug Events in Older Hospitalized Patients FREEDocument14 pagesPotentially Inappropriate Medications Defined by STOPP Criteria and The Risk of Adverse Drug Events in Older Hospitalized Patients FREENurul FitryaniNo ratings yet
- Antipsychotics For Preventing Delirium in Hospitalized AdultsDocument12 pagesAntipsychotics For Preventing Delirium in Hospitalized AdultsLuis CsrNo ratings yet
- Efficacy and Acceptability of Pharmacological Treat-Ments For Depressive Disorders in Primary Care: Systematic Review and Network Meta-AnalysisDocument11 pagesEfficacy and Acceptability of Pharmacological Treat-Ments For Depressive Disorders in Primary Care: Systematic Review and Network Meta-AnalysisPutri YingNo ratings yet
- Using Human Genetics To Improve Safety Assessment of TherapeuticsDocument18 pagesUsing Human Genetics To Improve Safety Assessment of TherapeuticsSergio VillicañaNo ratings yet
- Prevalence of Self-Medication and Associated Factors in An Elderly Population: A Systematic ReviewDocument14 pagesPrevalence of Self-Medication and Associated Factors in An Elderly Population: A Systematic ReviewRomário CerqueiraNo ratings yet
- Reducing Inappropriate Polypharmacy The Process of DeprescribingDocument8 pagesReducing Inappropriate Polypharmacy The Process of DeprescribingThiago SartiNo ratings yet
- Nihms 439055Document31 pagesNihms 439055Amalia NandiaNo ratings yet
- Medications and Falls in Older People: Geriatric TherapeuticsDocument4 pagesMedications and Falls in Older People: Geriatric TherapeuticsMamenn DicinieNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundPsiquiatría CESAMENo ratings yet
- Potential For Interactions Between Dietary Supplements and Prescription MedicationsDocument5 pagesPotential For Interactions Between Dietary Supplements and Prescription MedicationsMuhammad DeddyNo ratings yet
- Co-Prescription Trends in A Large Cohort of Subjects Predict Substantial Drug-Drug InteractionsDocument19 pagesCo-Prescription Trends in A Large Cohort of Subjects Predict Substantial Drug-Drug Interactionsadern-07huepfendNo ratings yet
- Wait-and-See Prescription For The Treatment of Acute Otitis MediaDocument7 pagesWait-and-See Prescription For The Treatment of Acute Otitis MediaatikahanifahNo ratings yet
- Chakelba 2013Document9 pagesChakelba 2013Nawang WulanNo ratings yet
- Chittaranjan, A. 2017Document4 pagesChittaranjan, A. 2017Andrea HenaoNo ratings yet
- Article 10Document7 pagesArticle 10vzwsvt7hgkNo ratings yet
- Phytotherapy Research - 2018 - Yeung - Herbal Medicine For Depression and Anxiety A Systematic Review With Assessment ofDocument27 pagesPhytotherapy Research - 2018 - Yeung - Herbal Medicine For Depression and Anxiety A Systematic Review With Assessment ofolivia.f.parrishNo ratings yet
- Ethn 15 01 116Document8 pagesEthn 15 01 116Bot AINo ratings yet
- Linnen Et Al. (2011) - Depression and Essential Health Risk Factors in Surgical Patients in The Preoperative Anaesthesiological Assessment ClinicDocument9 pagesLinnen Et Al. (2011) - Depression and Essential Health Risk Factors in Surgical Patients in The Preoperative Anaesthesiological Assessment Clinicfabienne czechNo ratings yet
- 1642-Article Text-7699-1-10-20200623Document5 pages1642-Article Text-7699-1-10-20200623mtgnzgaNo ratings yet
- Nonpharmacological Interventions To Prevent DeliriumDocument12 pagesNonpharmacological Interventions To Prevent Deliriumjuan.pablo.castroNo ratings yet
- Nejme 2301045Document2 pagesNejme 2301045Billy LamNo ratings yet
- Drug Interactions-Principles, Examples and Clinical ConsequencesDocument12 pagesDrug Interactions-Principles, Examples and Clinical ConsequencesNispap Harami RJNo ratings yet
- Efficacy of Antidepressants and Benzodiazepines in Minor Depression Systematic Review and MetaanalysisDocument6 pagesEfficacy of Antidepressants and Benzodiazepines in Minor Depression Systematic Review and MetaanalysisChica MirandaNo ratings yet
- Identificación y Validación de Objetivos Farmacológicos Controlados GenéticamenteDocument13 pagesIdentificación y Validación de Objetivos Farmacológicos Controlados GenéticamenteBrayanTrujilloNo ratings yet
- 529-Einstein 5 3 1 246-251Document7 pages529-Einstein 5 3 1 246-251Gatwech DechNo ratings yet
- Ejr 4 2 109Document4 pagesEjr 4 2 109andrianiputri916No ratings yet
- 6-Comparacion de Ejercicio Vs Farmacos LongevidadDocument9 pages6-Comparacion de Ejercicio Vs Farmacos LongevidadflorNo ratings yet
- Effectiveness and Adverse Drug Reactions of Levetiracetam and Midazolam in Refractory Neonatal Seizure: A Cross Sectional Comparative StudyDocument6 pagesEffectiveness and Adverse Drug Reactions of Levetiracetam and Midazolam in Refractory Neonatal Seizure: A Cross Sectional Comparative StudySultan Rahmat SeptianNo ratings yet
- A Comparison of Acute Treatment Regimens For Migraine in The Emergency DepartmentDocument9 pagesA Comparison of Acute Treatment Regimens For Migraine in The Emergency DepartmentAndreas NatanNo ratings yet
- The Active Comparator, New User Study Design in Pharmacoepidemiology: Historical Foundations and Contemporary ApplicationDocument8 pagesThe Active Comparator, New User Study Design in Pharmacoepidemiology: Historical Foundations and Contemporary ApplicationDici RachmandaNo ratings yet
- Comparative Associations Between Measures of AntiDocument10 pagesComparative Associations Between Measures of AntiLuisFernandoValladalesRestrepoNo ratings yet
- Appi Ajp 2018 17111282Document14 pagesAppi Ajp 2018 17111282Alan AlvídrezNo ratings yet
- Arch Intern Med Medication Errors Observed in 36 Health Care Facilities 2002Document7 pagesArch Intern Med Medication Errors Observed in 36 Health Care Facilities 2002alejandromfunes1749No ratings yet
- Yildiz 2014Document19 pagesYildiz 2014Lorrane NevesNo ratings yet
- 673 FullDocument7 pages673 FullAq IfahNo ratings yet
- Reconciliacao MedicamentosaDocument22 pagesReconciliacao MedicamentosapchrispimNo ratings yet
- POTENTIAL DRUG INTERACTIONS IN INTENSIVE CARE PATIENTS AT A Teaching HospitalDocument6 pagesPOTENTIAL DRUG INTERACTIONS IN INTENSIVE CARE PATIENTS AT A Teaching HospitalJuwita RamadhaniNo ratings yet
- Determinants and Effects of Self-Administration With Nsaids in A Tertiary Care Hospital of Eastern IndiaDocument6 pagesDeterminants and Effects of Self-Administration With Nsaids in A Tertiary Care Hospital of Eastern IndiaAnoop ThoombayilNo ratings yet
- Drug Interactions-Principles Examples and ClinicalDocument13 pagesDrug Interactions-Principles Examples and ClinicalRaudhatul JannahNo ratings yet
- Pharmacological Aspects: Pharmacogenetics and Outcome With Antipsychotic DrugsDocument12 pagesPharmacological Aspects: Pharmacogenetics and Outcome With Antipsychotic DrugsFuad AlamsyahNo ratings yet
- Book Reviews: Prescribing by Numbers: Drugs and The Definition of DiseaseDocument3 pagesBook Reviews: Prescribing by Numbers: Drugs and The Definition of DiseasehernanbotinaNo ratings yet
- FG 4Document7 pagesFG 4Veronica BalanNo ratings yet
- Artigo Lancet Medicamentos AnsiedadeDocument10 pagesArtigo Lancet Medicamentos AnsiedadeRebecca DiasNo ratings yet
- Computerized ProgramDocument7 pagesComputerized ProgramfatiisaadatNo ratings yet
- Mother NejmDocument12 pagesMother NejmIzara Maité Mondragón MorenoNo ratings yet
- Substance Abuse? A Meta-Analytic Review of The Literature Does Stimulant Therapy of Attention-Deficit/Hyperactivity Disorder Beget LaterDocument9 pagesSubstance Abuse? A Meta-Analytic Review of The Literature Does Stimulant Therapy of Attention-Deficit/Hyperactivity Disorder Beget LaterNatália Macedo CavagnoliNo ratings yet
- Relationships Between Beliefs About Medications AnDocument7 pagesRelationships Between Beliefs About Medications Annoor cahayaNo ratings yet
- Is The Efficacy of Antidepressants in Panic Disorder Mediated by Adverse Events? A Mediational AnalysisDocument12 pagesIs The Efficacy of Antidepressants in Panic Disorder Mediated by Adverse Events? A Mediational AnalysisYulistia AsmiNo ratings yet
- Painreports 2 E589Document7 pagesPainreports 2 E589goliath.chad2000No ratings yet
- Gonzales 2013Document7 pagesGonzales 2013Nurul AiniNo ratings yet
- Past, Present, and Future of Drug-Drug Interactions PDFDocument3 pagesPast, Present, and Future of Drug-Drug Interactions PDFCatalina Del CantoNo ratings yet
- Barrionuevo 2018Document7 pagesBarrionuevo 2018hlwNo ratings yet
- Health Risk Behaviors With Synthetic Cannabinoids Versus MarijuanaDocument12 pagesHealth Risk Behaviors With Synthetic Cannabinoids Versus MarijuanaDr Monal YuwanatiNo ratings yet
- Mbe 2017 (Ajm)Document5 pagesMbe 2017 (Ajm)Anderson CarvalhoNo ratings yet
- Article - False Positive Interferences of Common UDS ImmunoassaysDocument10 pagesArticle - False Positive Interferences of Common UDS ImmunoassayshmNo ratings yet
- Sexton 2011Document19 pagesSexton 2011koushikNo ratings yet
- Academy Pocket Guide To Pediatric Nutrition 2nd Edition Sample ChapterDocument6 pagesAcademy Pocket Guide To Pediatric Nutrition 2nd Edition Sample ChapterGanes Tiara WidhaNo ratings yet
- ADHD in ChildrenDocument10 pagesADHD in ChildrenDebbie KlippNo ratings yet
- Dialog Percakapan Bidan Tugas Bahs Inggris DedeDocument5 pagesDialog Percakapan Bidan Tugas Bahs Inggris DedeSardianto TurnipNo ratings yet
- Review Combat Against COVID-19 Complications - Traditional Plant Lantana CamaraDocument5 pagesReview Combat Against COVID-19 Complications - Traditional Plant Lantana CamaraInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of School Facilities On The Learning EnvironmentDocument174 pagesThe Impact of School Facilities On The Learning EnvironmentEnrry Sebastian71% (31)
- K102 Referencing FAQs 21JDocument5 pagesK102 Referencing FAQs 21JpaulNo ratings yet
- Material Safety Data Sheet Ecol Lube SilDocument4 pagesMaterial Safety Data Sheet Ecol Lube Silfs1640No ratings yet
- Potential Health Benefits of Garlic Allium SativumDocument26 pagesPotential Health Benefits of Garlic Allium SativumAlyssa SagarioNo ratings yet
- Keywords: Rural Nursing, Rural Nursing Theory, Synergy Model, SynergyDocument13 pagesKeywords: Rural Nursing, Rural Nursing Theory, Synergy Model, Synergyputri dewiNo ratings yet
- Shaping A Humane World Edward J. Valeau, Rosalind L. RabyDocument17 pagesShaping A Humane World Edward J. Valeau, Rosalind L. RabySTAR ScholarsNo ratings yet
- Review Article: Common Periodontal Diseases of Children and AdolescentsDocument8 pagesReview Article: Common Periodontal Diseases of Children and AdolescentsGea Akalili SabrinaNo ratings yet
- Ro10 Bukidnon Provincial Medical Center Malaybalay CityDocument37 pagesRo10 Bukidnon Provincial Medical Center Malaybalay Citycaleb castilloNo ratings yet
- Apps For Paediatric Dosing - An Evaluation - Vonbach PriskaDocument1 pageApps For Paediatric Dosing - An Evaluation - Vonbach PriskaSara KreboldNo ratings yet
- Hricak 2021Document37 pagesHricak 2021Xiomara CelyNo ratings yet
- The Concepts and Principles of Equity and HealthDocument18 pagesThe Concepts and Principles of Equity and HealthPaulo César López BarrientosNo ratings yet
- CIF - Version 9 GENE XPERT POST MORTEMDocument3 pagesCIF - Version 9 GENE XPERT POST MORTEMBALIUAG DISTRICT LABORATORYNo ratings yet
- 7 Tips To Stay Mentally Healthy During CrisisDocument2 pages7 Tips To Stay Mentally Healthy During CrisisnoemiNo ratings yet
- HSE AwarenessDocument70 pagesHSE Awarenessعبدالحميد عبدالغفار الدرديري50% (2)
- Text For NoDocument3 pagesText For NoMasita NazalinNo ratings yet
- DLL in MAPEH 6 - Health Week 10Document4 pagesDLL in MAPEH 6 - Health Week 10Sara Jane C. Jose-TayaoNo ratings yet
- Uterine Therapeutics: by Henry MintonDocument48 pagesUterine Therapeutics: by Henry MintonSravs Pandu100% (1)
- HemivaginaDocument3 pagesHemivaginafitriamarizkaNo ratings yet
- Management of The Short Bowel Syndrome in Adults - UpToDateDocument10 pagesManagement of The Short Bowel Syndrome in Adults - UpToDateyessyNo ratings yet
- Pazoki Et Al. 2022 - Efficacy and Safety of Saffron As Adjunctive Therapy in Adults With ADHDDocument7 pagesPazoki Et Al. 2022 - Efficacy and Safety of Saffron As Adjunctive Therapy in Adults With ADHDLaura DecockNo ratings yet
- 09 Prostate Cancer 2017 WebDocument146 pages09 Prostate Cancer 2017 WebDharmesh PatelNo ratings yet
- MSDS 984229Document16 pagesMSDS 984229anibal_rios_rivasNo ratings yet
- Economics For Pharmaceutical ManagementDocument29 pagesEconomics For Pharmaceutical ManagementTifa IstiwaNo ratings yet
- Fusion Center Study Finds 79% of Recent Mass Shootings Attributable To History of Mental Illness - Public IntelligenceDocument11 pagesFusion Center Study Finds 79% of Recent Mass Shootings Attributable To History of Mental Illness - Public IntelligenceTy UsikNo ratings yet
- Ddis DSM 5Document20 pagesDdis DSM 5AlexisMolinaCampuzanoNo ratings yet
- l3 Measures of Population Impact and Infectiouness NotesDocument9 pagesl3 Measures of Population Impact and Infectiouness Notestheus_35No ratings yet