You might also like
- 2011 ApmsaDocument302 pages2011 ApmsaChristopher SchmittNo ratings yet
- Lesson 1 - Introduction To Psychiatric Mental HealthDocument63 pagesLesson 1 - Introduction To Psychiatric Mental HealthHazel Roda EstorqueNo ratings yet
- Operating Room ProcedureDocument4 pagesOperating Room ProcedureROxanne S. RendonNo ratings yet
- Transitions in Dying and Bereavement: A Psychosocial Guide For Hospice and Palliative Care, Second Edition (Excerpt)Document12 pagesTransitions in Dying and Bereavement: A Psychosocial Guide For Hospice and Palliative Care, Second Edition (Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.20% (5)
- Written Assignment: Reflective WritingDocument9 pagesWritten Assignment: Reflective WritingNur Aziemah Mohd Zamri100% (1)
- 118 RLE Infection Control PDFDocument15 pages118 RLE Infection Control PDFclaire yowsNo ratings yet
- Association Between Proton Pump Inhibitor Use and Spontaneous Bacterial PeritonitisDocument5 pagesAssociation Between Proton Pump Inhibitor Use and Spontaneous Bacterial PeritonitisMuhammad Rehan AnisNo ratings yet
- Varietal EsophagusDocument10 pagesVarietal EsophagusgigibesiNo ratings yet
- Risk factors and outcomes of infection types in spontaneous bacterial peritonitisDocument7 pagesRisk factors and outcomes of infection types in spontaneous bacterial peritonitisphonex xoxNo ratings yet
- Laroche 1998Document9 pagesLaroche 1998takechi takechiNo ratings yet
- v01 Pneumonia Rapid Testing Case Study - DorDocument4 pagesv01 Pneumonia Rapid Testing Case Study - DorJanet TranNo ratings yet
- Microbes Predict Outcomes Complicated Lung InfectionsDocument9 pagesMicrobes Predict Outcomes Complicated Lung InfectionsabhikanjeNo ratings yet
- Jurnal 3Document6 pagesJurnal 3Rafiqa Zulfi UmmiahNo ratings yet
- Prophylaxis Against Fungal Peritonitis in CAPD A Single Center Experience With Low Dose FluconazoleDocument5 pagesProphylaxis Against Fungal Peritonitis in CAPD A Single Center Experience With Low Dose FluconazoleJorge David Gamez PeñarandaNo ratings yet
- Clinical-Liver, Pancreas, and Biliary TractDocument8 pagesClinical-Liver, Pancreas, and Biliary TractKirsten HartmanNo ratings yet
- Absceso Hepático NeonatalDocument6 pagesAbsceso Hepático NeonatalNabila Peña ZapataNo ratings yet
- Tamma Et Al., 2015Document7 pagesTamma Et Al., 2015Caio Bonfim MottaNo ratings yet
- Fecal microbiota transplant for Crohn disease_ ADocument8 pagesFecal microbiota transplant for Crohn disease_ AMartinaNo ratings yet
- A Pilot Study of Vidofludimus Calcium For Treatment of Primary Sclerosing CholangitisDocument9 pagesA Pilot Study of Vidofludimus Calcium For Treatment of Primary Sclerosing CholangitisrachelNo ratings yet
- IndianJMedRes1386995-8025199 221731Document8 pagesIndianJMedRes1386995-8025199 221731dinda annisaNo ratings yet
- Avances en Sepsis Art Ing 2022Document10 pagesAvances en Sepsis Art Ing 2022roman rodriguezNo ratings yet
- Clinical Trial: Effectiveness of Lactobacillus Rhamnosus (Strains E N, Oxy and Pen) in The Prevention of Antibiotic-Associated Diarrhoea in ChildrenDocument8 pagesClinical Trial: Effectiveness of Lactobacillus Rhamnosus (Strains E N, Oxy and Pen) in The Prevention of Antibiotic-Associated Diarrhoea in ChildrenBryan Paul RamirezNo ratings yet
- Usefulness of Presepsin As A Diagnostic and Prognostic Marker of Sepsis in Daily Clinical PracticeDocument7 pagesUsefulness of Presepsin As A Diagnostic and Prognostic Marker of Sepsis in Daily Clinical Practicefaraz.mirza1No ratings yet
- Peritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDocument9 pagesPeritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDesi HutapeaNo ratings yet
- Risk Factors and Pattern of Changes in Liver Enzymes Among The Patients With Anti-Tuberculosis Drug-Induced HepatitisDocument3 pagesRisk Factors and Pattern of Changes in Liver Enzymes Among The Patients With Anti-Tuberculosis Drug-Induced HepatitisnazarNo ratings yet
- 03Document10 pages03Luis ReyesNo ratings yet
- Ceftriaxone Compared With Sodium Penicillin G For Treatment of Severe LeptospirosisDocument9 pagesCeftriaxone Compared With Sodium Penicillin G For Treatment of Severe LeptospirosisFifi SumarwatiNo ratings yet
- Systematic Review: Tuberculous Peritonitis - Presenting Features, Diagnostic Strategies and TreatmentDocument16 pagesSystematic Review: Tuberculous Peritonitis - Presenting Features, Diagnostic Strategies and TreatmenthendraNo ratings yet
- JurnalDocument5 pagesJurnalgustina mariantiNo ratings yet
- Kel 5 Sirosis HepatikDocument9 pagesKel 5 Sirosis HepatikJorianditha RamadhanNo ratings yet
- SBP Investigation and TreatmentDocument3 pagesSBP Investigation and TreatmentBaihaqi SaharunNo ratings yet
- Four-Month Moxifloxacin-Based Regimens For Drug-Sensitive TuberculosisDocument9 pagesFour-Month Moxifloxacin-Based Regimens For Drug-Sensitive TuberculosisTheodoraAnamariaNo ratings yet
- Efficacy of Levofloxacin in The Treatment of BK Viremia - A Multicenter, Double-Blinded, Randomized, Placebo-Controlled Trial - PMCDocument15 pagesEfficacy of Levofloxacin in The Treatment of BK Viremia - A Multicenter, Double-Blinded, Randomized, Placebo-Controlled Trial - PMCWEE LENG GANNo ratings yet
- Genexpert - On Body Fluid SpecimensDocument4 pagesGenexpert - On Body Fluid Specimensramo G.No ratings yet
- A Candidate Probiotic With Unfavourable Effects in Subjects With Irritable Bowel Syndrome: A Randomised Controlled TrialDocument7 pagesA Candidate Probiotic With Unfavourable Effects in Subjects With Irritable Bowel Syndrome: A Randomised Controlled Trialdolo2000No ratings yet
- Carbapenemico OralDocument12 pagesCarbapenemico Oralalejandro montesNo ratings yet
- Hoa 3Document9 pagesHoa 3ruth angelinaNo ratings yet
- Fungal Infections in Neonates: Risks, Diagnosis and TreatmentDocument5 pagesFungal Infections in Neonates: Risks, Diagnosis and TreatmentaseelNo ratings yet
- Daud Jurnal PDFDocument9 pagesDaud Jurnal PDFAngga PratamaNo ratings yet
- Diagnostic and Prognostic Biomarkers of Sepsis in Critical CareDocument8 pagesDiagnostic and Prognostic Biomarkers of Sepsis in Critical Caremr_curiousityNo ratings yet
- Proton Pump Inhibitor Initiation and Withdrawal Affects Gut Microbiota and Readmission Risk in CirrhosisDocument11 pagesProton Pump Inhibitor Initiation and Withdrawal Affects Gut Microbiota and Readmission Risk in CirrhosisMirzania Mahya FathiaNo ratings yet
- Choosing Antibiotic Therapy For Severe Community-Acquired PneumoniaDocument7 pagesChoosing Antibiotic Therapy For Severe Community-Acquired PneumoniaJuan Sebastian SuarezNo ratings yet
- Procalcitonin GuidanceDocument44 pagesProcalcitonin GuidanceMiguel Chung SangNo ratings yet
- Antibiotic Prophylaxis in Cirrhosis: Good and Bad: ReviewsDocument13 pagesAntibiotic Prophylaxis in Cirrhosis: Good and Bad: ReviewsGiani Herrera HurtadoNo ratings yet
- Abcesele FicatuluiDocument4 pagesAbcesele FicatuluiMihaela AlinaNo ratings yet
- Song 2018Document7 pagesSong 2018Jonathan RyanNo ratings yet
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsDocument9 pagesResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998No ratings yet
- Do Proton Pump Inhibitors Increase Mortality in Cirrhotic Patients With Spontaneous Bacterial Peritonitis?Document29 pagesDo Proton Pump Inhibitors Increase Mortality in Cirrhotic Patients With Spontaneous Bacterial Peritonitis?Muhammad Rehan AnisNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyMuhammad AsrizalNo ratings yet
- Prognostic Factors in Tuberculosis Related Mortalities in Hospitalized PatientsDocument7 pagesPrognostic Factors in Tuberculosis Related Mortalities in Hospitalized PatientsAshok PanjwaniNo ratings yet
- Sepsis - Eval and MGMTDocument62 pagesSepsis - Eval and MGMTDr Ankit SharmaNo ratings yet
- Jurnal Intensified Antituberculosis Therapy in Adult With Tuberculous MeningitisDocument13 pagesJurnal Intensified Antituberculosis Therapy in Adult With Tuberculous Meningitisnaila ghinayaNo ratings yet
- (03241750 - Acta Medica Bulgarica) Fungal Peritonitis Due To Gastroduodenal Perforation - Diagnostic and Treatment ChallengesDocument8 pages(03241750 - Acta Medica Bulgarica) Fungal Peritonitis Due To Gastroduodenal Perforation - Diagnostic and Treatment ChallengesTeodorNo ratings yet
- Usefulness of Presepsin in Diagnosing SepsisDocument7 pagesUsefulness of Presepsin in Diagnosing SepsisMuhammad Anshory AkNo ratings yet
- CoryneDocument8 pagesCoryneEsther Najera GalarretaNo ratings yet
- Nebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaDocument4 pagesNebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaPhan Tấn TàiNo ratings yet
- Abdominal Sepsis Prognostic FactorDocument6 pagesAbdominal Sepsis Prognostic FactorPrasojo JojoNo ratings yet
- Causes and Factors of Persistent Pneumonia in ChildrenDocument4 pagesCauses and Factors of Persistent Pneumonia in ChildrenBereket temesgenNo ratings yet
- 394 Full PDFDocument20 pages394 Full PDFHaltiNo ratings yet
- Effect of Lactobacillus Rhamnosus On Serum Uremic Toxins (Phenol and P-Cresol) in Hemodialysis PatientsDocument7 pagesEffect of Lactobacillus Rhamnosus On Serum Uremic Toxins (Phenol and P-Cresol) in Hemodialysis PatientsOctavianus KevinNo ratings yet
- 09 2019 Pediatric Neonatology LAYOUT R2Document50 pages09 2019 Pediatric Neonatology LAYOUT R2khalid alharbiNo ratings yet
- BMC Infectious Diseases: Study ProtocolDocument9 pagesBMC Infectious Diseases: Study ProtocolyuenkeithNo ratings yet
- Once-Daily Plazomicin For Complicated Urinary Tract InfectionsDocument12 pagesOnce-Daily Plazomicin For Complicated Urinary Tract InfectionsharvardboyNo ratings yet
- Hepatitis B Virus and Liver DiseaseFrom EverandHepatitis B Virus and Liver DiseaseJia-Horng KaoNo ratings yet
- Palliative Care of Stomach CancerDocument16 pagesPalliative Care of Stomach Cancerurmila prajapatiNo ratings yet
- 3 RdmolarDocument25 pages3 RdmolarocadaNo ratings yet
- Description of Theory of Unpleasant SymptomsDocument14 pagesDescription of Theory of Unpleasant SymptomsGithaiga Kimani100% (1)
- MSI TemplateDocument3 pagesMSI TemplateKenneth LuciferNo ratings yet
- Resume For WeeblyDocument1 pageResume For Weeblyapi-241346165No ratings yet
- PHTLS Lessone 3Document28 pagesPHTLS Lessone 3Adel AlkaliliNo ratings yet
- Case Pres ZandiOrstDocument17 pagesCase Pres ZandiOrstNajeeb UllahNo ratings yet
- Neonatal Fever Clinical PathwayDocument55 pagesNeonatal Fever Clinical PathwayAdvocateforPedsNo ratings yet
- Supercharge your career with KSOM's Super MBA in Business AnalyticsDocument24 pagesSupercharge your career with KSOM's Super MBA in Business AnalyticsVirat TiwariNo ratings yet
- Inspector Checklist Website Version Sep12Document7 pagesInspector Checklist Website Version Sep12pradip_26No ratings yet
- Reasons For Extraction of Primary Teeth in Jordan-A Study.: August 2013Document5 pagesReasons For Extraction of Primary Teeth in Jordan-A Study.: August 2013Mutia KumalasariNo ratings yet
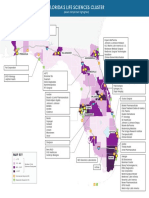
- Florida's Life Sciences Cluster MapDocument1 pageFlorida's Life Sciences Cluster MapCocoNo ratings yet
- 2020 Covid Deaths Ffs EmsDocument5 pages2020 Covid Deaths Ffs EmsepraetorianNo ratings yet
- MBBS Curriculum 1st Revision 2014 15122014Document478 pagesMBBS Curriculum 1st Revision 2014 15122014gangadharpath123100% (1)
- Nursing Service Division Risks and OpportunitiesDocument38 pagesNursing Service Division Risks and OpportunitiesStephanie BadilloNo ratings yet
- ANAGHADocument82 pagesANAGHAanagha ajithNo ratings yet
- Individual Mental Health AssignmentDocument18 pagesIndividual Mental Health AssignmentRebekah Roberts100% (1)
- Top Dentists 2010: Now say 'ahhhhDocument10 pagesTop Dentists 2010: Now say 'ahhhhpassapgoldyNo ratings yet
- DAFTAR PUSTAKA GabunganDocument9 pagesDAFTAR PUSTAKA GabunganIda Bagus MustikaNo ratings yet
- Diary Retail (AutoRecovered)Document56 pagesDiary Retail (AutoRecovered)Maizurah ZulkafliNo ratings yet
- References: The M Word: How To Thrive in Menopause by DR Ginni MansbergDocument51 pagesReferences: The M Word: How To Thrive in Menopause by DR Ginni MansbergAllen & Unwin0% (1)
- Nursing-Care-Plan Case 1 LaquihonDocument2 pagesNursing-Care-Plan Case 1 LaquihonRuby Jane LaquihonNo ratings yet
- EAU Guidelines On Male Sexual Dysfunction 2019Document96 pagesEAU Guidelines On Male Sexual Dysfunction 2019Muti IlmarifaNo ratings yet
- The Validation of The Moorehead-Ardelt Quality of Life Questionnaire IIDocument9 pagesThe Validation of The Moorehead-Ardelt Quality of Life Questionnaire IIVictoria DowningNo ratings yet