You might also like
- New Technique Combined With Suture and PDFDocument8 pagesNew Technique Combined With Suture and PDFzachvuhaNo ratings yet
- Midcheek Lift Using Facial Soft-Tissue Spaces of The MidcheekDocument11 pagesMidcheek Lift Using Facial Soft-Tissue Spaces of The MidcheekЩербакова ЛенаNo ratings yet
- Wang 2019Document10 pagesWang 2019Hải Dương MinhNo ratings yet
- Snodgrass HypospDocument11 pagesSnodgrass HypospRajarshi KumarNo ratings yet
- Transpalpebral Corrugator Resection: 25-Year Experience, Refinements and Additional IndicationsDocument7 pagesTranspalpebral Corrugator Resection: 25-Year Experience, Refinements and Additional IndicationsMehmet SürmeliNo ratings yet
- Ahn 2013Document2 pagesAhn 2013Aliénor VienneNo ratings yet
- Trabeculectomy TechniqueDocument8 pagesTrabeculectomy TechniqueJose Antonio Fuentes VegaNo ratings yet
- Current Concepts in BlepharoplastyDocument11 pagesCurrent Concepts in BlepharoplastyRajinder Kumar Bassan100% (1)
- Surgical Eye ProceduresDocument4 pagesSurgical Eye ProceduresLeonela SánchezNo ratings yet
- Squisis MacularDocument8 pagesSquisis MacularremotmNo ratings yet
- Translabprevention CSFJCGPRLDocument5 pagesTranslabprevention CSFJCGPRLJohn GoddardNo ratings yet
- Umbilical Surgery in CalvesDocument11 pagesUmbilical Surgery in CalvesguadialvarezNo ratings yet
- Coclia EyelidDocument5 pagesCoclia EyelidFaradila HakimNo ratings yet
- Upperlidblepharoplasty: A Current PerspectiveDocument9 pagesUpperlidblepharoplasty: A Current PerspectivedoctorbanNo ratings yet
- PIIS1043181018300332Document4 pagesPIIS1043181018300332Ottofianus Alvedo Hewick KalangiNo ratings yet
- Crawley 2015Document6 pagesCrawley 2015Eduardo HernándezNo ratings yet
- Medial Ectropion Repair of Lower Eyelids With A Cicatricial ComponentDocument3 pagesMedial Ectropion Repair of Lower Eyelids With A Cicatricial ComponentDiaz RandanilNo ratings yet
- Etiology and Treatment of Congenital Festoons PDFDocument11 pagesEtiology and Treatment of Congenital Festoons PDFprashanth kenchotiNo ratings yet
- Brachioplasty in The Patient With Massive Weight Loss: Operative StrategiesDocument9 pagesBrachioplasty in The Patient With Massive Weight Loss: Operative StrategiesamdreyNo ratings yet
- Z OllingerDocument6 pagesZ OllingerjylovescarynNo ratings yet
- H&N - Cervical Plexus BlockDocument9 pagesH&N - Cervical Plexus BlockJane KoNo ratings yet
- Blefaroplastia en AsiaticosDocument11 pagesBlefaroplastia en AsiaticosLiliana Cepeda GarcíaNo ratings yet
- Internal MastopexyDocument7 pagesInternal MastopexyfumblefumbleNo ratings yet
- Sling LiftDocument6 pagesSling LiftBFF BotoxNo ratings yet
- Blepharoplasty: ExtendedDocument4 pagesBlepharoplasty: ExtendedBFF BotoxNo ratings yet
- Limited Scar .Reed2014Document11 pagesLimited Scar .Reed2014Rafael FerreiraNo ratings yet
- Eyelid Blepharoplasty: ExtendedDocument4 pagesEyelid Blepharoplasty: ExtendedBFF BotoxNo ratings yet
- Power of The Pinch Pinch Lower Lid BlepharoplastyDocument6 pagesPower of The Pinch Pinch Lower Lid BlepharoplastyBFF BotoxNo ratings yet
- Strategies To Improve Outcomes From Operative Childhood Management of DDHDocument9 pagesStrategies To Improve Outcomes From Operative Childhood Management of DDHVALENTINA LOPEZ MARINNo ratings yet
- Final Versionof Vascular Chaptersfor OHOSFigueiredo BhattacharyaDocument44 pagesFinal Versionof Vascular Chaptersfor OHOSFigueiredo BhattacharyaKing ThiyagaNo ratings yet
- A Novel Strategy To Achieve Stable and Lasting Double Eyelids in Upper BlepharoplastyDocument4 pagesA Novel Strategy To Achieve Stable and Lasting Double Eyelids in Upper BlepharoplastyRaul FonsecaNo ratings yet
- Mayo 1901Document9 pagesMayo 1901Martin BergerNo ratings yet
- Four Flaps Technique For Neoumbilicoplasty: Young Taek Lee, Chan Kwon, Seung Chul Rhee, Sang Hun Cho, Su Rak EoDocument5 pagesFour Flaps Technique For Neoumbilicoplasty: Young Taek Lee, Chan Kwon, Seung Chul Rhee, Sang Hun Cho, Su Rak Eojuan carlos pradaNo ratings yet
- The M-Y Axilloplasty After Massive Weight Loss: Analysis of 159 Consecutive PatientsDocument6 pagesThe M-Y Axilloplasty After Massive Weight Loss: Analysis of 159 Consecutive PatientsamdreyNo ratings yet
- Umbilicalherniarepair: Overview of Approaches and Review of LiteratureDocument16 pagesUmbilicalherniarepair: Overview of Approaches and Review of LiteratureVictor Matias BarriosNo ratings yet
- The Translabyrinthine Approach: James Bowman, MBBS, BDSC, FracsDocument8 pagesThe Translabyrinthine Approach: James Bowman, MBBS, BDSC, FracsSebastianNo ratings yet
- EDAMS Nota Tecnica GoodDocument4 pagesEDAMS Nota Tecnica GoodnaimNo ratings yet
- Paediatric Caudal AnaesthesiaDocument5 pagesPaediatric Caudal AnaesthesiaSuresh KumarNo ratings yet
- Upperblepharoplasty: The Aesthetic IdealDocument6 pagesUpperblepharoplasty: The Aesthetic IdealFelyana GunawanNo ratings yet
- deltopectoral approachDocument4 pagesdeltopectoral approachAlex DiconiNo ratings yet
- Superficial Parotidectomy Through Retrograde Facial Nerve DissectionDocument8 pagesSuperficial Parotidectomy Through Retrograde Facial Nerve DissectionAnonymous LnWIBo1GNo ratings yet
- Lelouarn 2007Document10 pagesLelouarn 2007saul iranNo ratings yet
- Open Access Atlas of Otolaryngology, Head & Neck Operative SurgeryDocument16 pagesOpen Access Atlas of Otolaryngology, Head & Neck Operative SurgeryMihai Ionut TanaseNo ratings yet
- Excision of Preauricular Pits and SinusesDocument7 pagesExcision of Preauricular Pits and SinusesHNo ratings yet
- Total LaryngectomyDocument15 pagesTotal LaryngectomyKumaran Bagavathi RagavanNo ratings yet
- Full Endoscopic Bilateral Over The Top Decompression in LumbarDocument6 pagesFull Endoscopic Bilateral Over The Top Decompression in Lumbarckilincer2No ratings yet
- Suturing of The Arachnoid Membrane For Reconstruction of The Cisterna MagnaDocument5 pagesSuturing of The Arachnoid Membrane For Reconstruction of The Cisterna MagnaAlejandro Zurita SaáNo ratings yet
- Tensioned Reverse Abdominoplasty: BackgroundDocument8 pagesTensioned Reverse Abdominoplasty: BackgroundlarissaNo ratings yet
- Bozola 2009Document7 pagesBozola 2009Mariangel HinojosaNo ratings yet
- Surgical Atlas Primary Hypospadias Repair With Buccal MucosaDocument19 pagesSurgical Atlas Primary Hypospadias Repair With Buccal MucosaNurul Simatupang100% (1)
- OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK SURGERYDocument7 pagesOPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK SURGERYjoshnaNo ratings yet
- Blepharoplasty Text BookDocument12 pagesBlepharoplasty Text BookHisham Seify MD,PhD100% (1)
- Superior Pedicle Reduction Mammaplasty: Operative Strategies Operative StrategiesDocument7 pagesSuperior Pedicle Reduction Mammaplasty: Operative Strategies Operative StrategiesitsvamshikrishNo ratings yet
- Avelar Abdoplasty ExpDocument5 pagesAvelar Abdoplasty Exprandomaeiou7273No ratings yet
- Use of Retroauricular Temporal Flap For Large Post Oncosurgical Glabellar and Forehead DefectsDocument4 pagesUse of Retroauricular Temporal Flap For Large Post Oncosurgical Glabellar and Forehead DefectsPalwasha Malik100% (1)
- Management of Anterior Shoulder Instability Without Bone Loss: Arthroscopic and Mini-Open TechniquesDocument7 pagesManagement of Anterior Shoulder Instability Without Bone Loss: Arthroscopic and Mini-Open TechniquesHari WangsaNo ratings yet
- Awake Craniotomy Anaesthesia GuideDocument7 pagesAwake Craniotomy Anaesthesia GuidePablo Sousa CasasnovasNo ratings yet
- RIDGE RECONSTRUCTION TECHNIQUESDocument14 pagesRIDGE RECONSTRUCTION TECHNIQUESkishanNo ratings yet
- Extended Abdominoplasty - Applications and A New Classification System For AbdominoplastyDocument7 pagesExtended Abdominoplasty - Applications and A New Classification System For AbdominoplastyDaniel Alfonso Gonzalez MercadoNo ratings yet
- The Dome Procedure: A New Technique For The Reconstruction of The UmbilicusDocument4 pagesThe Dome Procedure: A New Technique For The Reconstruction of The UmbilicusfumblefumbleNo ratings yet
- The Impact of Cosmetic Surgery on Women's Marital Satisfaction and Self-ConceptDocument8 pagesThe Impact of Cosmetic Surgery on Women's Marital Satisfaction and Self-ConceptfumblefumbleNo ratings yet
- A Systematic Review of The Factors Predicting The Interest in Cosmetic Plastic SurgeryDocument6 pagesA Systematic Review of The Factors Predicting The Interest in Cosmetic Plastic SurgeryfumblefumbleNo ratings yet
- Scarless Reverse Umbilicoplasty A New Tech - 2019 - Journal of Plastic ReconDocument6 pagesScarless Reverse Umbilicoplasty A New Tech - 2019 - Journal of Plastic Reconjuan carlos pradaNo ratings yet
- Creating The Perfect UmbilicusDocument8 pagesCreating The Perfect UmbilicusfumblefumbleNo ratings yet
- Psychosocial Factors Predicting The Motivation To.9Document12 pagesPsychosocial Factors Predicting The Motivation To.9fumblefumbleNo ratings yet
- Motivating Factors For Seeking Cosmetic SurgeryDocument6 pagesMotivating Factors For Seeking Cosmetic SurgeryfumblefumbleNo ratings yet
- 30 Minute WorkoutDocument14 pages30 Minute WorkoutIordan FlorinNo ratings yet
- удаление комков бишаDocument6 pagesудаление комков бишаAlexey SorokinNo ratings yet
- Comprehensive Approach For Aesthetic Correction of Round FaceDocument7 pagesComprehensive Approach For Aesthetic Correction of Round FacefumblefumbleNo ratings yet
- Gluteal Implants Versus Autologous Flaps in Patients With Postbariatric Surgery Weight LossDocument10 pagesGluteal Implants Versus Autologous Flaps in Patients With Postbariatric Surgery Weight LossfumblefumbleNo ratings yet
- Buccal Fat Pad RemovalDocument2 pagesBuccal Fat Pad RemovalfumblefumbleNo ratings yet
- The Effects of Cosmetic Surgery On BodyDocument7 pagesThe Effects of Cosmetic Surgery On BodyMiran El-MaghrabiNo ratings yet
- A Human Body Mathematical Model Biometric Using Golden Ratio: A New Algorithm Provisional Chapter Golden Ratio: A New AlgorithmDocument25 pagesA Human Body Mathematical Model Biometric Using Golden Ratio: A New Algorithm Provisional Chapter Golden Ratio: A New AlgorithmfumblefumbleNo ratings yet
- Anatomical Study of Pectoral NervesDocument5 pagesAnatomical Study of Pectoral NervesfumblefumbleNo ratings yet
- Facial Reshaping Using Less Invasive MethodsDocument9 pagesFacial Reshaping Using Less Invasive MethodsfumblefumbleNo ratings yet
- Augmentation Mammoplasty:MastopexyDocument12 pagesAugmentation Mammoplasty:MastopexyfumblefumbleNo ratings yet
- Abdominal Etching: Past and PresentDocument10 pagesAbdominal Etching: Past and PresentfumblefumbleNo ratings yet
- Motivating Factors For Seeking Cosmetic SurgeryDocument6 pagesMotivating Factors For Seeking Cosmetic SurgeryfumblefumbleNo ratings yet
- Calf Augmentation and Reshaping With Autologous Fat GraftingDocument10 pagesCalf Augmentation and Reshaping With Autologous Fat GraftingfumblefumbleNo ratings yet
- The Impact of Cosmetic Surgery on Women's Marital Satisfaction and Self-ConceptDocument8 pagesThe Impact of Cosmetic Surgery on Women's Marital Satisfaction and Self-ConceptfumblefumbleNo ratings yet
- Psychosocial Factors Predicting The Motivation To.9Document12 pagesPsychosocial Factors Predicting The Motivation To.9fumblefumbleNo ratings yet
- A Systematic Review of The Factors Predicting The Interest in Cosmetic Plastic SurgeryDocument6 pagesA Systematic Review of The Factors Predicting The Interest in Cosmetic Plastic SurgeryfumblefumbleNo ratings yet
- Abdominoplasty: Pitfalls and ProspectsDocument6 pagesAbdominoplasty: Pitfalls and ProspectsfumblefumbleNo ratings yet
- Arm ContouringDocument11 pagesArm ContouringfumblefumbleNo ratings yet
- Facelift: Joseph L. Leach, JR, MDDocument6 pagesFacelift: Joseph L. Leach, JR, MDfumblefumbleNo ratings yet
- The Effects of Cosmetic Surgery On BodyDocument7 pagesThe Effects of Cosmetic Surgery On BodyMiran El-MaghrabiNo ratings yet
- Facial Filler Agents: Raghu S. Athre, MDDocument5 pagesFacial Filler Agents: Raghu S. Athre, MDfumblefumbleNo ratings yet
- Cosmetic Use of Botulinum Toxin in The Upper Face - 2007 - Operative Techniques in Otolaryngology Head and Neck SurgeryDocument6 pagesCosmetic Use of Botulinum Toxin in The Upper Face - 2007 - Operative Techniques in Otolaryngology Head and Neck SurgeryfumblefumbleNo ratings yet
- Peritonsillar AbscessDocument19 pagesPeritonsillar AbscessMarianne LayloNo ratings yet
- Moh A. Pps Hcai Manual 2.12.21Document136 pagesMoh A. Pps Hcai Manual 2.12.21Nurfarzana NadhirahNo ratings yet
- Mohammad Javed Ali (Auth.) - Atlas of Lacrimal Drainage Disorders (2018, Springer Singapore) PDFDocument684 pagesMohammad Javed Ali (Auth.) - Atlas of Lacrimal Drainage Disorders (2018, Springer Singapore) PDFGustavo HernandezNo ratings yet
- Atlas On The Surgical Anatomy of LaryngDocument2 pagesAtlas On The Surgical Anatomy of LaryngManling JaoNo ratings yet
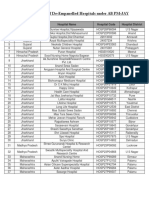
- List of De-Empanelled Hospitals under PM-JAYDocument5 pagesList of De-Empanelled Hospitals under PM-JAYBhawna Chaurasia100% (1)
- The Effect of Pre-And Postmastectomy Radiotherapy On The Degree of Edema, Shoulder-Joint Mobility, and Gripping ForceDocument5 pagesThe Effect of Pre-And Postmastectomy Radiotherapy On The Degree of Edema, Shoulder-Joint Mobility, and Gripping ForceSarly FebrianaNo ratings yet
- Holep Laser Prostectomy - Dr. Shyam VarmaDocument6 pagesHolep Laser Prostectomy - Dr. Shyam Varmashyam varmaNo ratings yet
- CV JD Ghosh 20-08-2021Document32 pagesCV JD Ghosh 20-08-2021Jay Deep GhoshNo ratings yet
- Cleaning A Sutured Wound & Changing A Dressing On A Wound With A Drain Procedure ChecklistDocument3 pagesCleaning A Sutured Wound & Changing A Dressing On A Wound With A Drain Procedure ChecklistMonicaElizadePazNo ratings yet
- Advanced Wound Healing and Professional Scar Management: SwitzerlandDocument7 pagesAdvanced Wound Healing and Professional Scar Management: SwitzerlandAndreeaNo ratings yet
- Runner's Knee (Patellofemoral Pain) : CausesDocument4 pagesRunner's Knee (Patellofemoral Pain) : CausesBarath KannanNo ratings yet
- Siemens Acuson Sc2000 Flyer Combine The Best of Both WorldsDocument8 pagesSiemens Acuson Sc2000 Flyer Combine The Best of Both Worldsbashir019No ratings yet
- 22 Patient Chart Checklist EditedDocument1 page22 Patient Chart Checklist EditedAina HaravataNo ratings yet
- Redundant: A Case of Complicated Dolichocolon in A NeonateDocument4 pagesRedundant: A Case of Complicated Dolichocolon in A NeonateCassNo ratings yet
- BongraftingDocument4 pagesBongraftingjaxine labialNo ratings yet
- Techniques of Local Anesthesia in Ophthalmology: Manbir Singh Bassan R.NO 54Document36 pagesTechniques of Local Anesthesia in Ophthalmology: Manbir Singh Bassan R.NO 54m singhNo ratings yet
- Online Seat Allocation INI-CETDocument2 pagesOnline Seat Allocation INI-CETNael NajeebNo ratings yet
- 10 Tips About Aesthetic ImplantologyDocument16 pages10 Tips About Aesthetic ImplantologyMario Troncoso Andersenn0% (1)
- Thirty Years of Submental Intubation: A Review: Review Paper Oral SurgeryDocument5 pagesThirty Years of Submental Intubation: A Review: Review Paper Oral SurgeryUmer HussainNo ratings yet
- What Made You Choose Your Host Institution/host University?: Do You Already Have Contacts There?Document5 pagesWhat Made You Choose Your Host Institution/host University?: Do You Already Have Contacts There?Carolyn FanNo ratings yet
- GMC Quotation Q200014904049Document4 pagesGMC Quotation Q200014904049pandeyvashishthaNo ratings yet
- Vesicovaginal Fistula RepaireDocument21 pagesVesicovaginal Fistula RepaireFlaviu Ionuț FaurNo ratings yet
- Product Catalog: Smiles That Last A Life TimeDocument312 pagesProduct Catalog: Smiles That Last A Life Timescribd@iamdooser.orgNo ratings yet
- Medical Surgical Nursing Study GiudeDocument5 pagesMedical Surgical Nursing Study GiudeRexson Alcantara DalanginNo ratings yet
- Jaipur Foot Innovation Case StudyDocument30 pagesJaipur Foot Innovation Case StudypriyaNo ratings yet
- Medical DictionaryDocument184 pagesMedical DictionaryHAROLD SCOTT BIDESNo ratings yet
- Anaesthesia For Pancreatic SurgeryDocument11 pagesAnaesthesia For Pancreatic SurgeryDianita P Ñáñez VaronaNo ratings yet
- Cardiac Risk Stratification - CardiologyDocument10 pagesCardiac Risk Stratification - CardiologyDaniel A. Velarde LópezNo ratings yet
- Aldrich Resume FinalDocument2 pagesAldrich Resume Finalapi-532847344No ratings yet
- Preemptive Quadratus Lumborum Laparoscopic BariatricDocument8 pagesPreemptive Quadratus Lumborum Laparoscopic BariatricEmmanuel FortalezaNo ratings yet