You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- September Thursday Communication 1Document26 pagesSeptember Thursday Communication 1api-250858579No ratings yet
- Parkside Safety Plan 2022Document22 pagesParkside Safety Plan 2022api-250858579No ratings yet
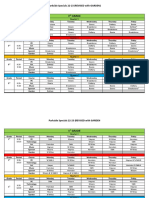
- Specials 22-23 Sy W GardenDocument6 pagesSpecials 22-23 Sy W Gardenapi-250858579No ratings yet
- Thursday CommunicationDocument15 pagesThursday Communicationapi-250858579No ratings yet
- Second Step Log On InstructionsDocument2 pagesSecond Step Log On Instructionsapi-250858579No ratings yet
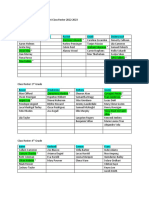
- Rosters Homeroom 2022-2023Document2 pagesRosters Homeroom 2022-2023api-250858579No ratings yet
- 2022-23 Connecting Sel Ib Book of The MonthDocument10 pages2022-23 Connecting Sel Ib Book of The Monthapi-250858579No ratings yet
- Six Traits Anchor Charts 2022Document12 pagesSix Traits Anchor Charts 2022api-250858579No ratings yet
- Fundations Preparation and Implementation 2022Document8 pagesFundations Preparation and Implementation 2022api-250858579No ratings yet
- Comprehensive Barangay Youth Development PlanDocument4 pagesComprehensive Barangay Youth Development PlanIvan KamamangNo ratings yet
- Public Distribution System in IndiaDocument7 pagesPublic Distribution System in IndiaSurhud JoshiNo ratings yet
- PCVL Brgy 1228016 SagnapDocument14 pagesPCVL Brgy 1228016 SagnapAl SimbajonNo ratings yet
- ICDSDocument28 pagesICDSमयंक सिंहNo ratings yet
- 1 Introduction To The Security IndustryDocument6 pages1 Introduction To The Security IndustryAmanpreet Vaseer100% (1)
- Media Law NotesDocument20 pagesMedia Law NotesJambiaNo ratings yet
- April 2016 ElibDocument1,576 pagesApril 2016 ElibTrishia Fernandez GarciaNo ratings yet
- Monitoring in The WorkplaceDocument26 pagesMonitoring in The WorkplaceBerliana SetyawatiNo ratings yet
- Scarlett Al Ansi Letter To School Board 09.18.2020Document5 pagesScarlett Al Ansi Letter To School Board 09.18.2020Jason RantzNo ratings yet
- Syllabus For Criminal Law ReviewDocument18 pagesSyllabus For Criminal Law ReviewMariel Grace Delin0% (1)
- Answer in LEA 100 1CDocument4 pagesAnswer in LEA 100 1Cronaldo juaniNo ratings yet
- GEnder Studies Notes MergedDocument81 pagesGEnder Studies Notes MergedKhadija AftabNo ratings yet
- Prof Ed 2 - Mandatory Child Protection TrainingDocument65 pagesProf Ed 2 - Mandatory Child Protection TrainingFherlene Ruth FelicitasNo ratings yet
- 7-Mental Health WorkplaceDocument16 pages7-Mental Health Workplaceernst rutherfordNo ratings yet
- Introduction To CorrectionDocument5 pagesIntroduction To CorrectionErica Joy RubacNo ratings yet
- Special Penal Laws by Alexis Alcantara UploadDocument3 pagesSpecial Penal Laws by Alexis Alcantara UploadChelsea BayaniNo ratings yet
- Dissertation - Content (Critical Anaylsis of Comepnsation To The Rape VictimsDocument27 pagesDissertation - Content (Critical Anaylsis of Comepnsation To The Rape Victimsshivam5singh-25No ratings yet
- Famines of Bengal 1770,1943Document12 pagesFamines of Bengal 1770,1943Austin GomesNo ratings yet
- Notes On Correctional AdministrationDocument110 pagesNotes On Correctional AdministrationGesler Pilvan SainNo ratings yet
- Unesco School Violence and Bulliyng ReportDocument56 pagesUnesco School Violence and Bulliyng ReportsofiabloemNo ratings yet
- Chase ColemanDocument2 pagesChase ColemanTim KnaussNo ratings yet
- National Women Development PolicyDocument3 pagesNational Women Development PolicyHasan RizviNo ratings yet
- I Have A Dream PresentationDocument20 pagesI Have A Dream Presentationlodee100% (1)
- Child MarriageDocument30 pagesChild Marriagenurauni48No ratings yet
- Genesis Foundation, The Tale of A Family: A Group of Dreamy Youth With A Vision To Change The WorldDocument3 pagesGenesis Foundation, The Tale of A Family: A Group of Dreamy Youth With A Vision To Change The WorldEshraq MostafiNo ratings yet
- Commonwealth Human Rights InitiativeDocument1 pageCommonwealth Human Rights Initiativemyjoyonline.comNo ratings yet
- Policies and Procedure Gym - XEC, LLCDocument2 pagesPolicies and Procedure Gym - XEC, LLCA ThingNo ratings yet
- Abused and Neglected Children FdneDocument26 pagesAbused and Neglected Children FdneRonit ChandNo ratings yet
- Export DocumentDocument11 pagesExport DocumentJoe Bert ButligNo ratings yet
- LGR Curriculum v5-Final-B PDFDocument83 pagesLGR Curriculum v5-Final-B PDFAfrian IndrawanNo ratings yet