You might also like
- CASE STUDY Bronchial AsthmaDocument6 pagesCASE STUDY Bronchial AsthmaRichelle Sandriel C. de Castro86% (22)
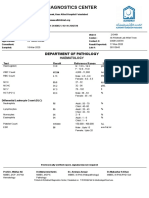
- Al-Khidmat Diagnostics Center: Department of PathologyDocument1 pageAl-Khidmat Diagnostics Center: Department of PathologyKiran HassanNo ratings yet
- Haematology Mcqs For Diploma: Choose The Correct Answer From A - EDocument11 pagesHaematology Mcqs For Diploma: Choose The Correct Answer From A - ESAMMY92% (12)
- COMPLETE BLOOD PICTURE Ok-1 PDFDocument78 pagesCOMPLETE BLOOD PICTURE Ok-1 PDFEmanuel100% (1)
- Vascular Surgery: Current QuestionsFrom EverandVascular Surgery: Current QuestionsAires A. B. Barros D'SaRating: 5 out of 5 stars5/5 (1)
- NS 1 Quiz 7 Sas 19 23Document15 pagesNS 1 Quiz 7 Sas 19 23it's me ANGELANo ratings yet
- BC-5000 English Operator's Manual (7.0) PDFDocument190 pagesBC-5000 English Operator's Manual (7.0) PDFmdk25% (8)
- Manual of Chronic Total Occlusion Percutaneous Coronary Interventions: A Step-by-Step ApproachFrom EverandManual of Chronic Total Occlusion Percutaneous Coronary Interventions: A Step-by-Step ApproachRating: 5 out of 5 stars5/5 (1)
- Computing and Visualization for Intravascular Imaging and Computer-Assisted StentingFrom EverandComputing and Visualization for Intravascular Imaging and Computer-Assisted StentingSimone BaloccoNo ratings yet
- Complications of Chronic Kidney Disease Current STDocument32 pagesComplications of Chronic Kidney Disease Current STmetaNo ratings yet
- AKI Guideline KDIGODocument141 pagesAKI Guideline KDIGOSarah RepinNo ratings yet
- Service Manual: AC 310 Hematology AnalyzerDocument65 pagesService Manual: AC 310 Hematology AnalyzerPhú Nguyễn100% (1)
- Ananya Deb - 18IUT0290004Document26 pagesAnanya Deb - 18IUT0290004subankar NagNo ratings yet
- Incorrected-Ananya Deb - 18IUT0290004Document19 pagesIncorrected-Ananya Deb - 18IUT0290004subankar NagNo ratings yet
- How To Deal With Dialysis Catheter in ICUDocument13 pagesHow To Deal With Dialysis Catheter in ICUjosephNo ratings yet
- Antiplatelet Therapy After Percutaneous Coronary InterventionDocument26 pagesAntiplatelet Therapy After Percutaneous Coronary Interventionnazim bencharifNo ratings yet
- Determinants Influencing Length of Icu Stay in Renal Transplant Recipients Undergoing General AnaesthesiaDocument8 pagesDeterminants Influencing Length of Icu Stay in Renal Transplant Recipients Undergoing General AnaesthesiaIJAR JOURNALNo ratings yet
- Study of Coagulation Profile in Type 2 Diabetes Mellitus Patients in Correlation With Long Term Glycemic Control (Hba1c)Document2 pagesStudy of Coagulation Profile in Type 2 Diabetes Mellitus Patients in Correlation With Long Term Glycemic Control (Hba1c)IJAR JOURNALNo ratings yet
- Bacteremia and Mortality Among Patients With Nontunneled andDocument8 pagesBacteremia and Mortality Among Patients With Nontunneled andFitri AudiniahNo ratings yet
- 2 Cataract Surgery in Diabetes Mellitus A Systematic ReviewDocument10 pages2 Cataract Surgery in Diabetes Mellitus A Systematic ReviewJohn Vargas AgudeloNo ratings yet
- Study of Hemotologicalprofile and Serum Iron Indices in Chronic Kidney Disease in Tertiary Care CentreDocument5 pagesStudy of Hemotologicalprofile and Serum Iron Indices in Chronic Kidney Disease in Tertiary Care CentreIJAR JOURNALNo ratings yet
- HaematologyDocument25 pagesHaematologyAbid KhanNo ratings yet
- WJGS 15 127Document16 pagesWJGS 15 127Octavio GarciaNo ratings yet
- Special Article: Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, ThailandDocument7 pagesSpecial Article: Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, ThailanddefriNo ratings yet
- IraposopemidososDocument9 pagesIraposopemidososjoseNo ratings yet
- s12933 020 01087 4Document12 pagess12933 020 01087 4sarahNo ratings yet
- The Effect of Diabetes Mellitus On Corneal Endothelial Cells and Central Corneal Thickness A Case Control StudyDocument15 pagesThe Effect of Diabetes Mellitus On Corneal Endothelial Cells and Central Corneal Thickness A Case Control Studypramukh prasadNo ratings yet
- Share RateDocument26 pagesShare Ratevirtualpop3No ratings yet
- DOACs in Cirrhotic Patients With Portal Vein Thrombosis - The EvidenceDocument15 pagesDOACs in Cirrhotic Patients With Portal Vein Thrombosis - The EvidencelabertoNo ratings yet
- Dic 1Document6 pagesDic 1Sandra Lusi NovitaNo ratings yet
- Personalized Electrolyte Prescription For Dialysis PatientsDocument13 pagesPersonalized Electrolyte Prescription For Dialysis PatientsSa7arNo ratings yet
- HDA y AntiplaquetariosDocument17 pagesHDA y AntiplaquetariosinarenhdcenNo ratings yet
- Coagulation Dynamics Type 2 Diabetes Mellitus Insights PT APTT AssessmentDocument5 pagesCoagulation Dynamics Type 2 Diabetes Mellitus Insights PT APTT AssessmentSSR-IIJLS JournalNo ratings yet
- JCM 12 06173Document20 pagesJCM 12 06173Taulant MukaNo ratings yet
- AKI and CRRT RelationDocument10 pagesAKI and CRRT RelationZainab MotiwalaNo ratings yet
- 05 N111 39956Document28 pages05 N111 39956Mahruri SaputraNo ratings yet
- Biomedicines 11 03146Document10 pagesBiomedicines 11 03146Andrés HpNo ratings yet
- Chronic Kidney Disease: A Predictive Model Using Decision TreeDocument15 pagesChronic Kidney Disease: A Predictive Model Using Decision TreedadNo ratings yet
- Association Between Systemic Inflammatory Response Index and Left Ventricular Remodeling and Systolic Dysfunction in Atrial Fibrillation PatientsDocument11 pagesAssociation Between Systemic Inflammatory Response Index and Left Ventricular Remodeling and Systolic Dysfunction in Atrial Fibrillation PatientsDr-Ashik RahmanNo ratings yet
- Apport de Lhemodialyse Dans Linsuffisance Renale Aigue Obstructive: Benefices Et RisquesDocument8 pagesApport de Lhemodialyse Dans Linsuffisance Renale Aigue Obstructive: Benefices Et RisquesIJAR JOURNALNo ratings yet
- 2023 ANNALS OF INTENSIVE CARE Mottling As A Prognosis Marker in Cardiogenic ShockDocument13 pages2023 ANNALS OF INTENSIVE CARE Mottling As A Prognosis Marker in Cardiogenic ShockConny MuñozNo ratings yet
- Approach To Emergent Neurotrauma-Related Neurosurgical Procedures in Patients With 2021Document5 pagesApproach To Emergent Neurotrauma-Related Neurosurgical Procedures in Patients With 2021MARIA JOSE MENDOZA AVENDAÑONo ratings yet
- CCRT CovidDocument7 pagesCCRT CovidEdmilson R. LimaNo ratings yet
- Backpropagation Neural Network-Based Machine Learning Model For Prediction of Blood Urea and Glucose in CKD Patients - Health - Med - 2021 - 6454Document8 pagesBackpropagation Neural Network-Based Machine Learning Model For Prediction of Blood Urea and Glucose in CKD Patients - Health - Med - 2021 - 6454droidNo ratings yet
- Applied SciencesDocument20 pagesApplied SciencesFaisalNo ratings yet
- Cardioprotection During Cardiac Surgery: Spotlight ReviewDocument13 pagesCardioprotection During Cardiac Surgery: Spotlight ReviewJorge L Quispe LópezNo ratings yet
- Ivz035Document8 pagesIvz035BEATRIZ CUBILLONo ratings yet
- Eco en SD CardiorenalDocument20 pagesEco en SD Cardiorenaladela pintoNo ratings yet
- Clinical Indications, Treatment and Current PracticeDocument14 pagesClinical Indications, Treatment and Current PracticefadmayulianiNo ratings yet
- Electrolyte Imbalance in CKD PatientsDocument4 pagesElectrolyte Imbalance in CKD PatientsEditor IJTSRDNo ratings yet
- KDIGO 2012 Guidelines de IRADocument141 pagesKDIGO 2012 Guidelines de IRACinara Barros de SáNo ratings yet
- KDIGO AKI Guideline DownloadDocument141 pagesKDIGO AKI Guideline DownloadSandi AuliaNo ratings yet
- Continuous Renal Replacement Therapy Among Patients With COVID-19 and Acute Kidney InjuryDocument8 pagesContinuous Renal Replacement Therapy Among Patients With COVID-19 and Acute Kidney InjuryPIR BanjarmasinNo ratings yet
- A Tertiary Care Hospital's Comparison of Hydronephrosis in An Adult and A Rare CauseDocument4 pagesA Tertiary Care Hospital's Comparison of Hydronephrosis in An Adult and A Rare CauseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- IJAIRneelf 21 PDFDocument14 pagesIJAIRneelf 21 PDFrandaifaNo ratings yet
- Thesis On Acute Coronary SyndromeDocument5 pagesThesis On Acute Coronary Syndromejum1p0tonip3100% (2)
- Niyats Proposal DraftDocument35 pagesNiyats Proposal DraftrobelNo ratings yet
- Pediatric CPBDocument10 pagesPediatric CPBsomaraj kNo ratings yet
- Knowledge, Attitude and Perception of Health Care Workers About Peritoneal Dialysis in Dialysis Center in Westbank, PalestineDocument9 pagesKnowledge, Attitude and Perception of Health Care Workers About Peritoneal Dialysis in Dialysis Center in Westbank, Palestineخالد بن عزيز بن عبدالرحمن حسين خالد بن عزيز بن عبدالرحمن حسينNo ratings yet
- Acute Haemodialysis Clinical GuidelinesDocument16 pagesAcute Haemodialysis Clinical GuidelinesAron PaivaNo ratings yet
- KDIGO Improving CKD Quality of Care - Scope of Work - FinalDocument10 pagesKDIGO Improving CKD Quality of Care - Scope of Work - FinalGEORGINA NIEVES CHOQUETICLLANo ratings yet
- Uncontrolled Donation After Circulatory Death CompDocument9 pagesUncontrolled Donation After Circulatory Death CompKaffal TwoNo ratings yet
- Acute Peritoneal Dialysis in COVID-19Document4 pagesAcute Peritoneal Dialysis in COVID-19Angel SotoNo ratings yet
- My SnopsisDocument30 pagesMy SnopsisaaaaaaaliNo ratings yet
- Manual of STEMI InterventionsFrom EverandManual of STEMI InterventionsSameer MehtaNo ratings yet
- Orientation Schedule 2022Document2 pagesOrientation Schedule 2022subankar NagNo ratings yet
- Self DeclarationDocument1 pageSelf Declarationsubankar NagNo ratings yet
- Payment of 200Document1 pagePayment of 200subankar NagNo ratings yet
- LL Slot BookingDocument1 pageLL Slot Bookingsubankar NagNo ratings yet
- Ananya Deb - 18IUT0290004 - PPTDocument16 pagesAnanya Deb - 18IUT0290004 - PPTsubankar NagNo ratings yet
- SL NO Enrollment NO Name Distnce (KM) Gender Place Form NODocument1 pageSL NO Enrollment NO Name Distnce (KM) Gender Place Form NOsubankar NagNo ratings yet
- Different Types of Energy Piles With Heating Cooling CyclesDocument12 pagesDifferent Types of Energy Piles With Heating Cooling Cyclessubankar NagNo ratings yet
- Indian Institute of Engineering Science and Technology, Shibpur HOWRAH - 711 103Document1 pageIndian Institute of Engineering Science and Technology, Shibpur HOWRAH - 711 103subankar NagNo ratings yet
- Science & Beyond Science Final1Document25 pagesScience & Beyond Science Final1Veeresh M Honnihal100% (2)
- Cell DyneDocument12 pagesCell DyneLia WieNo ratings yet
- Study Guide Lecture Exam 1 Use This Handout With Your Video Review Possible Essay QuestionsDocument4 pagesStudy Guide Lecture Exam 1 Use This Handout With Your Video Review Possible Essay QuestionsBrandice BradleyNo ratings yet
- Full Blood CountDocument3 pagesFull Blood CountStephanie SujanaNo ratings yet
- FORMS Reseta and All Forms 2022 PDFDocument16 pagesFORMS Reseta and All Forms 2022 PDFJessa MaeNo ratings yet
- Hematocrit - StatPearls - NCBI BookshelfDocument4 pagesHematocrit - StatPearls - NCBI BookshelfVincent ReyesNo ratings yet
- Client Package Manual (Magsaysay - WestfalLarsen Management AS)Document8 pagesClient Package Manual (Magsaysay - WestfalLarsen Management AS)Shalinur GonzalesNo ratings yet
- Pancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoDocument6 pagesPancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoYeni PuspitasariNo ratings yet
- Ward ClassDocument7 pagesWard ClassAYESSA JOELLE FOMOKAONo ratings yet
- HematologyonprobioticsDocument7 pagesHematologyonprobioticsMirela CrețuNo ratings yet
- Unicorn: "Cute" "Smart", Yet The Most Powerful 5 Part Differential Hematology Solution ..Document6 pagesUnicorn: "Cute" "Smart", Yet The Most Powerful 5 Part Differential Hematology Solution ..Dharmesh PatelNo ratings yet
- Vet Comparative Oncology - 2022 - Harris - Using Digital RNA Counting To Establish Flow Cytometry Diagnostic Criteria ForDocument10 pagesVet Comparative Oncology - 2022 - Harris - Using Digital RNA Counting To Establish Flow Cytometry Diagnostic Criteria Formarta idziakNo ratings yet
- Operator's Manual: Automated 3-Part Hematology AnalyzerDocument129 pagesOperator's Manual: Automated 3-Part Hematology AnalyzerDani JuhaszNo ratings yet
- Pathophysiology of AllDocument1 pagePathophysiology of AllBGHMC PEDIAHONo ratings yet
- R138911 Amit Kumar 300822180312Document3 pagesR138911 Amit Kumar 300822180312amit kumarNo ratings yet
- NCP Ineffective Tissue PerfusionDocument4 pagesNCP Ineffective Tissue PerfusionSteffiNo ratings yet
- B.Sc. MicrobiologyDocument38 pagesB.Sc. MicrobiologyelaiyarajaNo ratings yet
- Erythematous Throat and Tonsils. Swollen Cervical Lymph NodesDocument32 pagesErythematous Throat and Tonsils. Swollen Cervical Lymph NodesDr.Kuntal PatelNo ratings yet
- 10 BloodDocument20 pages10 BloodEr Nitin SinghNo ratings yet
- Questions With Answers PDF - 231017 - 100634Document27 pagesQuestions With Answers PDF - 231017 - 100634chedielnyagawaNo ratings yet
- Klubsybear Additional Recalls: Hematology A.karyolysisDocument2 pagesKlubsybear Additional Recalls: Hematology A.karyolysisMartin ClydeNo ratings yet
- 2022 Nutrition & Blood DisordersDocument30 pages2022 Nutrition & Blood DisordersDietary EamcNo ratings yet
- Complete Blood CountDocument5 pagesComplete Blood CountShella CondezNo ratings yet