You might also like
- Ebook First Aid For The Psychiatry Clerkship Sixth Edition PDF Full Chapter PDFDocument59 pagesEbook First Aid For The Psychiatry Clerkship Sixth Edition PDF Full Chapter PDFgwendolyn.jordan28397% (31)
- Soap Notes AsthmaDocument6 pagesSoap Notes AsthmaCHRISTINE KARENDINo ratings yet
- Applied Pharma (NLE)Document2 pagesApplied Pharma (NLE)Maginalyn CangasNo ratings yet
- Case Study of SVIDocument27 pagesCase Study of SVICristina100% (1)
- Crossm: Descriptive, Retrospective Study of The Clinical Characteristics of Asymptomatic COVID-19 PatientsDocument11 pagesCrossm: Descriptive, Retrospective Study of The Clinical Characteristics of Asymptomatic COVID-19 PatientsYogi Sampe PasangNo ratings yet
- Journal Pone 0249090Document11 pagesJournal Pone 0249090Syed Rehan AghaNo ratings yet
- Coronavirus Disease 2019 (COVID-19)Document27 pagesCoronavirus Disease 2019 (COVID-19)Mateus SchulzNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - UpToDateDocument43 pagesCoronavirus Disease 2019 (COVID-19) - UpToDateGloria MiramontesNo ratings yet
- Crossm: Descriptive, Retrospective Study of The Clinical Characteristics of Asymptomatic COVID-19 PatientsDocument11 pagesCrossm: Descriptive, Retrospective Study of The Clinical Characteristics of Asymptomatic COVID-19 PatientsdariusNo ratings yet
- The Epidemiology and Pathogenesis of Coronavirus Disease Covid 19 Outbreak Hussin A Rothan Download 2024 Full ChapterDocument26 pagesThe Epidemiology and Pathogenesis of Coronavirus Disease Covid 19 Outbreak Hussin A Rothan Download 2024 Full Chapterbertha.harriman873100% (13)
- Novel Coronavirus Infection (Covid-19) Basic GuideDocument9 pagesNovel Coronavirus Infection (Covid-19) Basic GuideSamanNo ratings yet
- The Management of Coronavirus Disease 2019 (COVID 19) : Jialin Liu - Siru LiuDocument7 pagesThe Management of Coronavirus Disease 2019 (COVID 19) : Jialin Liu - Siru LiuFina RepitiyanaNo ratings yet
- Jurnal 3Document8 pagesJurnal 3kalstarNo ratings yet
- Immune Response To Sars-Cov-2 and Mechanisms of Immunopathological Changes in Covid-19Document18 pagesImmune Response To Sars-Cov-2 and Mechanisms of Immunopathological Changes in Covid-19Ayu MayangsariNo ratings yet
- Jurnal 6Document2 pagesJurnal 6kalstarNo ratings yet
- Uptodate - Coronavirus Epi, PreventionDocument55 pagesUptodate - Coronavirus Epi, PreventionAlexRázuriNo ratings yet
- Corona Virus DiseaseDocument6 pagesCorona Virus DiseaseSAKET MEHTANo ratings yet
- An Update On COVID 19 Pandemic The Epidemiology Pathogenesis Prevention and Treatment Strategies (Important)Document13 pagesAn Update On COVID 19 Pandemic The Epidemiology Pathogenesis Prevention and Treatment Strategies (Important)ayoubNo ratings yet
- Covid19 PDFDocument40 pagesCovid19 PDFMan Hong SoNo ratings yet
- Epidemiologia e Características Clínicas Do COVID 19 Uma RevisãoDocument7 pagesEpidemiologia e Características Clínicas Do COVID 19 Uma RevisãoFulano de TalNo ratings yet
- WHO Declares COVID-19 A Pandemic: Domenico Cucinotta, Maurizio VanelliDocument4 pagesWHO Declares COVID-19 A Pandemic: Domenico Cucinotta, Maurizio VanelliNessa Dila AnandaNo ratings yet
- Update 28 Covid 19 What We Know May 2020Document18 pagesUpdate 28 Covid 19 What We Know May 2020Mohammed ImenksNo ratings yet
- Yi WU 2022Document9 pagesYi WU 2022suieny.rodriguesNo ratings yet
- Epidemiology and Clinical Characteristics of COVID-19: MedicineDocument4 pagesEpidemiology and Clinical Characteristics of COVID-19: MedicineAlexRázuriNo ratings yet
- Diagnosis, Treatment, and Prevention of 2019 Novel Coronavirus Infection in Children: Experts' Consensus StatementDocument10 pagesDiagnosis, Treatment, and Prevention of 2019 Novel Coronavirus Infection in Children: Experts' Consensus StatementBaiq DysaNo ratings yet
- Covid-19 in South Korea - Challenges of Subclinical ManifestationsDocument2 pagesCovid-19 in South Korea - Challenges of Subclinical ManifestationsSuwandi ChangNo ratings yet
- Novel CoronavirusDocument7 pagesNovel CoronavirusMustafa KhudhairNo ratings yet
- Clinical Outcomes and Immunologic Characteristics of Coronavirus Disease 2019 in People With Human Immunodeficiency VirusDocument6 pagesClinical Outcomes and Immunologic Characteristics of Coronavirus Disease 2019 in People With Human Immunodeficiency VirusanaNo ratings yet
- Velavan Et Al-2020-Tropical Medicine International HealthDocument4 pagesVelavan Et Al-2020-Tropical Medicine International Healthjunior rodriguesNo ratings yet
- MelianaEclesiaManurung - 4172121028 - BilingualPhysics17 - Paper - Breakthrough of COVID 19 Using Radiotherapy Treatment Modalites - Gamma RaysDocument6 pagesMelianaEclesiaManurung - 4172121028 - BilingualPhysics17 - Paper - Breakthrough of COVID 19 Using Radiotherapy Treatment Modalites - Gamma RaysmelianaeclsNo ratings yet
- 04 OFIDHighdose IVIGasatherapeuticoptionDocument7 pages04 OFIDHighdose IVIGasatherapeuticoptionmy accountNo ratings yet
- Natureofepidemic, COVID-19 FinalDocument19 pagesNatureofepidemic, COVID-19 FinalSam SezNo ratings yet
- 10 1056@NEJMe2002387 PDFDocument2 pages10 1056@NEJMe2002387 PDFAlbert Andía MamaniNo ratings yet
- 10 1056@NEJMe2002387 PDFDocument2 pages10 1056@NEJMe2002387 PDFAlbert Andía MamaniNo ratings yet
- 10 1056@NEJMe2002387 PDFDocument2 pages10 1056@NEJMe2002387 PDFAlbert Andía MamaniNo ratings yet
- Nosocomial Infection of COVID 19: A New Challenge For Healthcare Professionals (Review)Document10 pagesNosocomial Infection of COVID 19: A New Challenge For Healthcare Professionals (Review)lagi magerNo ratings yet
- Immunology - 2022 - Chen - New Onset Autoimmune Phenomena Post COVID 19 Vaccination-1Document17 pagesImmunology - 2022 - Chen - New Onset Autoimmune Phenomena Post COVID 19 Vaccination-1Ivan StojanovicNo ratings yet
- MainDocument7 pagesMainM ANo ratings yet
- Etiologi-Patofisioloy COVID-19Document12 pagesEtiologi-Patofisioloy COVID-19hening ciptiany pertiwyNo ratings yet
- Ciaa 247Document6 pagesCiaa 247berlian gurningNo ratings yet
- JCMM 24 6558Document13 pagesJCMM 24 6558Roberto D. GarceteNo ratings yet
- PB DikonversiDocument18 pagesPB DikonversiAhmadNo ratings yet
- Age-Dependent Risks of Incidence and Mortality of COVID-19 in Hubei Province and Other Parts of ChinaDocument6 pagesAge-Dependent Risks of Incidence and Mortality of COVID-19 in Hubei Province and Other Parts of ChinaAnugerahIndahMarethaNo ratings yet
- Evidence For Pre-Symptomatic Transmission of Coronavirus Disease 2019 (COVID-19) in ChinaDocument8 pagesEvidence For Pre-Symptomatic Transmission of Coronavirus Disease 2019 (COVID-19) in ChinaFatrina Maha DewiNo ratings yet
- Investigatory Project Sample SurveyDocument65 pagesInvestigatory Project Sample SurveySnekha TNo ratings yet
- Coronavirus Disease 2019 (COVID-19) A Perspective From ChinaDocument29 pagesCoronavirus Disease 2019 (COVID-19) A Perspective From ChinabackupNo ratings yet
- Koodak PDFDocument9 pagesKoodak PDFHugoMarcelo77No ratings yet
- Coronavirus (COVID-19) Outbreak: What The Department of Endoscopy Should KnowDocument6 pagesCoronavirus (COVID-19) Outbreak: What The Department of Endoscopy Should KnowswabrijNo ratings yet
- Corona Virus 2019Document11 pagesCorona Virus 2019Jonille EchevarriaNo ratings yet
- Clinical Immunology: Koichi Yuki, Miho Fujiogi, Sophia Koutsogiannaki TDocument7 pagesClinical Immunology: Koichi Yuki, Miho Fujiogi, Sophia Koutsogiannaki TishmahNo ratings yet
- COVID-19 - Clinical Features - UpToDateDocument27 pagesCOVID-19 - Clinical Features - UpToDateDuy Hùng HoàngNo ratings yet
- Coronavirus (2019 Ncov) Selected Bibliographic References 12 02 2020 v1Document6 pagesCoronavirus (2019 Ncov) Selected Bibliographic References 12 02 2020 v1Andi SanapatiNo ratings yet
- 2019 Coronavirus Disease (COVID-19) Outbreak: A Review ArticleDocument6 pages2019 Coronavirus Disease (COVID-19) Outbreak: A Review ArticleMelakuNo ratings yet
- English Papers: "Corona Virus (Covid-19) "Document15 pagesEnglish Papers: "Corona Virus (Covid-19) "Deliana MonizNo ratings yet
- A Review On Immunopathogenesis, Molecular Biology and Clinical Aspects of The 2019 Novel Coronavirus (COVID-19)Document14 pagesA Review On Immunopathogenesis, Molecular Biology and Clinical Aspects of The 2019 Novel Coronavirus (COVID-19)fer ferNo ratings yet
- Type 1 Diabetes Triggered by Covid-19 Pandemic A Potential OutbreakDocument3 pagesType 1 Diabetes Triggered by Covid-19 Pandemic A Potential OutbreaksamuelNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Nurseslabs PDFDocument21 pagesCoronavirus Disease 2019 (COVID-19) - Nurseslabs PDFSanket TelangNo ratings yet
- Vaccines For COVID-19 - The Current State of Play PDFDocument8 pagesVaccines For COVID-19 - The Current State of Play PDFdiana.alyNo ratings yet
- On A Knife's Edge of A COVID-19 Pandemic: Is Containment Still Possible?Document5 pagesOn A Knife's Edge of A COVID-19 Pandemic: Is Containment Still Possible?BobanBisercicNo ratings yet
- تقرير وبائياتDocument6 pagesتقرير وبائياتMustafa KhudhairNo ratings yet
- Covid UpdateDocument25 pagesCovid UpdateAndreea PostolacheNo ratings yet
- Asymptomatic Carrier State Acute Respiratory Disease and Pneumonia Due To Severe Acute Respiratory Syndrome Coronavirus 2 Sars Cov 2 Facts and Myths Chih Cheng Lai Download 2024 Full ChapterDocument32 pagesAsymptomatic Carrier State Acute Respiratory Disease and Pneumonia Due To Severe Acute Respiratory Syndrome Coronavirus 2 Sars Cov 2 Facts and Myths Chih Cheng Lai Download 2024 Full Chaptertyrone.cruz893100% (12)
- Neonatal Covid 19 Exposures and Infections A Systematic Review of Modes of Transmission Manifestations and ManagementDocument18 pagesNeonatal Covid 19 Exposures and Infections A Systematic Review of Modes of Transmission Manifestations and ManagementadeNo ratings yet
- COVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsFrom EverandCOVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsNo ratings yet
- Antivitamins For Medicinal Applications: DOI: 10.1002/cbic.201500072Document15 pagesAntivitamins For Medicinal Applications: DOI: 10.1002/cbic.201500072Delfina RubioNo ratings yet
- 2018 Article 1448Document18 pages2018 Article 1448Delfina RubioNo ratings yet
- Travel Medicine and Infectious Disease: Contents Lists Available atDocument13 pagesTravel Medicine and Infectious Disease: Contents Lists Available atDelfina RubioNo ratings yet
- Covid 19 Patients' Clinical Characteristics, Discharge Rate, and Fatality Rate of Meta AnalysisDocument7 pagesCovid 19 Patients' Clinical Characteristics, Discharge Rate, and Fatality Rate of Meta AnalysisDelfina RubioNo ratings yet
- Depression in IndiaDocument50 pagesDepression in IndiaVignesh BalaNo ratings yet
- Millon Clinical Multiaxial Inventory IIIDocument16 pagesMillon Clinical Multiaxial Inventory IIIJhoana Bello100% (2)
- FunxionDocument1 pageFunxionEllain CaballeroNo ratings yet
- JEE Main, JEE Advanced, CBSE, NEET, IIT, Free Study Packages, Test Papers, Counselling, Ask ExpertsDocument13 pagesJEE Main, JEE Advanced, CBSE, NEET, IIT, Free Study Packages, Test Papers, Counselling, Ask ExpertsDevil SidhuNo ratings yet
- Maria Angeline Mendoza BSN 3a2 - Communicable Disease StudyDocument17 pagesMaria Angeline Mendoza BSN 3a2 - Communicable Disease StudyAiram Enilegna AzodnemNo ratings yet
- Outline of Lecture On Mental Health and IllnessDocument14 pagesOutline of Lecture On Mental Health and IllnessMahasiwa RebahanNo ratings yet
- Telemedicine PDFDocument8 pagesTelemedicine PDFBenjamin YokeshNo ratings yet
- Covid-19 Is A Deception - Here's WhyDocument31 pagesCovid-19 Is A Deception - Here's WhyFaiezNo ratings yet
- Current Concepts in Ischemic Hepatitis.9Document6 pagesCurrent Concepts in Ischemic Hepatitis.9Anabel GonzalezNo ratings yet
- Product Brochure - Lunit INSIGHT CXRDocument16 pagesProduct Brochure - Lunit INSIGHT CXRDebora NunesNo ratings yet
- The The Various Communicative Methods Practiced by Animals in The WildDocument2 pagesThe The Various Communicative Methods Practiced by Animals in The WildAmutha AmmuNo ratings yet
- Cure For VertigoDocument6 pagesCure For VertigoPraveen KumarNo ratings yet
- Motion For Telephonic Appearance - Abogado Jose - Wendy Karina RAMIREZ MENDEZ - 10-23-2020Document5 pagesMotion For Telephonic Appearance - Abogado Jose - Wendy Karina RAMIREZ MENDEZ - 10-23-2020TuttiUribeNo ratings yet
- Chapter2 Template Group 1Document8 pagesChapter2 Template Group 1Alessa LamesNo ratings yet
- Revision - Why Do We Fall Ill NotesDocument15 pagesRevision - Why Do We Fall Ill NotesAtharva VarshneyNo ratings yet
- Autoimmune EbookDocument11 pagesAutoimmune EbookIndra LuftiNo ratings yet
- Mcqs DDDocument15 pagesMcqs DDIjaz KhanNo ratings yet
- Sympathetic Agonist and Antagonist 23Document12 pagesSympathetic Agonist and Antagonist 23PNo ratings yet
- M1 - Midnight's BloodDocument50 pagesM1 - Midnight's BloodTsuryth TsuNo ratings yet
- Laboratory Diagnosis of Hepatobiliary Disease BCCMDocument65 pagesLaboratory Diagnosis of Hepatobiliary Disease BCCMMeghana MaddaliNo ratings yet
- Evening Primrose (Oenothera Biennis) Oil in Management of Female AilmentsDocument9 pagesEvening Primrose (Oenothera Biennis) Oil in Management of Female AilmentsThùy LinhNo ratings yet
- MurmursDocument5 pagesMurmursAlexander G. Álvarez RojasNo ratings yet
- HSE AwarenessDocument209 pagesHSE Awarenesstariq19870% (1)
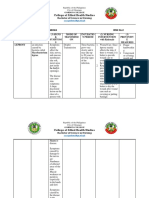
- Family Nursing Care PlanDocument5 pagesFamily Nursing Care PlanMarlchiel Nathan ArregladoNo ratings yet
- Jurnal ParuDocument8 pagesJurnal ParuM Rizal Hermawan PNo ratings yet
- Latent Tuberculosis Infection NejmDocument10 pagesLatent Tuberculosis Infection Nejmpogesil46No ratings yet