You might also like
- Text A: Part A: Texts A - DDocument7 pagesText A: Part A: Texts A - Danilrajputlive100% (1)
- Head injuries management guideDocument7 pagesHead injuries management guideNars Oet MateryalesNo ratings yet
- Head Injury Management of PediatricDocument22 pagesHead Injury Management of PediatricIrma KusumaNo ratings yet
- Erm - All Files in OneDocument213 pagesErm - All Files in OneBryan GCNo ratings yet
- PREDICTALGORITHM v1 1 29.01.21Document2 pagesPREDICTALGORITHM v1 1 29.01.21selvi zhafirahNo ratings yet
- TEC Escala Glasgow Trauma CraneoencefálicoDocument42 pagesTEC Escala Glasgow Trauma CraneoencefálicoJenny Lopez BocangelNo ratings yet
- ENT Handbook: The Master Surgeon TrustDocument16 pagesENT Handbook: The Master Surgeon TrustSabyasachi MukhopadhyayNo ratings yet
- Management of A Head InjuryDocument10 pagesManagement of A Head InjuryEiYzwan SYahNo ratings yet
- Paediatric NotesDocument76 pagesPaediatric NotesaminaNo ratings yet
- Head Injury and Role of Anaesthesiologist in ManagementDocument38 pagesHead Injury and Role of Anaesthesiologist in ManagementDeepak SolankiNo ratings yet
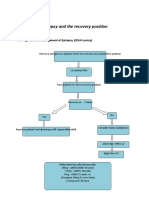
- Epilepsy Recovery Period - Second YrDocument3 pagesEpilepsy Recovery Period - Second YrBrian MaloneyNo ratings yet
- Sample Medical Guidelines: Pediatric SeizureDocument2 pagesSample Medical Guidelines: Pediatric SeizureJohn PerezNo ratings yet
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3No ratings yet
- Powered byDocument25 pagesPowered byAditi ParmarNo ratings yet
- Long Quiz RegodosDocument4 pagesLong Quiz RegodosIan Cyrus RegodosNo ratings yet
- 002 Performing The Glasgow Coma Scale Students 1Document6 pages002 Performing The Glasgow Coma Scale Students 1SHAINA CADALINNo ratings yet
- Head InjuryDocument88 pagesHead InjuryPrisca Angelina100% (2)
- NSO Glasgow Coma ScaleDocument3 pagesNSO Glasgow Coma Scaleanon_657718264No ratings yet
- Physiotherapy management in unconscious TBI patientsDocument28 pagesPhysiotherapy management in unconscious TBI patientsSaurav NeupaneNo ratings yet
- TRAUMATIC BRAIN INJURY MEDICAL SURGICAL NURSINGDocument48 pagesTRAUMATIC BRAIN INJURY MEDICAL SURGICAL NURSINGErica Keil MoleNo ratings yet
- UncounsionessDocument17 pagesUncounsionessElijah MagaiwaNo ratings yet
- PediatricseizureDocument2 pagesPediatricseizureRifrita Fransisca HalimNo ratings yet
- PEDIA Assessment NEURODocument12 pagesPEDIA Assessment NEUROEncee MianNo ratings yet
- PVD Prep U. Chapter 27 Study Guide for Cardiac NursingDocument5 pagesPVD Prep U. Chapter 27 Study Guide for Cardiac NursingMonica JubaneNo ratings yet
- W5 - MEDSURG Neurologic Disorders (Bell's Palsy, GBS, Trigeminal Neuralgia)Document9 pagesW5 - MEDSURG Neurologic Disorders (Bell's Palsy, GBS, Trigeminal Neuralgia)Kyla L. Madjad100% (1)
- ATLS Chapter Review QuestionsDocument36 pagesATLS Chapter Review QuestionsKen Evans89% (57)
- TMS Safety ChecklistDocument4 pagesTMS Safety Checklistyaang yuliana ciptaNo ratings yet
- Diagnosing and Managing MigrainesDocument41 pagesDiagnosing and Managing MigrainesmichaelwillsonNo ratings yet
- Bells Palsy or Stroke 02.06.2019Document19 pagesBells Palsy or Stroke 02.06.2019Emily EresumaNo ratings yet
- Emergency Room Medicine Notes ATFDocument192 pagesEmergency Room Medicine Notes ATFGiovanna Moller100% (3)
- Headache Syndromes Presentation Dr. TarekDocument50 pagesHeadache Syndromes Presentation Dr. TarekHero StoreNo ratings yet
- Glasgow Coma Scale and Causes of ComaDocument6 pagesGlasgow Coma Scale and Causes of ComaEm Hernandez AranaNo ratings yet
- Neurosensory Disorders: Symptoms, Tests, and Nursing CareDocument13 pagesNeurosensory Disorders: Symptoms, Tests, and Nursing CarePaul Lexus Gomez LorenzoNo ratings yet
- Procedure Sick Bay 2017Document6 pagesProcedure Sick Bay 2017Syed FareedNo ratings yet
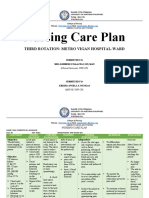
- Nursing Care Plan: Third Rotation: Metro Vigan Hospital-WardDocument5 pagesNursing Care Plan: Third Rotation: Metro Vigan Hospital-WardKrizha Angela NicolasNo ratings yet
- Cerebral Trauma: AKA Traumatic Brain InjuryDocument15 pagesCerebral Trauma: AKA Traumatic Brain InjuryAlison ThorpeNo ratings yet
- Neurologic Disorder PostDocument8 pagesNeurologic Disorder PostGwenn SalazarNo ratings yet
- Bell's Palsy: Submitted By: Twinkle Singh & Kinjalika VarmaDocument34 pagesBell's Palsy: Submitted By: Twinkle Singh & Kinjalika Varmatwinklestar1396No ratings yet
- Neurology Questions & Answers: Management and DiagnosisDocument58 pagesNeurology Questions & Answers: Management and DiagnosisMonica J Ortiz Pereira100% (2)
- Evaluating The Neurologic Status of Unconscious PatientDocument3 pagesEvaluating The Neurologic Status of Unconscious Patientsambel_88No ratings yet
- Patient Management Problem Preferred Responses.27Document12 pagesPatient Management Problem Preferred Responses.27mhd.mamdohNo ratings yet
- Headache History and Diagnosis GuideDocument7 pagesHeadache History and Diagnosis GuideLeilia FibrianasariNo ratings yet
- GUIDELINE TCE PEDDocument9 pagesGUIDELINE TCE PEDcarolgc99No ratings yet
- Lady Diane CabrigaDocument34 pagesLady Diane CabrigaDayan Cabriga100% (1)
- Question ID Title Last Revision: Page 30) Page 32)Document4 pagesQuestion ID Title Last Revision: Page 30) Page 32)AnisulHaqueNo ratings yet
- What Is A Febrile ConvulsionDocument14 pagesWhat Is A Febrile ConvulsionJazendra TootNo ratings yet
- A ZHealthDocument3 pagesA ZHealthDaut DervishoskiNo ratings yet
- Questions To Ask When Answering OMFS BleepDocument4 pagesQuestions To Ask When Answering OMFS BleepNeelam Rathod MehtaNo ratings yet
- Lumbar Puncture GuidelinesDocument6 pagesLumbar Puncture GuidelinesYwagar YwagarNo ratings yet
- Causes and Components of Consciousness and UnconsciousnessDocument102 pagesCauses and Components of Consciousness and UnconsciousnessHardeep KaurNo ratings yet
- Patient Management Problem.29Document6 pagesPatient Management Problem.29مجاهد إسماعيل حسن حسينNo ratings yet
- NCM 104 Midterm ExamDocument22 pagesNCM 104 Midterm ExammalindaNo ratings yet
- 03 NeurologyDocument34 pages03 Neurologyfire_n_iceNo ratings yet
- Head Injury Admission To Bservation NIT: Xclusion RiteriaDocument3 pagesHead Injury Admission To Bservation NIT: Xclusion RiteriaTONY GO AWAYNo ratings yet
- Coma, (Unconsciousness) A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandComa, (Unconsciousness) A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Heart of the Field "Refresher & Nha Certification Quick Notes"From EverandHeart of the Field "Refresher & Nha Certification Quick Notes"No ratings yet
- Ice Cream Headache, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIce Cream Headache, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- ATLS-9e Tetanus PDFDocument2 pagesATLS-9e Tetanus PDFAroell KriboNo ratings yet
- Biology Form 4 Chapter 6 NutritionDocument5 pagesBiology Form 4 Chapter 6 NutritionzaedmohdNo ratings yet
- 4 Hour BodyDocument20 pages4 Hour BodyHealingForLifeNo ratings yet
- NIH Low Iodine Diet For Nuclear MedDocument8 pagesNIH Low Iodine Diet For Nuclear MedderekcftamNo ratings yet
- 02 Community Organizaing - The RationaleDocument15 pages02 Community Organizaing - The RationaleValerie Estrella100% (1)
- James Andretich Resume #2Document2 pagesJames Andretich Resume #2Abbey DavisNo ratings yet
- Accredited Clinic As of April 2018 PDFDocument64 pagesAccredited Clinic As of April 2018 PDFBelteshazzarL.CabacangNo ratings yet
- BARANGAY TrainingDocument2 pagesBARANGAY TrainingAngel BenateroNo ratings yet
- The Tell-Tale Heart by Edgar Allan PoeDocument21 pagesThe Tell-Tale Heart by Edgar Allan PoeDavid Con RiveroNo ratings yet
- HOPE 1 - Exercise For FitnessDocument3 pagesHOPE 1 - Exercise For FitnessReàgan Buela II0% (1)
- Risk factors for autism linked to genderDocument14 pagesRisk factors for autism linked to gendermacarenavNo ratings yet
- Tongue Tie 2016Document6 pagesTongue Tie 2016drchiNo ratings yet
- Norms, Policies and Protocols of Pediatric CareDocument49 pagesNorms, Policies and Protocols of Pediatric CareSivabarathy86% (14)
- Assessment and Diagnosis of StrokeDocument34 pagesAssessment and Diagnosis of StrokeMohd Khateeb100% (1)
- Fat-Containing Liver Lesions On Imaging: Detection and Differential DiagnosisDocument10 pagesFat-Containing Liver Lesions On Imaging: Detection and Differential DiagnosisOana AndreeaNo ratings yet
- Local - Media2196001544712081207 1 1 2Document60 pagesLocal - Media2196001544712081207 1 1 2jaymar gervacioNo ratings yet
- Volume 48, Issue 49, December 5, 2014Document43 pagesVolume 48, Issue 49, December 5, 2014BladeNo ratings yet
- Drug Calculations 2015Document35 pagesDrug Calculations 2015Anonymous DWMeAjhD1cNo ratings yet
- Public Health Nutrition Career OptionsDocument2 pagesPublic Health Nutrition Career OptionsZaka RehmanNo ratings yet
- Guidelines On The Biggest Loser Contest Among Government Employees of Central LuzonDocument20 pagesGuidelines On The Biggest Loser Contest Among Government Employees of Central LuzonChix LasundinNo ratings yet
- T-Nation Yoke TrainingDocument11 pagesT-Nation Yoke TrainingJoseph Glaser100% (1)
- Movement Disorders: Akinetic-Rigid SyndromesDocument8 pagesMovement Disorders: Akinetic-Rigid SyndromesMarwan M.No ratings yet
- DHS Baltimore Freddie Gray Protest DocumentsDocument773 pagesDHS Baltimore Freddie Gray Protest DocumentsJason Leopold100% (1)
- PSORIASISDocument9 pagesPSORIASISDianne BernardoNo ratings yet
- Handbook (Chemistry Workshop)Document34 pagesHandbook (Chemistry Workshop)DocsNo ratings yet
- The Journal of Torah and Medicine of The Albert Einstein College of Medicine Synagogue and RIETSDocument160 pagesThe Journal of Torah and Medicine of The Albert Einstein College of Medicine Synagogue and RIETSoutdash2No ratings yet
- Business Communication: Dabur India LTDDocument30 pagesBusiness Communication: Dabur India LTDshashank nutiNo ratings yet
- Concrete Pouring & Compacting MethodDocument18 pagesConcrete Pouring & Compacting MethodDragu SorinNo ratings yet
- HEALTH AND NUTRITION: WEIGHT MANAGEMENTDocument29 pagesHEALTH AND NUTRITION: WEIGHT MANAGEMENTJuhany MusaNo ratings yet
- Buku Kerja Guru 3Document15 pagesBuku Kerja Guru 3ismail salehNo ratings yet