You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- NCP-Risk For InjuryDocument1 pageNCP-Risk For InjuryLave Majorenos80% (10)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Amc MCQ PDFDocument48 pagesAmc MCQ PDFSohaib Zafar50% (2)
- LVAD in An Hbo2 ChamberDocument5 pagesLVAD in An Hbo2 ChamberTony LeeNo ratings yet
- Osteoarthritis Concept MapDocument1 pageOsteoarthritis Concept Mapashleydean67% (3)
- Topical Oxygen Wound TherapyDocument9 pagesTopical Oxygen Wound TherapyTony LeeNo ratings yet
- Air Vs Oxygen in STEMPDocument8 pagesAir Vs Oxygen in STEMPTony LeeNo ratings yet
- Hbo2 Abt SystemDocument7 pagesHbo2 Abt SystemTony LeeNo ratings yet
- Hbo2 and RedoxDocument9 pagesHbo2 and RedoxTony LeeNo ratings yet
- Lactate Accumulation in Apneic SportsDocument9 pagesLactate Accumulation in Apneic SportsTony LeeNo ratings yet
- Waist Hip Ratio or CV RiskDocument1 pageWaist Hip Ratio or CV RiskTony LeeNo ratings yet
- Transcutaneous Oximetry in Clin Practice - ConsensusDocument11 pagesTranscutaneous Oximetry in Clin Practice - ConsensusTony LeeNo ratings yet
- Hematology VenipunctureDocument1 pageHematology VenipuncturecassseeeyyyNo ratings yet
- Emergency Psychiatry Other Than Suicide: Dr. Pooja Singh, MD Assistant ProfessorDocument45 pagesEmergency Psychiatry Other Than Suicide: Dr. Pooja Singh, MD Assistant Professorpooja singhNo ratings yet
- JCRC 19 010TangoTherapy02 2019 01Document5 pagesJCRC 19 010TangoTherapy02 2019 01Csongor KicsiNo ratings yet
- Making Occlusion 2Document7 pagesMaking Occlusion 2Ali QawasNo ratings yet
- Policies & Procedures Manual: Anesthesia & Surgery CommitteeDocument3 pagesPolicies & Procedures Manual: Anesthesia & Surgery CommitteeEsamNo ratings yet
- Modalities of Cancer TreatmentDocument65 pagesModalities of Cancer TreatmentBspharma 2E100% (1)
- A Case Study in Marburg Hemorrhagic Fever - MicrobiologyDocument1 pageA Case Study in Marburg Hemorrhagic Fever - MicrobiologyAnna PriskaNo ratings yet
- Truncus ArteriosusDocument19 pagesTruncus ArteriosusHijaz Al-YamanNo ratings yet
- (Anatomy) Chapter 12 - Lymphatic SystemDocument71 pages(Anatomy) Chapter 12 - Lymphatic SystemJezreel Mian A. LacsonNo ratings yet
- Fractures: Types, Complications, and ManagementDocument26 pagesFractures: Types, Complications, and Managementsm - kardmNo ratings yet
- Demodectic Mange and Inexpensive TreatmentDocument3 pagesDemodectic Mange and Inexpensive Treatmentcigar77No ratings yet
- CHN 4 RCDocument11 pagesCHN 4 RCMarga AlvarezNo ratings yet
- Nursing Health History ReyDocument10 pagesNursing Health History ReyNikki MarieNo ratings yet
- Staphylococcus Aureus Research PaperDocument6 pagesStaphylococcus Aureus Research Paperisvgmchkf100% (1)
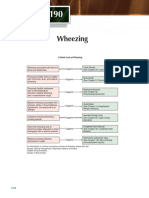
- Wheezing: A Quick Look at WheezingDocument1 pageWheezing: A Quick Look at WheezingpelinNo ratings yet
- 02 MenangitisDocument4 pages02 MenangitisMaeen Gamal AlhadhramiNo ratings yet
- DS CD34 MicroBead Kit HDocument4 pagesDS CD34 MicroBead Kit Hsankalpa3No ratings yet
- Sexual Reproduction in Humans: Chapter - I Reproduction SystemsDocument18 pagesSexual Reproduction in Humans: Chapter - I Reproduction Systemsrajendra110778No ratings yet
- Intra-Abdominal Hypertension: Andrew William L. AquinoDocument15 pagesIntra-Abdominal Hypertension: Andrew William L. AquinoEdelrose LapitanNo ratings yet
- Lecture N4 Breast-Feeding. Value and Advantages of Breast-Feeding. Methods of Calculation of Daily Volume of Feeding. Weaning at Breast FeedingDocument7 pagesLecture N4 Breast-Feeding. Value and Advantages of Breast-Feeding. Methods of Calculation of Daily Volume of Feeding. Weaning at Breast FeedingAVINASH PvkNo ratings yet
- Artesunate Uses, Side Effects & WarningsDocument3 pagesArtesunate Uses, Side Effects & Warningstarun yadavNo ratings yet
- DR Romila Chimoriya Lecturer Department of Pediatrics: Acute Rheumatic FeverDocument27 pagesDR Romila Chimoriya Lecturer Department of Pediatrics: Acute Rheumatic FeverDhiraj PantNo ratings yet
- Chapter 8Document89 pagesChapter 8Harith AtrisNo ratings yet
- ENT (Revised)Document6 pagesENT (Revised)Tanishka KoyandeNo ratings yet
- ISHRS 21st Abstract Book 2013 SanFran DR Alan Bauman FinalDocument542 pagesISHRS 21st Abstract Book 2013 SanFran DR Alan Bauman FinalAlan J Bauman MDNo ratings yet
- Cardiovascular DiseaseDocument73 pagesCardiovascular DiseaseAli SherNo ratings yet