You might also like
- Biology for Students: The Only Biology Study Guide You'll Ever Need to Ace Your CourseFrom EverandBiology for Students: The Only Biology Study Guide You'll Ever Need to Ace Your CourseNo ratings yet
- Chapter 3 For Animal SCDocument37 pagesChapter 3 For Animal SCRediat GossayeNo ratings yet
- Infection and ImmunityDocument68 pagesInfection and ImmunityWilliam EwingNo ratings yet
- VirusesDocument30 pagesVirusesJamila AragonNo ratings yet
- Viruses: Shafie Abdulkadir HassanDocument29 pagesViruses: Shafie Abdulkadir HassanShafici CqadirNo ratings yet
- Virus PDFDocument60 pagesVirus PDFrenz bartolomeNo ratings yet
- Viral CNS Infections - Polio, Rabies Group PresentationDocument49 pagesViral CNS Infections - Polio, Rabies Group Presentationodhiambo samwelNo ratings yet
- PNVL Biological Science Lecture on VirusesDocument3 pagesPNVL Biological Science Lecture on VirusesJenny MendozaNo ratings yet
- Diagnostic VirologyDocument46 pagesDiagnostic VirologySarah DadoNo ratings yet
- Abubaker SikyDocument6 pagesAbubaker SikyAbubaker sikyNo ratings yet
- Herpes VirusesDocument26 pagesHerpes VirusesUmar'Farouq OniNo ratings yet
- Understanding Human Retroviruses and HIVDocument58 pagesUnderstanding Human Retroviruses and HIVRandy BerryNo ratings yet
- Viral Characteristics and StructureDocument24 pagesViral Characteristics and Structurekevin100% (1)
- Biology Ip XiiDocument8 pagesBiology Ip XiiSugumaran MageshNo ratings yet
- Virology ReviewDocument5 pagesVirology ReviewTerence Eday100% (1)
- 5 Herpes VirusesDocument5 pages5 Herpes VirusesTᕼE FᗩᗪEᗪ ᔕOᑌᒪNo ratings yet
- Prof. Dalia M. Mohsen Lecture VirologyDocument24 pagesProf. Dalia M. Mohsen Lecture VirologyDalia M. MohsenNo ratings yet
- Clinical Virology (Dental)Document134 pagesClinical Virology (Dental)samar yousif mohamedNo ratings yet
- HIV Notes (Clinical Virology) MR - ManigaDocument31 pagesHIV Notes (Clinical Virology) MR - ManigaDaniel OkakaNo ratings yet
- AIDSDocument32 pagesAIDSJuwairia tariqNo ratings yet
- Microbiology Introduction To Virology: Dr. Esra HassanDocument9 pagesMicrobiology Introduction To Virology: Dr. Esra HassanjasnaldNo ratings yet
- Pathogenesis To Viruses DDocument16 pagesPathogenesis To Viruses DJaydee PlataNo ratings yet
- DR - Dr.efrida Warganegara, M.Kes., SP - MKDocument30 pagesDR - Dr.efrida Warganegara, M.Kes., SP - MKDedy SantosoNo ratings yet
- Chapter 65 (Introduction To Viruses)Document16 pagesChapter 65 (Introduction To Viruses)leoNo ratings yet
- Microorganism Classification GuideDocument26 pagesMicroorganism Classification GuidehangoverNo ratings yet
- HIV SeminarDocument111 pagesHIV SeminarRakshaNo ratings yet
- L21 - Viral Carcinogenesis-Part 1-S23Document21 pagesL21 - Viral Carcinogenesis-Part 1-S23waNo ratings yet
- Diaz & Estrael Sc23 VirologyDocument69 pagesDiaz & Estrael Sc23 VirologyJohn Rafael DiazNo ratings yet
- b76eeVIRUSES 4Document4 pagesb76eeVIRUSES 4Mudit MisraNo ratings yet
- Herpes Viruses: Viruses Causing Latent InfectionsDocument96 pagesHerpes Viruses: Viruses Causing Latent InfectionsSolustNo ratings yet
- Kimutai N Gideon Dennis Mutiso Moderator DR Songok 07 FEB 2011Document56 pagesKimutai N Gideon Dennis Mutiso Moderator DR Songok 07 FEB 2011drgiddie7640No ratings yet
- Assignment: ON Topic: Pox Viridae General Properties, Dna Replication & Cow Pox DiseaseDocument8 pagesAssignment: ON Topic: Pox Viridae General Properties, Dna Replication & Cow Pox DiseaseVinayak ChuraNo ratings yet
- Human Immunodeficiency Virus (HIV)Document34 pagesHuman Immunodeficiency Virus (HIV)Ahmed SafaNo ratings yet
- Chapter 13 Viruses, Viroids and Prions-2Document31 pagesChapter 13 Viruses, Viroids and Prions-2Hillani TadesseNo ratings yet
- Biology Investigatory Project Viral DiseasesDocument20 pagesBiology Investigatory Project Viral DiseasesAchu Jaseem0% (2)
- Chapter 13 Viral PathogenesisDocument68 pagesChapter 13 Viral PathogenesisKelly WareNo ratings yet
- Key elements of viruses and viral infectionsDocument44 pagesKey elements of viruses and viral infectionsMay BerNo ratings yet
- Disorder of The Immune System 2Document58 pagesDisorder of The Immune System 2Daniel OkakaNo ratings yet
- RetrovirusesDocument79 pagesRetrovirusesrasimmozturkNo ratings yet
- Viruses Notes: Erick MaritimDocument269 pagesViruses Notes: Erick MaritimBeni6620 A.No ratings yet
- Microbialdiseases 160303140348Document42 pagesMicrobialdiseases 160303140348proud.student2023No ratings yet
- Viral Structure NotesDocument9 pagesViral Structure Notesantonia putriNo ratings yet
- Pathological Response To Infectious and Parasitic DiseasesDocument36 pagesPathological Response To Infectious and Parasitic DiseasesCLEMENTNo ratings yet
- What Is HIV?Document8 pagesWhat Is HIV?Quan ThieuNo ratings yet
- HIV ENT ManifestationDocument33 pagesHIV ENT ManifestationAhmad fayazNo ratings yet
- DR - Husni Samadin Mikrobiologi FK - UnsriDocument55 pagesDR - Husni Samadin Mikrobiologi FK - UnsriIlham Akbar Ilaker'ErumbiaNo ratings yet
- Pathogenesis of VirusesDocument32 pagesPathogenesis of VirusesSamuel OgaroNo ratings yet
- Chapter 6: Infectious Diseases and ImmunityDocument32 pagesChapter 6: Infectious Diseases and ImmunityTsegaye YalewNo ratings yet
- Virus 7 LastDocument50 pagesVirus 7 LastBatool SherbiniNo ratings yet
- Human Immunodeficiency VirusDocument110 pagesHuman Immunodeficiency VirusFrancis MakanyaNo ratings yet
- Lab Diagnosis: Specimen Collection & Virus Detection MethodsDocument6 pagesLab Diagnosis: Specimen Collection & Virus Detection MethodsIDRAAK HUSSAINNo ratings yet
- Gulu Cohes Hiv Nelly MDDocument68 pagesGulu Cohes Hiv Nelly MDYIKI ISAACNo ratings yet
- Pertemuan Ke-2 REPRODocument74 pagesPertemuan Ke-2 REPROAdi Joyo NegoroNo ratings yet
- Human Health and DiseaseDocument6 pagesHuman Health and DiseaseSunil GargNo ratings yet
- Chapter 9 Viral of Human DiseaseDocument6 pagesChapter 9 Viral of Human DiseaseMahrukh SaeedNo ratings yet
- Presented By:-Pallavi Chawla Pallavi Dhiman (BDS - 3 Year)Document28 pagesPresented By:-Pallavi Chawla Pallavi Dhiman (BDS - 3 Year)tinu989No ratings yet
- List of ContentsDocument21 pagesList of Contentsankur bharaliNo ratings yet
- Biology Investigatory Project - Viral DiseasesDocument14 pagesBiology Investigatory Project - Viral DiseasesSamiha Antara81% (127)
- General Virology 1Document6 pagesGeneral Virology 1safiya nihaalNo ratings yet
- Lectures On VirusesDocument72 pagesLectures On Virusesvinay guptaNo ratings yet
- 2019 10 31 Chemistry of Death Rebroadcast SlidesDocument38 pages2019 10 31 Chemistry of Death Rebroadcast SlidesLogyn SamNo ratings yet
- 37 Mustafaetal 2020Document7 pages37 Mustafaetal 2020Logyn SamNo ratings yet
- Ancient EgyptDocument4 pagesAncient EgyptLogyn SamNo ratings yet
- Poster TemplateDocument1 pagePoster TemplateLogyn SamNo ratings yet
- AnimalsDocument10 pagesAnimalsLogyn SamNo ratings yet
- Lecture 9 (Renal Tumors)Document15 pagesLecture 9 (Renal Tumors)Logyn SamNo ratings yet
- Lecture 7 (Diseases of Urinary System)Document26 pagesLecture 7 (Diseases of Urinary System)Logyn SamNo ratings yet
- PB3 NP4Document10 pagesPB3 NP4Angelica Charisse BuliganNo ratings yet
- Stages of HIV Infection and AIDS ExplainedDocument10 pagesStages of HIV Infection and AIDS ExplainedHarshitha Gowda HarshiNo ratings yet
- HIV in PregnancyDocument28 pagesHIV in PregnancyRaja100% (1)
- Botswana Ref Ranges PaperDocument7 pagesBotswana Ref Ranges PaperMunyaradzi MangwendezaNo ratings yet
- AIDS and Oral Health - Jaypee Brothers 1st Edition (2006) PDFDocument151 pagesAIDS and Oral Health - Jaypee Brothers 1st Edition (2006) PDFErisa BllakajNo ratings yet
- Pathology COMPRE2018 Finale PDFDocument79 pagesPathology COMPRE2018 Finale PDFrinkal chavdaNo ratings yet
- 2011 HIV Om in BurmeseDocument67 pages2011 HIV Om in BurmesemaponlooNo ratings yet
- Upload 00059265 1503977380705Document25 pagesUpload 00059265 1503977380705Khuon BunthaNo ratings yet
- 02 Review of LiteratureDocument8 pages02 Review of LiteratureAnnapoorna SHNo ratings yet
- Lesson Plan AIDSDocument14 pagesLesson Plan AIDSS GNo ratings yet
- 1 s2.0 S0223523422008005 MainDocument31 pages1 s2.0 S0223523422008005 MainBurakkYılmazNo ratings yet
- Hiv LessonDocument4 pagesHiv Lessonapi-265967818No ratings yet
- Chapter18 Genetics of Viruses and BacteriaDocument69 pagesChapter18 Genetics of Viruses and BacteriaMandaviNo ratings yet
- Acquired Immune Deficiency Syndrome or Acquired Immunodeficiency Syndrome (AIDS) Is A Disease of The Human Immune System Caused byDocument7 pagesAcquired Immune Deficiency Syndrome or Acquired Immunodeficiency Syndrome (AIDS) Is A Disease of The Human Immune System Caused byAdrian MallarNo ratings yet
- Virology ASCPDocument24 pagesVirology ASCP2131443No ratings yet
- Teal Sarah Wnu 1Document4 pagesTeal Sarah Wnu 1api-657367909No ratings yet
- Pencegahan HivDocument17 pagesPencegahan HivJH ELIS RNo ratings yet
- Catalog2021 New Revised ProgramsDocument4 pagesCatalog2021 New Revised ProgramsAlexjuniorysaNo ratings yet
- 美国chemcon公司单抗目录(英文)Document20 pages美国chemcon公司单抗目录(英文)api-3742158No ratings yet
- Buzzer RoundDocument22 pagesBuzzer RoundParmar YogeshNo ratings yet
- TOEFL Kel.4Document13 pagesTOEFL Kel.4Nesti PujiaNo ratings yet
- Beck Protocol HandbookDocument87 pagesBeck Protocol Handbookatideva100% (2)
- Immuno and InfectiousDocument17 pagesImmuno and Infectiousgreen_archerNo ratings yet
- HivrenewalformDocument3 pagesHivrenewalformkbl27No ratings yet
- 2ND Co Lesson Plan Hiv and AidsDocument10 pages2ND Co Lesson Plan Hiv and AidsBryan Cordova BialenNo ratings yet
- Hepati Tac AbstractDocument296 pagesHepati Tac AbstractMagda MagNo ratings yet
- AIDS Virus Man Made by Michel KassettDocument19 pagesAIDS Virus Man Made by Michel KassettCazzac111100% (1)
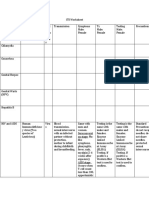
- STI Management GuideDocument6 pagesSTI Management GuideDanielle NelsonNo ratings yet
- 27 Pekeliling KPK 1-2011-CARTA ALIR - UJIAN PENGESAHAN HIVDocument20 pages27 Pekeliling KPK 1-2011-CARTA ALIR - UJIAN PENGESAHAN HIVsiti nur aishah jalilNo ratings yet
- Efecto de Hiv1 en Mujeres Embarazadas de RwandaDocument8 pagesEfecto de Hiv1 en Mujeres Embarazadas de RwandaIsmaelJoséGonzálezGuzmánNo ratings yet