You might also like
- Guide: Curves Built in The GymDocument34 pagesGuide: Curves Built in The GymAlt Ctrl Shift60% (10)
- 14 - Fire Safety and Inspection ChecklistDocument3 pages14 - Fire Safety and Inspection ChecklistSainu Kalathingal83% (6)
- Bpops Template (Plan)Document1 pageBpops Template (Plan)Al Simbajon95% (19)
- Jsa For DG Operation PDFDocument5 pagesJsa For DG Operation PDFajmalvk100% (4)
- English Activity:: 2ND GradeDocument1 pageEnglish Activity:: 2ND GradeJudith Criollo DiazNo ratings yet
- Bnap FormsDocument9 pagesBnap Formsjimelyquinones78No ratings yet
- QuizDocument2 pagesQuizxs8k4ry56mNo ratings yet
- Pro Form A For Participation in Sports 11213Document5 pagesPro Form A For Participation in Sports 11213Foundation 123No ratings yet
- 2021 EVALUATION FORM LETTER SIZE 1stSEMDocument1 page2021 EVALUATION FORM LETTER SIZE 1stSEMJan Myrille CabinganNo ratings yet
- Enhanced FMS FormsDocument18 pagesEnhanced FMS FormsAmyfe AdapNo ratings yet
- PA BGSPD 15 A2 - Scholarship Renewal Form SUC 1Document1 pagePA BGSPD 15 A2 - Scholarship Renewal Form SUC 1Jessica DiazNo ratings yet
- Verification Slip - Provincial FormDocument1 pageVerification Slip - Provincial FormAngel Diaz50% (2)
- SPORTSDocument5 pagesSPORTSSharique AmanNo ratings yet
- Application Form For The U.S. Coast Guard Academy (Uscga) Class of 2024 International Cadet ProgramDocument1 pageApplication Form For The U.S. Coast Guard Academy (Uscga) Class of 2024 International Cadet ProgramJoella PitallanoNo ratings yet
- First Time Job Seeker Application Form 2022Document1 pageFirst Time Job Seeker Application Form 2022jade capalacNo ratings yet
- Reg Form Anthem 2019 PDFDocument1 pageReg Form Anthem 2019 PDFArika MumtazNo ratings yet
- PEL - JubertDocument1 pagePEL - JubertkbcorderoNo ratings yet
- University of Santo Tomas Institute of Physical Education and AthleticsDocument3 pagesUniversity of Santo Tomas Institute of Physical Education and AthleticsJacob CasugboNo ratings yet
- Ug Fees & Check List 2022-23Document7 pagesUg Fees & Check List 2022-23rutuja ghogareNo ratings yet
- Photo Card: Gbayange Lubem Benedict 81RRIDocument6 pagesPhoto Card: Gbayange Lubem Benedict 81RRITerhemen IorverNo ratings yet
- 4ps MCCT Update FormDocument1 page4ps MCCT Update FormDerick MacedaNo ratings yet
- PPE Request FormDocument1 pagePPE Request FormArnold MejiaNo ratings yet
- Travel Expense ChecklistDocument2 pagesTravel Expense ChecklistMichelle Domanacal UrsabiaNo ratings yet
- Hi-Precision - Mission Registration Slip 2 Updated - RVGDocument1 pageHi-Precision - Mission Registration Slip 2 Updated - RVGmhelai guevarraNo ratings yet
- National College of Arts: LahoreDocument5 pagesNational College of Arts: LahorechristianNo ratings yet
- QF 019 Parents Consent and WaiverDocument2 pagesQF 019 Parents Consent and WaiverJhanella TabudloNo ratings yet
- Palladium Fantasy RPG® Character Sheet: Ombat KillDocument1 pagePalladium Fantasy RPG® Character Sheet: Ombat KillElSireNo ratings yet
- Form 4Document1 pageForm 4HARISHRUTHINo ratings yet
- FEE WEBSITE-1 IK EnterprisesDocument6 pagesFEE WEBSITE-1 IK Enterprisesrushdakhan0123No ratings yet
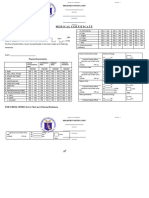
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Lormy Layeka Calderon SiolNo ratings yet
- PA-BGSPD-15-A2 - Scholarship Renewal Form SUCDocument1 pagePA-BGSPD-15-A2 - Scholarship Renewal Form SUCCharles Linelle MendozaNo ratings yet
- Application Form-Summer Internship Program1Document8 pagesApplication Form-Summer Internship Program1Tristan James SimNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Tarhata LampatanNo ratings yet
- PSU Coron Student DirectoryDocument1 pagePSU Coron Student DirectoryJustine Kyle BasilanNo ratings yet
- Travel Order No.: Lawrence D. SempioDocument2 pagesTravel Order No.: Lawrence D. SempioWilliam Leo GasconNo ratings yet
- Scholarship FormDocument1 pageScholarship FormejNo ratings yet
- Membership Savings Remittance Form (MSRF) : HQP-PFF-053Document2 pagesMembership Savings Remittance Form (MSRF) : HQP-PFF-053Airine ParedesNo ratings yet
- Budget ProposalDocument1 pageBudget ProposalJohna Mae EtangNo ratings yet
- Activity ProposalDocument3 pagesActivity ProposalSoleil SierraNo ratings yet
- HPS Bonus Report For FY2010-11 FY2011-12Document25 pagesHPS Bonus Report For FY2010-11 FY2011-12realhartfordNo ratings yet
- Immaj-Pjmcc Cadetship Training Program Cadet Information SheetDocument1 pageImmaj-Pjmcc Cadetship Training Program Cadet Information SheetKevin John Aguipo IINo ratings yet
- Annexure - A/5 Form 5: S.No. Year Place Name of The Tournament/event Events Participated Position Earned 1. 2. 3. 4. 5Document1 pageAnnexure - A/5 Form 5: S.No. Year Place Name of The Tournament/event Events Participated Position Earned 1. 2. 3. 4. 5Kiran BhorNo ratings yet
- Chara SheetDocument2 pagesChara SheetrileyNo ratings yet
- Annexure - A/5 Form 5: S.No. Year Place Name of The Tournament/event Events Participated Position Earned 1. 2. 3. 4. 5Document1 pageAnnexure - A/5 Form 5: S.No. Year Place Name of The Tournament/event Events Participated Position Earned 1. 2. 3. 4. 5Kiran BhorNo ratings yet
- Training ProgramDocument3 pagesTraining ProgramPrem KumarNo ratings yet
- SUC - PA-BGSPD-15-A2 - Scholarship Renewal Form SUC Rev 01Document1 pageSUC - PA-BGSPD-15-A2 - Scholarship Renewal Form SUC Rev 01Mary Jamaica San PedroNo ratings yet
- Annexure - A/1 Form 1: S.No. Year Place Name of The Tournament/event Events Participated Position Earned 1. 2. 3. 4. 5Document1 pageAnnexure - A/1 Form 1: S.No. Year Place Name of The Tournament/event Events Participated Position Earned 1. 2. 3. 4. 5ShaktisinghNo ratings yet
- Clinic First Aider ReportDocument2 pagesClinic First Aider ReportFlorence T. IsidoroNo ratings yet
- National College of Arts ADMISSION SESSION 2021 (Check List)Document5 pagesNational College of Arts ADMISSION SESSION 2021 (Check List)Hamza AliNo ratings yet
- Development ST Org Expense ReportDocument2 pagesDevelopment ST Org Expense ReportStudentFILMcollectivNo ratings yet
- Form 6: Regulation 7Document2 pagesForm 6: Regulation 7Leo BotesNo ratings yet
- Admn Form 08032013 PDFDocument2 pagesAdmn Form 08032013 PDFAhmad Rashed SalimiNo ratings yet
- Cesdi Sports FormsDocument4 pagesCesdi Sports FormsHari Ng SablayNo ratings yet
- Entry/Registration Form: Name of SchoolDocument4 pagesEntry/Registration Form: Name of SchoolElliebotNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1CON REGASPINo ratings yet
- Annex 8 Billing Statement SY 2021-2022Document3 pagesAnnex 8 Billing Statement SY 2021-2022MARY GRACE CABILI100% (1)
- Mymaxicare Application Form: Applicant'S InformationDocument1 pageMymaxicare Application Form: Applicant'S InformationAriane ComboyNo ratings yet
- Aman Amu PDHHHDocument3 pagesAman Amu PDHHHAman AligNo ratings yet
- Afcons Infrastructure Limited: Application FormDocument4 pagesAfcons Infrastructure Limited: Application Formkishan100% (1)
- Introduction NNUDocument3 pagesIntroduction NNUZuna QaziNo ratings yet
- Days and Themes 2022 GPSCDocument10 pagesDays and Themes 2022 GPSC275 DILIP RAYGORNo ratings yet
- 9 INDICATORS COT 2 Lesson Plan in HealthDocument3 pages9 INDICATORS COT 2 Lesson Plan in HealthJoenero Tresquio100% (2)
- Ultrasonic Cleaning Solution, MC-3 - Metal Cleaner - SdsDocument5 pagesUltrasonic Cleaning Solution, MC-3 - Metal Cleaner - SdsLaban KantorNo ratings yet
- JSA For Manual Excavation Inside The Operation Area (Access Road)Document6 pagesJSA For Manual Excavation Inside The Operation Area (Access Road)Mohammed MinhajNo ratings yet
- CV ClemensDocument12 pagesCV Clemensapi-439712011No ratings yet
- Econ 203 Syllabus-Spring 2021-1Document5 pagesEcon 203 Syllabus-Spring 2021-1Reem MohamadNo ratings yet
- Cat Multipurpose TractorOil (MTO) - MSDSDocument11 pagesCat Multipurpose TractorOil (MTO) - MSDSanibal_rios_rivasNo ratings yet
- Chapter Two EhealthDocument10 pagesChapter Two Ehealthaynu gebreNo ratings yet
- Neet Test 04 - Answer Key - PW-AITS - NT-04 (PCB) - Answer KeyDocument2 pagesNeet Test 04 - Answer Key - PW-AITS - NT-04 (PCB) - Answer Keytanmay jha50% (2)
- Java Script 2Document50 pagesJava Script 2ashishkumar140806No ratings yet
- Discharge PlanningDocument6 pagesDischarge PlanningHamdah GirlsNo ratings yet
- Keperawatan Dengan Masalah Gangguan Intoleransi Aktivitas Pada Pasien Hepatitis B Di Rumah Sakit TK II Putri Hijau Medan Tahun 2021Document12 pagesKeperawatan Dengan Masalah Gangguan Intoleransi Aktivitas Pada Pasien Hepatitis B Di Rumah Sakit TK II Putri Hijau Medan Tahun 2021Boys SanNo ratings yet
- Medical Updates As On The 18th April 2024Document38 pagesMedical Updates As On The 18th April 2024nxtvistaenterprisesNo ratings yet
- Motivation, Compliance and Satisfaction in Orthodontic TreatmentDocument16 pagesMotivation, Compliance and Satisfaction in Orthodontic TreatmentAkram AlsharaeeNo ratings yet
- Case Digest RapeDocument20 pagesCase Digest RapeRaymond Ruther100% (3)
- Pre Prosthetic Surgery Part I &IIDocument160 pagesPre Prosthetic Surgery Part I &IItegegnegenet2No ratings yet
- Bleeding Disorders Ce319Document25 pagesBleeding Disorders Ce319cesimpsonNo ratings yet
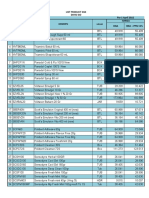
- Divisi Go List Product GSK Per 1 April 2022 Harga: NO Kode Produk Deskripsi SatuanDocument2 pagesDivisi Go List Product GSK Per 1 April 2022 Harga: NO Kode Produk Deskripsi Satuanmispa hendriNo ratings yet
- Đề Phát Triển Minh Họa Tiếng Anh 2024 - Chuẩn Cấu Trúc - Đề Số 1Document18 pagesĐề Phát Triển Minh Họa Tiếng Anh 2024 - Chuẩn Cấu Trúc - Đề Số 1anhdtd1006No ratings yet
- Wickes 1953 Part 1Document8 pagesWickes 1953 Part 1Tanya CassidyNo ratings yet
- Unit 1 - CounselingDocument10 pagesUnit 1 - CounselingPriyadharshini TNo ratings yet
- Penggunaan Serbuk Buah Pare (Momordicha: Charantia L) Terhadap Kematian Larva Aedes AegyptiDocument8 pagesPenggunaan Serbuk Buah Pare (Momordicha: Charantia L) Terhadap Kematian Larva Aedes AegyptiWireifnitedNo ratings yet
- 1 Identification: Safety Data SheetDocument7 pages1 Identification: Safety Data SheetNicol GuevaraNo ratings yet
- Academic Burnout and Coping Strategies of Nurse Educators For FINAL CONSULTATIONDocument27 pagesAcademic Burnout and Coping Strategies of Nurse Educators For FINAL CONSULTATIONduca.danrainer02No ratings yet
- Depot-Ped: 3 Months: 11.25 MG or 30 MG Q12weeks. (SQ) Lupron: Children: Initially, 50Document3 pagesDepot-Ped: 3 Months: 11.25 MG or 30 MG Q12weeks. (SQ) Lupron: Children: Initially, 50thuey epeNo ratings yet
- CAP Exam OutlineDocument10 pagesCAP Exam OutlineironmanNo ratings yet
- 038 1084E - Hydraulic Dock Leveler - Owner S ManualDocument32 pages038 1084E - Hydraulic Dock Leveler - Owner S ManualAndres F. TrujilloNo ratings yet