You might also like
- Doctor On Call BookDocument42 pagesDoctor On Call BookFarzana Samejo100% (1)
- Anemia Hemolítica Autoinmune NEJMDocument13 pagesAnemia Hemolítica Autoinmune NEJMSMIBA Medicina100% (1)
- Autonomic Neuropathy in Patients With HIV: Course, Impact of Disease Stage, and MedicationDocument6 pagesAutonomic Neuropathy in Patients With HIV: Course, Impact of Disease Stage, and MedicationkarinarakhmaNo ratings yet
- Clinical Neurology and NeurosurgeryDocument5 pagesClinical Neurology and NeurosurgeryAffan AdibNo ratings yet
- C-Reactive Protein During and After Myocardial Infarction in Relation To Cardiac Injury and Left Ventricular Function at Follow-UpDocument6 pagesC-Reactive Protein During and After Myocardial Infarction in Relation To Cardiac Injury and Left Ventricular Function at Follow-UpALVARO LUCIO JIBAJA DEZANo ratings yet
- Radiologi 3Document5 pagesRadiologi 3Sarah watiNo ratings yet
- Reducing Central Nervous System Complications Associated With The Human Immunodeficiency VirusDocument4 pagesReducing Central Nervous System Complications Associated With The Human Immunodeficiency VirusJoaoMarioFloresFernandezNo ratings yet
- 3.Dias-2015-RETROSPECTIVE COHORT-Antiplatelet Therapy in TakotsuboDocument6 pages3.Dias-2015-RETROSPECTIVE COHORT-Antiplatelet Therapy in TakotsuboHi GamingNo ratings yet
- Bradyarrhythmias in Patientswith COVID-19Document6 pagesBradyarrhythmias in Patientswith COVID-19Marcela Soruco AyupeNo ratings yet
- Procal Vs MasccDocument7 pagesProcal Vs MasccRoshan MathewNo ratings yet
- Factores para FNRDocument10 pagesFactores para FNRPOMYNo ratings yet
- PCT 2006 Read For DiscussionDocument8 pagesPCT 2006 Read For DiscussionArnavjyoti DasNo ratings yet
- Life 11 01429Document14 pagesLife 11 01429Genesis PerezNo ratings yet
- Presenter: Dr. Deborah Pakpahan Supervisor: Dr. Reyhan Eddy Yunus, Sprad, M.SCDocument27 pagesPresenter: Dr. Deborah Pakpahan Supervisor: Dr. Reyhan Eddy Yunus, Sprad, M.SCDeborah Anasthasia PakpahanNo ratings yet
- Cardiovascular Disease in Rheumatoid Arthritis: Single-Center Hospital-Based Cohort Study in FranceDocument15 pagesCardiovascular Disease in Rheumatoid Arthritis: Single-Center Hospital-Based Cohort Study in Francemarisa isahNo ratings yet
- BMM 2018 0348Document14 pagesBMM 2018 0348Harpreet SinghNo ratings yet
- Usefulness of Elevated Troponin To Predict Death in Patients With COVID-19 and Myocardial InjuryDocument7 pagesUsefulness of Elevated Troponin To Predict Death in Patients With COVID-19 and Myocardial InjurySilvhy yujraNo ratings yet
- Covid ResearchDocument4 pagesCovid ResearchDr. Kaushal Kishor SharmaNo ratings yet
- Cardiac Pathology 6 Months After Hospitalization For COVID-19 and Association With The Acute Disease SeverityDocument11 pagesCardiac Pathology 6 Months After Hospitalization For COVID-19 and Association With The Acute Disease SeverityArdhia Kusuma PutriNo ratings yet
- Cardiac Troponin-I As A Marker of Myocardial Dysfunction in Children With Septic ShockDocument5 pagesCardiac Troponin-I As A Marker of Myocardial Dysfunction in Children With Septic ShockjessicaesmrldaNo ratings yet
- A Multicenter Cohort StudyDocument9 pagesA Multicenter Cohort Studyfatchurhamzah62No ratings yet
- Chest CT Vs RT-PCR in Covid-19Document9 pagesChest CT Vs RT-PCR in Covid-19Srini AwallaNo ratings yet
- Correlations of CT Scan With High-Sensitivity C-ReDocument5 pagesCorrelations of CT Scan With High-Sensitivity C-ReAnthony ChristantoNo ratings yet
- Thesis TopicsDocument14 pagesThesis TopicskiranNo ratings yet
- 1 Pag 4Document10 pages1 Pag 4Mr. LNo ratings yet
- Impact of Atropine and Aminophylline On TAVB With Inferior Wall MIDocument2 pagesImpact of Atropine and Aminophylline On TAVB With Inferior Wall MIRakhmat RamadhaniNo ratings yet
- HSR3 07 PicarielloDocument8 pagesHSR3 07 Picarielloserena7205No ratings yet
- Ijph 41 2 63Document7 pagesIjph 41 2 63Asry AchyyNo ratings yet
- Ijph 41 2 63 PDFDocument7 pagesIjph 41 2 63 PDFAsry AchyyNo ratings yet
- ReferensiDocument7 pagesReferensireza amahoruNo ratings yet
- MyocarditisDocument10 pagesMyocarditisJesús QuirarteNo ratings yet
- Comparative Study of Serum and Biliary Lipid Profile in Libyan Gallstone PatientsDocument54 pagesComparative Study of Serum and Biliary Lipid Profile in Libyan Gallstone PatientsJagannadha Rao PeelaNo ratings yet
- Hsu2019 PDFDocument6 pagesHsu2019 PDFrachmadyNo ratings yet
- The First Affiliated Hospital of Zhengzhou University, Nöroloji, Zhengzhou, ÇinDocument12 pagesThe First Affiliated Hospital of Zhengzhou University, Nöroloji, Zhengzhou, ÇinwithoutlifeNo ratings yet
- Macin 2005Document7 pagesMacin 2005Picha PichiNo ratings yet
- 2001 - Value of ECG in AMI - JAMADocument8 pages2001 - Value of ECG in AMI - JAMAMichail PapafaklisNo ratings yet
- Cancer - 2002 - Tomita - Prophylactic Intrathecal Methotrexate and Hydrocortisone Reduces Central Nervous System RecurrenceDocument5 pagesCancer - 2002 - Tomita - Prophylactic Intrathecal Methotrexate and Hydrocortisone Reduces Central Nervous System RecurrenceJan Marnie ReniedoNo ratings yet
- Chapter IIDocument2 pagesChapter IIDian Abdurrahman MathondangNo ratings yet
- Clinical Cardiology - 2022 - Liang - Prognostic Value of RDW Alone and in Combination With NT proBNP in Patients With HeartDocument13 pagesClinical Cardiology - 2022 - Liang - Prognostic Value of RDW Alone and in Combination With NT proBNP in Patients With Heartrizkiyah prabawantiNo ratings yet
- Bedside Multimarker Testing For Risk StratificationDocument6 pagesBedside Multimarker Testing For Risk StratificationGabriel Cadavid GilNo ratings yet
- Jamacardiology Puntmann 2020 Oi 200057Document9 pagesJamacardiology Puntmann 2020 Oi 200057Henry DanielNo ratings yet
- Study of Congenital Heart Disease in Neonates: Clinical Profile, Diagnosis, Immediate Outcome and Short-Term Follow-UpDocument6 pagesStudy of Congenital Heart Disease in Neonates: Clinical Profile, Diagnosis, Immediate Outcome and Short-Term Follow-UpDhiaul IzzahNo ratings yet
- TCC Con Fase de Continuación para DepresiónDocument15 pagesTCC Con Fase de Continuación para DepresiónGuillermo Van LooNo ratings yet
- Nejmoa 2100591Document12 pagesNejmoa 2100591FELIPE OTALVARO ALVAREZNo ratings yet
- Euro J of Neurology - 2023 - Kincl - Parkinson S Disease Cardiovascular Symptoms A New Complex Functional and StructuralDocument9 pagesEuro J of Neurology - 2023 - Kincl - Parkinson S Disease Cardiovascular Symptoms A New Complex Functional and StructuralIvan MihailovicNo ratings yet
- Determining Which Hospitalized Coronavirus Disease 2019 Patients Require Urgent EchocardiographyDocument8 pagesDetermining Which Hospitalized Coronavirus Disease 2019 Patients Require Urgent EchocardiographyMarco Antonio Viera ArevaloNo ratings yet
- COVID 19 RadiologyDocument29 pagesCOVID 19 RadiologyДоржготов АриунболдNo ratings yet
- Association of Second Trimester Uterine Artery Doppler Parameters WithDocument6 pagesAssociation of Second Trimester Uterine Artery Doppler Parameters WithpaolabriglimNo ratings yet
- Meningitis BacterialisDocument9 pagesMeningitis BacterialisReza OktaramaNo ratings yet
- Safety and Health Status Following Early Discharge in Patients With Acute Myocardial Infarction Treated With Primary PCI: A Randomized TrialDocument8 pagesSafety and Health Status Following Early Discharge in Patients With Acute Myocardial Infarction Treated With Primary PCI: A Randomized TrialsarahNo ratings yet
- Main 51 ???Document5 pagesMain 51 ???pokharelriwaj82No ratings yet
- Nejmc2008597 PDFDocument2 pagesNejmc2008597 PDFAdriana VasilicaNo ratings yet
- Save More StudyDocument22 pagesSave More StudyChris VettasNo ratings yet
- 1 s2.0 S0009898118300500 MainDocument8 pages1 s2.0 S0009898118300500 MainMohamed AmineNo ratings yet
- Comparison of CK-MB Subforms and Troponin I in The Evaluation of Patients With Acute Coronary SyndromesDocument20 pagesComparison of CK-MB Subforms and Troponin I in The Evaluation of Patients With Acute Coronary SyndromesMitch de LeonNo ratings yet
- Angina 22Document3 pagesAngina 22Aqa Mirza Muhammad Al-SyahabadiNo ratings yet
- PESI Critical Care 2005Document6 pagesPESI Critical Care 2005Rocio Méndez FrancoNo ratings yet
- Haberka 2013Document10 pagesHaberka 2013Angie Kiara CamposNo ratings yet
- Sensitive Mirna Markers For The Detection and Management of Nstemi Acute Myocardial Infarction PatientsDocument10 pagesSensitive Mirna Markers For The Detection and Management of Nstemi Acute Myocardial Infarction PatientsSabariaNo ratings yet
- 10.1007@s10554 020 01913 6Document10 pages10.1007@s10554 020 01913 6Bosman AriestaNo ratings yet
- Assessment of Palpitation Complaints Benign Paroxysmal Positional VertigoDocument6 pagesAssessment of Palpitation Complaints Benign Paroxysmal Positional VertigoHappy PramandaNo ratings yet
- Noninvasive Diagnosis of Vascular DiseaseFrom EverandNoninvasive Diagnosis of Vascular DiseaseFalls B. HersheyRating: 5 out of 5 stars5/5 (1)
- Helicobacter Pylori Infection: Disease PrimersDocument24 pagesHelicobacter Pylori Infection: Disease PrimersKenny BellodasNo ratings yet
- Long COVIDDocument8 pagesLong COVIDSMIBA MedicinaNo ratings yet
- POCKET GUIDE GOLD 2023 Ver 1.2 17feb2023 - WMVDocument55 pagesPOCKET GUIDE GOLD 2023 Ver 1.2 17feb2023 - WMVMARISOL FERNANDA GÓMEZNo ratings yet
- Manejo Endocarditis en Usuarios de DrogasDocument15 pagesManejo Endocarditis en Usuarios de DrogasSMIBA MedicinaNo ratings yet
- Prevención StrokeDocument4 pagesPrevención StrokeSMIBA MedicinaNo ratings yet
- Artículo Enfermedad Criptocócica y HIVDocument64 pagesArtículo Enfermedad Criptocócica y HIVSMIBA MedicinaNo ratings yet
- PolipillDocument10 pagesPolipillSMIBA MedicinaNo ratings yet
- Artículo Sueño y CorazónDocument26 pagesArtículo Sueño y CorazónSMIBA MedicinaNo ratings yet
- Encefalitis 2022Document10 pagesEncefalitis 2022SMIBA MedicinaNo ratings yet
- Hipertensión Pulmonar (2022)Document114 pagesHipertensión Pulmonar (2022)Mauricio CabreraNo ratings yet
- Artículo Guía Tto y Profilaxis Tromboembolismo en CáncerDocument14 pagesArtículo Guía Tto y Profilaxis Tromboembolismo en CáncerSMIBA MedicinaNo ratings yet
- Pericarditis AgudaDocument9 pagesPericarditis AgudaSMIBA MedicinaNo ratings yet
- Uso de Albúmina en CirrosisDocument12 pagesUso de Albúmina en CirrosisSMIBA MedicinaNo ratings yet
- Artículo LeuconiquiaDocument17 pagesArtículo LeuconiquiaSMIBA Medicina100% (1)
- Sueño y ObesidadDocument10 pagesSueño y ObesidadSMIBA MedicinaNo ratings yet
- COVID ProlongadoDocument22 pagesCOVID ProlongadoSMIBA MedicinaNo ratings yet
- Clostridium y MicrobiomaDocument10 pagesClostridium y MicrobiomaSMIBA MedicinaNo ratings yet
- Guía OxigenoterapiaDocument39 pagesGuía OxigenoterapiaSMIBA MedicinaNo ratings yet
- Guía Hemorragia Intestino DelgadoDocument8 pagesGuía Hemorragia Intestino DelgadoSMIBA MedicinaNo ratings yet
- Manejo IRCDocument11 pagesManejo IRCSMIBA Medicina100% (1)
- Artículo Dislipemia ESCDocument12 pagesArtículo Dislipemia ESCSMIBA MedicinaNo ratings yet
- Artículo COVID 19 Tto Ac MonoclonalesDocument14 pagesArtículo COVID 19 Tto Ac MonoclonalesSMIBA MedicinaNo ratings yet
- Resistencia BacterianaDocument27 pagesResistencia BacterianaSMIBA MedicinaNo ratings yet
- Artículo Manejo de CoagulopatíaDocument17 pagesArtículo Manejo de CoagulopatíaSMIBA MedicinaNo ratings yet
- Artículo COVID 19 Test SalivaDocument13 pagesArtículo COVID 19 Test SalivaSMIBA MedicinaNo ratings yet
- Stroke AHA GuidelinesDocument104 pagesStroke AHA GuidelinesCristina ZeamaNo ratings yet
- POCUSDocument10 pagesPOCUSSMIBA MedicinaNo ratings yet
- Lukoff - Mysticism and PsychosisDocument27 pagesLukoff - Mysticism and Psychosiscurfexxx100% (1)
- Nani Web AUTORETIC Research StudyDocument1 pageNani Web AUTORETIC Research StudyihcflowNo ratings yet
- Makalah Fitoterapi: Serenoa Repens (Saw Palmetto) Untuk Mengobati Penyakit ProstatDocument9 pagesMakalah Fitoterapi: Serenoa Repens (Saw Palmetto) Untuk Mengobati Penyakit ProstatFauzi Rizqi KoesmadjiNo ratings yet
- Sono PDFDocument3 pagesSono PDFJeyarajasekar TtrNo ratings yet
- IPSGDocument4 pagesIPSGmohsinaNo ratings yet
- Tuberculosis and Poverty: What Could (And Should) Be Done?Document8 pagesTuberculosis and Poverty: What Could (And Should) Be Done?Richard GabrielNo ratings yet
- Pharmacotherapeutics PDFDocument30 pagesPharmacotherapeutics PDFprazol shresthaNo ratings yet
- Pembrolizumab Plus Pemetrexedplatinum For Metastatic Nonsquamous NSCLC KEYNOTE 189 Japan StudyDocument11 pagesPembrolizumab Plus Pemetrexedplatinum For Metastatic Nonsquamous NSCLC KEYNOTE 189 Japan StudyasdffdsaNo ratings yet
- Demodex: Demodex Mites As Seen Through A MicroscopeDocument3 pagesDemodex: Demodex Mites As Seen Through A MicroscopeGhea Tahara SugiantoNo ratings yet
- Alzheimer's Disease: From The Bench To The ClinicDocument37 pagesAlzheimer's Disease: From The Bench To The Clinichoyvin100% (1)
- Safety Data Sheet: 1. IdentificationDocument11 pagesSafety Data Sheet: 1. IdentificationAshley GuevaraNo ratings yet
- The Family Addict: A Review of The LiteratureDocument11 pagesThe Family Addict: A Review of The Literaturemiksi7906No ratings yet
- Antacids Are Medicines That Neutralize Stomach AcidDocument15 pagesAntacids Are Medicines That Neutralize Stomach Acidrishabhrawat0% (1)
- GraphDocument243 pagesGraphsubash1111@gmail.comNo ratings yet
- PDF Biochemical Parameters and The Nutritional Status of Children Novel Tools For Assessment 1St Edition Anil Gupta Author Ebook Full ChapterDocument54 pagesPDF Biochemical Parameters and The Nutritional Status of Children Novel Tools For Assessment 1St Edition Anil Gupta Author Ebook Full Chapterjeffrey.price646100% (2)
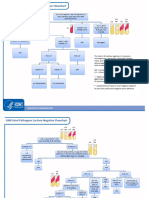
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Congestive Heart Failure Nursing CareDocument20 pagesCongestive Heart Failure Nursing Careminikompo100% (1)
- Black Plague PowerpointDocument24 pagesBlack Plague Powerpointapi-330079068100% (1)
- ADA Caries Risk Assessmento Mayores 6Document2 pagesADA Caries Risk Assessmento Mayores 6Catalina Cané Muñoz SilvaNo ratings yet
- Natural ProductsDocument82 pagesNatural ProductsChandra Reddy100% (1)
- Nutritional Needs of InfantsDocument8 pagesNutritional Needs of InfantsArianna Jasmine MabungaNo ratings yet
- Thiago English Inglês ESA 2020 - 2 Simulado ESA 2020Document3 pagesThiago English Inglês ESA 2020 - 2 Simulado ESA 2020Gabriel GomesNo ratings yet
- Material Safety Data SheetDocument2 pagesMaterial Safety Data Sheetمحمد عزتNo ratings yet
- Immunity: by U.SivakumarDocument37 pagesImmunity: by U.SivakumarAkash JaatNo ratings yet
- Genetic Recombination in BacteriaDocument16 pagesGenetic Recombination in Bacteriavineetvishal73No ratings yet
- Chap1 Introduction To Nutritional AssessmentDocument32 pagesChap1 Introduction To Nutritional AssessmentAbdi Khalaq Ali Hashi100% (1)
- ACC Anywhere Session ListingDocument9 pagesACC Anywhere Session ListingnideNo ratings yet
- 3rd Ccpbiosimconference Abstract BookletDocument82 pages3rd Ccpbiosimconference Abstract BookletRajeev Ranjan RoyNo ratings yet
- Model Dairy Project For 200 AnimalsDocument14 pagesModel Dairy Project For 200 AnimalsDHARIMIREDDY PAVAN KUMAR100% (1)