Volume 7, Issue 9, September – 2022 International Journal of Innovative Science and Research Technology
ISSN No:- 2456-2165
Post-Operative Outcomes Comparing Different
Techniques of Stump Closure after Distal
Pancreatectomy Post-Operative
Complications in Stump Closure
Dr. Shahbaz Khan, Dr. Muhib Ullah Dr. Muhammad Ayub
Specialist registrar, surgical A unit Hayatabad medical Medical officer, Khyber teaching hospital,
complex, Peshawar Pakistan Peshawar Pakistan
Dr. Jamshed Alam Dr. Zahra Alam Jan
Associate professor, surgical A unit Hayatabad Trainee Medical Officer, Gynae unit Hayatabad
Medical Complex, Peshawar, Pakistan Medical complex, Peshawar, Pakistan
Abstract:- Introduction: Distal pancreatectomy (DP) is I. INTRODUCTION
a preferred therapy for pancreatic disorders that affect
just the body and tail of the pancreas and do not include Distal pancreatectomy (DP) is a preferred therapy for
the head. Various methods are in practice for the stump pancreatic disorders that affect just the body and tail of the
closure after PD. The current study assesses the pancreas and do not include the head. Surgery is indicated
comparison of the autologous patch, hand sutured, and for benign as well as malignant diseases. In most studies,
staple in terms of postoperative complications and recent advances in surgery and enhanced pre and
hospital stays in stump closure after DP. Method: A perioperative care resulted in a 2% decrease in mortality
prospective study was conducted in patients who associated with DP [1, 2]. However, there was no
underwent stump closure after DP between August 2017 significant decrease in associated morbidity. It may be due
and March 2022 at Hayatabad Medical Complex, to the development of postoperative pancreatic fistula
Peshawar, Pakistan. After giving informed consent, the (POPF), which significantly contributes to the increased
patient was divided into three groups, including the morbidity. Post-surgery, the pancreatic juice is
autologous patch group (APG), hand sutured group continuously produced and excreted from the remnant of
(HSG), and stapled group (SG). The outcome of the the pancreatic tissue. If the closure fails to seal the ducts or
current study was operation time, intraoperative the residual surface, the pancreatic secretions will lyse the
bleeding, POPF, and hospital stay. The statistical surrounding tissues, resulting in intra-abdominal fluid
analysis was carried out using SPSS v25. Results: The collections, abscesses, or abdominal bleeding and fistulas.
mean operation time was observed lowest in the APG Multiple approaches have been proposed to prevent fistula
while highest in the SG. In the SG, most of the patients development; however, POPF is still challenging for
were fell in ASA grade ranged from I to III, while most surgeons [2-6].
of the APG patients were fell in ASA grade I. The
patients with grade C POPF was high in the HSG, So far, six different procedures have been documented
whereas the grade B POPF was high in the SG. Based to be used for stump closure after DP. These include hand
on CDC, the grade V postoperative complications were sutures on the stump to close the draining pancreatic duct,
high in the HSG and SG. The hospital stay was stapler-based transection, and concomitant stump closure,
observed less in patients who underwent autologous and a combination of stapler-based resection with manual
patch surgery compared to HSG and SG. Conclusion: sutures along the stapler line, pancreatico-enteric or -gastric
The current study highlighted that an autologous patch anastomosis, application of fibrin/coagulation factor-like
was superior to hand-sewn stump closure after DP in bio-sealants, and placement of autologous. In addition to
terms of the operation time, POPF, postoperative these procedures, laparoscopic DP is a new technological
complications based on CDC, and hospital stay. feature but still facing with a POPF [7-10]. Furthermore,
Whereas the patients presented almost the same there is a broad range of PF rates following DP, ranging
postoperative complications who underwent autologous from 12% to 51%, as well as significant variances in stump
patch and stapled stump closure. closure procedures used in different pancreatic centers
throughout the globe [7, 11].
Keywords:- Distal pancreatectomy, stump closure,
postoperative complications. The incidence of POPF after DP remains high, and
different pancreatic stump closure techniques have been
used to lower the prevalence. Moreover, many techniques
have been proposed for managing the pancreatic remnant to
reduce the incidence of PF after DP. Stapler closure and
hand-sewn closure of the pancreatic stump are the standard
methods described in the literature [12-14]. Several other
IJISRT22SEP696 www.ijisrt.com 1015
Volume 7, Issue 9, September – 2022 International Journal of Innovative Science and Research Technology
ISSN No:- 2456-2165
strategies, such as bipolar scissors, fibrin glue sealant, III. RESULT
omental plug, falciform ligament patch, saline-linked
radiofrequency ablation and pancreatojejunostomy of the In the current study, there was a significant difference
pancreatic stump, have also been described [15-17]. among the surgery group in terms of age (p=0.007). The
However, none of the current stump closure techniques mean operation time of the was observed lowest in the
have proven satisfactory for all patients [18-20]. The APG while highest in the SG (215.0±5.57 vs 240.13±4.55,
current study assesses the comparison of the autologous p<0.0001). the detail can be seen in Table 1.
patch, hand sutured, and staple in terms of postoperative
complications and hospital stays in stump closure after DP. Group
II. METHOD APG HSG SG P-
valu
mean± mean± e
A. Patients mean±S
SD/n SD/n
A prospective study was conducted in patients who D/n (%)
(%) (%)
underwent stump closure after DP between August 2017
and March 2022 at Hayatabad Medical Complex, Peshawar, Age (years) 41.80±4. 44.71±2. 44.50±2.0
0.007
Pakistan. All patients were included in the study who 32 21 0
underwent autologous patch, hand sutured, and stapled for
Gend Male 7 (29.2) 9 (37.5) 8 (33.3)
stump closure after DP. After giving informed consent, the
er 0.58
patient was divided into three groups, including the Fema
autologous patch group (APG), hand sutured group (HSG), 4(21.1) 6 (31.6) 9 (47.4)
le
and stapled group (SG). These patients were prospectively
followed for postoperative complications and hospital stay. Duration of 215.0±5. 225.57±7 240.13±4. <0.00
A tube drain was inserted at the pancreatic cut surface or operation (min) 57 .72 55 01
anastomosis. Amylase levels in the drainage fluid were Intra-operative 346.20±8 350.86±1 342.75±8.
monitored on days 5 and 7, and then twice weekly for the 0.196
blood loss (ml) .07 0.5 92
next two weeks in patients who developed a fistula. The
drain was withdrawn on days 3 and 5 and removed on day 7 Table 1: Patient Characteristics And Peri-Operative Status
in the normal case. Before discharge, all patients had Of Surgeries
postoperative ultrasonography (US) and/or computed
Autologous patch group (APG), Hand sutured group (HSG),
tomography (CT).
Stapled group (SG.)
B. Outcomes
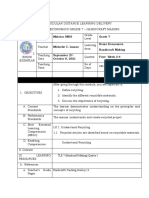
The outcome of the current study was operation time, In the SG, most of the patients were fell in ASA grade
intraoperative bleeding, POPF, and hospital stay. The POPF ranged from I to III, while most of the APG patients were
was graded according to the International Study Group on fell in ASA grade I (Figure 1A). The patients with grade C
Pancreatic Fistulas (ISGPF). The severity is graded from A POPF was high in the HSG, whereas the grade B POPF was
(least severe) through C (most severe). The clinical state, high in the SG (Figure 1B). Based on CDC, the grade V
therapy used, imaging study findings, delayed drainage, postoperative complications were high in the HSG and SG
reoperation, mortality, infection symptoms, and re- (Figure 1C). The hospital stay was observed less in patients
admission were used to grade POPF. The postoperative who underwent autologous patch surgery compared to HSG
complication was assessed using clavien-dindo and SG (Figure 1D).
classification (CDC). Based on this classification, the
postoperative complication was divided into five grades
ranging from no complications (Grade I) to severe
complications, which lead to death (Grade V).
C. Statistical analysis
The statistical analysis was performed using a statistical
package for social sciences (SPSS v25). The categorical
variables were tabulated as frequency and percentage, while
the scale variables were presented as mean and standard
deviation. Statistical differences between the subgroups
were assessed using the Kruskal-Wallis and Chi-square
tests, whereas the independent t-test and One-way AVOVA
test were used where the dependent variable was scale. The
P-value was statistically significant at a 0.05 level.
Fig. 1: Comparison of the Outcome Variables
IJISRT22SEP696 www.ijisrt.com 1016
Volume 7, Issue 9, September – 2022 International Journal of Innovative Science and Research Technology
ISSN No:- 2456-2165
IV. DISCUSSION absorbable mesh. Several small sample size prospective
trials and retrospective cohort studies have demonstrated
The current study highlighted that an autologous patch some reduction in POPF with its use [28]. However, a
was superior to hand-sewn stump closure after DP in terms multicenter RCT of 275 patients evaluating the use of an
of the operation time, POPF, postoperative complications absorbable fibrin sealant patch (TachoSil) revealed no
based on CDC, and hospital stay. Whereas the patients significant reduction in grade B or C POPF with its use in
presented almost the same postoperative complications, patients undergoing DP (TachoSil 8% vs no TachoSil 14%,
who underwent autologous patch and stapled stump p=0.139) [29]. Various glues have also been evaluated,
closure. with most studies showing no reduction in the rates of
POPF. Such glues include cyanoacrylate formulations and
One of the most common causes of postoperative fibrin glues [30].
complications is pancreatic leak [21]. It has been reported
that pancreatic leak occurs in 30% of patients. This is a V. CONCLUSION
greater rate than pancreaticoduodenectomy. The current
study shows POPF is the most common surgical The current study highlighted that an autologous patch
complication and has been reported that it is linked with was superior to hand-sewn stump closure after DP in terms
pancreatic leak [8]. However, depending on the grade, the of the operation time, POPF, postoperative complications
POPF can be managed. Notably, 70% of pancreatic fistulas based on CDC, and hospital stay. Whereas the patients
resolved spontaneously [8]. However, the best therapeutic presented almost the same postoperative complications who
strategy is still up for debate. The rate of grade C pancreatic underwent autologous patch and stapled stump closure.
fistula requiring a re-exploration range from 5 to 20%, with
a mortality rate of 39% [22]. The pancreatic fisula is REFERENCES
currently managed by pancreatic remnant preservation and
a complete pancreatectomy [23]. Although pancreatectomy [1.] van der Heijde N, Lof S, Busch OR, de Hingh I, de
prevents additional PF, it is associated with total pancreatic Kleine RH, Molenaar IQ, et al. Incidence and impact
insufficiency, which leads to brittle diabetes. The of postoperative pancreatic fistula after minimally
preservation strategy is technically simpler and has the invasive and open distal pancreatectomy. Surgery.
added benefit of preserving pancreatic function. However, 2022;171(6):1658-64.
it increases the risk of persistent pancreatic hemorrhage. [2.] Sa Cunha A, Carrere N, Meunier B, Fabre JM,
Furthermore, there is experience with other treatments, Sauvanet A, Pessaux P, et al. Stump closure
such as pancreaticogastrostomy conversion and the reinforcement with absorbable fibrin collagen sealant
bridging stent procedure. Moreover, there is no proof that sponge (TachoSil) does not prevent pancreatic fistula
drainage of the pancreatic duct with a stent can reduce PF after distal pancreatectomy: the FIABLE multicenter
rate following PD [24]. Finally, there is the practice of re- controlled randomized study. Am J Surg.
sectioning a dehiscent jejunal loop and pancreatic drainage, 2015;210(4):739-48.
followed by gastrofistulostomy [25]. [3.] Aoki T, Mansour DA, Koizumi T, Matsuda K,
Kusano T, Wada Y, et al. Preventing clinically
Patients who have complications following pancreatic relevant pancreatic fistula with combination of linear
surgery have three times the cost of those who do not have stapling plus continuous suture of the stump in
complications. It is worth noting that PF type C is one of laparoscopic distal pancreatectomy. BMC Surg.
the most severe postoperative surgical complications. These 2020;20(1):223.
patients' hospital stays are substantially longer than those of [4.] Hüttner FJ, Probst P, Kenngott HG, Knebel P, Hackert
patients who do not have PF [26]. A median total cost of T, Ulrich A, et al. 2-octyl cyanoacrylate sealing of the
the treatment depends on the type of PF: A, B, and C— pancreatic remnant after distal pancreatectomy - A
100%, 170%, and 620%, respectively. There is no prospective pilot study. PLoS One.
significant difference in total cost between patients without 2018;13(10):e0205748.
PF and with PF type A. One retrospective cohort study has [5.] Kawai M, Hirono S, Okada K, Sho M, Nakajima Y,
shown that dedicated oversewing of the main pancreatic Eguchi H, et al. Randomized Controlled Trial of
duct reduces the rates of POPF (9.6% vs 34.0%, p<0.001). Pancreaticojejunostomy versus Stapler Closure of the
However, such a result was probably obtained due to a Pancreatic Stump During Distal Pancreatectomy to
more accurate identification of the pancreatic duct in Reduce Pancreatic Fistula. Ann Surg.
tougher and more fibrotic pancreas, which is associated 2016;264(1):180-7.
with a decreased risk of POPF. The placement of a jejunal [6.] Konishi T, Hiraishi M, Kubota K, Bandai Y,
seromuscular patch to the DP staple line has also been Makuuchi M, Idezuki Y. Segmental occlusion of the
studied, with no difference in POPF rates. Drainage of the pancreatic duct with prolamine to prevent fistula
remaining stump via a pancreatoenteric anastomosis was formation after distal pancreatectomy. Ann Surg.
also investigated, but no significant difference in POPF 1995;221(2):165-70.
rates was seen [27]. [7.] Diener MK, Knaebel HP, Witte ST, Rossion I, Kieser
M, Buchler MW, et al. DISPACT trial: a randomized
Various ancillary methods have been described to controlled trial to compare two different surgical
reinforce stump closure of the remnant pancreas after DP. techniques of DIStal PAnCreaTectomy - study
This includes the use of staple line reinforcement with an rationale and design. Clin Trials. 2008;5(5):534-45.
IJISRT22SEP696 www.ijisrt.com 1017
Volume 7, Issue 9, September – 2022 International Journal of Innovative Science and Research Technology
ISSN No:- 2456-2165
[8.] Bilimoria MM, Cormier JN, Mun Y, Lee JE, Evans [20.] Zhou W, Lv R, Wang X, Mou Y, Cai X, Herr I.
DB, Pisters PW. Pancreatic leak after left Stapler vs suture closure of pancreatic remnant after
pancreatectomy is reduced following main pancreatic distal pancreatectomy: a meta-analysis. The American
duct ligation. Br J Surg. 2003;90(2):190-6. Journal of Surgery. 2010;200(4):529-36.
[9.] Suc B, Msika S, Fingerhut A, Fourtanier G, Hay JM, [21.] Nathan H, Cameron JL, Goodwin CR, Seth AK, Edil
Holmières F, et al. Temporary fibrin glue occlusion of BH, Wolfgang CL, et al. Risk factors for pancreatic
the main pancreatic duct in the prevention of intra- leak after distal pancreatectomy. Ann Surg.
abdominal complications after pancreatic resection: 2009;250(2):277-81.
prospective randomized trial. Ann Surg. [22.] Fuks D, Piessen G, Huet E, Tavernier M, Zerbib P,
2003;237(1):57-65. Michot F, et al. Life-threatening postoperative
[10.] Hassenpflug M, Hartwig W, Strobel O, Hinz U, pancreatic fistula (grade C) after
Hackert T, Fritz S, et al. Decrease in clinically pancreaticoduodenectomy: incidence, prognosis, and
relevant pancreatic fistula by coverage of the risk factors. Am J Surg. 2009;197(6):702-9.
pancreatic remnant after distal pancreatectomy. [23.] Dellaportas D, Tympa A, Nastos C, Psychogiou V,
Surgery. 2012;152(3 Suppl 1):S164-71. Karakatsanis A, Polydorou A, et al. An ongoing
[11.] Oláh A, Issekutz A, Belágyi T, Hajdú N, Romics L, dispute in the management of severe pancreatic
Jr. Randomized clinical trial of techniques for closure fistula: Pancreatospleenectomy or not? World J
of the pancreatic remnant following distal Gastrointest Surg. 2010;2(11):381-4.
pancreatectomy. Br J Surg. 2009;96(6):602-7. [24.] Kent TS, Callery MP, Vollmer CM, Jr. The bridge
[12.] Diener MK, Seiler CM, Rossion I, Kleeff J, stent technique for salvage of pancreaticojejunal
Glanemann M, Butturini G, et al. Efficacy of stapler anastomotic dehiscence. HPB (Oxford).
versus hand-sewn closure after distal pancreatectomy 2010;12(8):577-82.
(DISPACT): a randomised, controlled multicentre [25.] Rudiš J, Ryska M. [Postoperative pancreatic fistula
trial. The Lancet. 2011;377(9776):1514-22. management by gastrofistuloanastomosis - a set of
[13.] Kuroki T, Eguchi S. Laparoscopic distal case reports]. Rozhl Chir. 2012;91(11):620-4.
pancreatosplenectomy for pancreatic ductal [26.] Vonlanthen R, Slankamenac K, Breitenstein S, Puhan
adenocarcinoma. Surgery Today. 2015;45(7):808-12. MA, Muller MK, Hahnloser D, et al. The impact of
[14.] Futagawa Y, Takano Y, Furukawa K, Kanehira M, complications on costs of major surgical procedures: a
Onda S, Sakamoto T, et al. Comparison of Outcomes cost analysis of 1200 patients. Annals of surgery.
with Hand-sewn <em>Versus</em> 2011;254(6):907-13.
Stapler Closure of Pancreatic Stump in Distal [27.] Hamilton NA, Porembka MR, Johnston FM, Gao F,
Pancreatectomy. Anticancer Research. Strasberg SM, Linehan DC, et al. Mesh reinforcement
2017;37(5):2515. of pancreatic transection decreases incidence of
[15.] Kawai M, Tani M, Yamaue H. Transection using pancreatic occlusion failure for left pancreatectomy: a
bipolar scissors reduces pancreatic fistula after distal single-blinded, randomized controlled trial. Annals of
pancreatectomy. Journal of Hepato-Biliary-Pancreatic surgery. 2012;255(6):1037.
Surgery. 2008;15(4):366-72. [28.] Hayashibe A, Ogino N. Clinical study for pancreatic
[16.] Suzuki Y, Kuroda Y, Morita A, Fujino Y, Tanioka Y, fistula after distal pancreatectomy with mesh
Kawamura T, et al. Fibrin Glue Sealing for the reinforcement. Asian Journal of Surgery.
Prevention of Pancreatic Fistulas Following Distal 2018;41(3):236-40.
Pancreatectomy. Archives of Surgery. [29.] Tillmann L-C, Herzog T, Uhl W, Belyaev O. Sealing
1995;130(9):952-5. with cyanoacrylate and a falciform patch cannot
[17.] Blansfield JA, Rapp MM, Chokshi RJ, Woll NL, prevent postoperative pancreatic fistula. World
Hunsinger MA, Sheldon DG, et al. Novel Method of Journal of Surgery. 2017;41(6):1601-9.
Stump Closure for Distal Pancreatectomy with a 75% [30.] Conlon KC, Labow D, Leung D, Smith A, Jarnagin
Reduction in Pancreatic Fistula Rate. Journal of W, Coit DG, et al. Prospective randomized clinical
Gastrointestinal Surgery. 2012;16(3):524-8. trial of the value of intraperitoneal drainage after
[18.] Hassenpflug M, Hartwig W, Strobel O, Hinz U, pancreatic resection. Annals of surgery.
Hackert T, Fritz S, et al. Decrease in clinically 2001;234(4):487.
relevant pancreatic fistula by coverage of the
pancreatic remnant after distal pancreatectomy.
Surgery. 2012;152(3):S164-S71.
[19.] Knaebel HP, Diener MK, Wente MN, Büchler MW,
Seiler CM. Systematic review and meta-analysis of
technique for closure of the pancreatic remnant after
distal pancreatectomy. British Journal of Surgery.
2005;92(5):539-46.
IJISRT22SEP696 www.ijisrt.com 1018
You might also like
- Laparoscopic Versus Open Cystogastrostomy For Pancreatic Pseudocysts A Comparative StudyDocument4 pagesLaparoscopic Versus Open Cystogastrostomy For Pancreatic Pseudocysts A Comparative StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Afferent Loop Decompression Technique Is Associated With A Reduction in Pancreatic Fistula Following PancreaticoduodenectomyDocument10 pagesAfferent Loop Decompression Technique Is Associated With A Reduction in Pancreatic Fistula Following PancreaticoduodenectomyDrDipesh Kumar YadavNo ratings yet
- A Prospective Treatment Protocol For Outpatient Laparoscopic Appendectomy For Acute AppendicitisDocument5 pagesA Prospective Treatment Protocol For Outpatient Laparoscopic Appendectomy For Acute AppendicitisBenjamin PaulinNo ratings yet
- Research Article: Pancreatoduodenectomy With or Without Pyloric Preservation: A Clinical Outcomes ComparisonDocument9 pagesResearch Article: Pancreatoduodenectomy With or Without Pyloric Preservation: A Clinical Outcomes ComparisonHiroj BagdeNo ratings yet
- 1 Bjs 10662Document8 pages1 Bjs 10662Vu Duy KienNo ratings yet
- Hepaticojejunostomy vs. Hepaticoduodenostomy After Excision of Choledochal Cyst in Paediatric Population - A Retrospective StudyDocument3 pagesHepaticojejunostomy vs. Hepaticoduodenostomy After Excision of Choledochal Cyst in Paediatric Population - A Retrospective StudyGagan DeepNo ratings yet
- Outpatient Laparoscopic Cholecystectomy: Experience of A University Group Practice in A Developing CountryDocument8 pagesOutpatient Laparoscopic Cholecystectomy: Experience of A University Group Practice in A Developing CountryNurlailah AliNo ratings yet
- Is Nasogastric Tube Necessary After Alimentary Tract Surgery?Document4 pagesIs Nasogastric Tube Necessary After Alimentary Tract Surgery?Coy EnNo ratings yet
- WarshawDocument11 pagesWarshawJuan RamirezNo ratings yet
- Pancreaticoduodenectomy or Whipple Procedure: Overview: by Dr. Sreeremya.S Faculty of BiologyDocument11 pagesPancreaticoduodenectomy or Whipple Procedure: Overview: by Dr. Sreeremya.S Faculty of BiologyKhuvindra Kevin Matai100% (1)
- Comparison of Perioperative Outcomes Between Laparoscopic and Open Approach For PancreatoduodenectomyDocument9 pagesComparison of Perioperative Outcomes Between Laparoscopic and Open Approach For PancreatoduodenectomyVu Duy KienNo ratings yet
- Annals of Medicine and SurgeryDocument4 pagesAnnals of Medicine and SurgeryRadu MiricaNo ratings yet
- WJG 20 7739Document14 pagesWJG 20 7739Rares MunteanuNo ratings yet
- The Comparison of Hand-Sewn and Stapled Anastomosis in EsophagectomyDocument4 pagesThe Comparison of Hand-Sewn and Stapled Anastomosis in EsophagectomyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unukovych 2016Document7 pagesUnukovych 2016jdavies231No ratings yet
- Anastomosis After LaparoscopicDocument16 pagesAnastomosis After LaparoscopicDuratul FahliaNo ratings yet
- Laparoscopic Partial Sleeve Duodenectomy (PSD) - Stauffer2013Document6 pagesLaparoscopic Partial Sleeve Duodenectomy (PSD) - Stauffer2013Joy GhoseNo ratings yet
- Urinary Lithiasis Conventional Open Surgery2020Revista Da Associacao Medica BrasileiraOpen AccessDocument5 pagesUrinary Lithiasis Conventional Open Surgery2020Revista Da Associacao Medica BrasileiraOpen Accessdev darma karinggaNo ratings yet
- 5794 22276 2 PBDocument4 pages5794 22276 2 PBalifa ishmahdinaNo ratings yet
- Advantages and Limitations of Endoscopic Septoplasty Experience of 120 CasesDocument6 pagesAdvantages and Limitations of Endoscopic Septoplasty Experience of 120 CasesInternational Journal of Innovative Science and Research Technology100% (1)
- Advantage and Limitation of Endoscopic SepDocument6 pagesAdvantage and Limitation of Endoscopic SepTareq MohammadNo ratings yet
- Minimally Invasive SurgeryDocument6 pagesMinimally Invasive SurgerycarmenNo ratings yet
- Implementation and Evaluation of A Clinical Pathway For Pancreaticoduodenectomy Procedures: A Prospective Cohort StudyDocument22 pagesImplementation and Evaluation of A Clinical Pathway For Pancreaticoduodenectomy Procedures: A Prospective Cohort StudyAndika FriyonNo ratings yet
- 3Document8 pages3polomska.kmNo ratings yet
- PAFMJ DecDocument5 pagesPAFMJ DecAhmed BazilNo ratings yet
- Okumura2018 Article ImpactOfDrainInsertionAfterPerDocument8 pagesOkumura2018 Article ImpactOfDrainInsertionAfterPernoskovNo ratings yet
- Laparoscopic Vs Open Appendectomy: Which Way To Go?Document22 pagesLaparoscopic Vs Open Appendectomy: Which Way To Go?fahryzal_noteNo ratings yet
- Perforated Peptic Ulcer - An Update: ArticleDocument14 pagesPerforated Peptic Ulcer - An Update: ArticleMuhammad ibnu kaesar PurbaNo ratings yet
- 8 Mai 2020Document3 pages8 Mai 2020Radu MiricaNo ratings yet
- Conservative Treatment of Early Postoperative Small Bowel Obstruction With Obliterative PeritonitisDocument10 pagesConservative Treatment of Early Postoperative Small Bowel Obstruction With Obliterative Peritonitisalemago90No ratings yet
- 2020-Bashah-Management After Sleeve GastrectomiDocument6 pages2020-Bashah-Management After Sleeve GastrectomiMariana Andrea BurgosNo ratings yet
- Journal Pre-Proof: Surgery in Practice and ScienceDocument20 pagesJournal Pre-Proof: Surgery in Practice and Sciencefidodido2000No ratings yet
- Pancreaticojejunostomy Conducive To Biological Healing in Minimally Invasive PancreaticoduodenectomyDocument15 pagesPancreaticojejunostomy Conducive To Biological Healing in Minimally Invasive PancreaticoduodenectomyCesar RcNo ratings yet
- Vitrectomy Combined With Posterior-Segment Ahmed Valve Implant: A Case Series StudyDocument8 pagesVitrectomy Combined With Posterior-Segment Ahmed Valve Implant: A Case Series StudyVlady BordaNo ratings yet
- IPEG Guidelines - AppendicitisDocument12 pagesIPEG Guidelines - AppendicitisHeru Sutanto KNo ratings yet
- Shyr 2021Document8 pagesShyr 2021Ruyu WangNo ratings yet
- Anestesia - Cardiovascular - Luna OrtizDocument11 pagesAnestesia - Cardiovascular - Luna OrtizWeimar Andres Bonilla MosqueraNo ratings yet
- International Journal of Surgery Open: Tariq Al-Aubaidi, Basim R. Ghadhban, Samer S. ChitheerDocument7 pagesInternational Journal of Surgery Open: Tariq Al-Aubaidi, Basim R. Ghadhban, Samer S. Chitheersamer falconNo ratings yet
- Journal of Pediatric Surgery: Laura Baker, Alana L. Beres, Robert BairdDocument8 pagesJournal of Pediatric Surgery: Laura Baker, Alana L. Beres, Robert BairdHenry BarberenaNo ratings yet
- Outcomes of Endoscopic Ultrasound-Guided Biliary Drainage: A Systematic Review and Meta-AnalysisDocument9 pagesOutcomes of Endoscopic Ultrasound-Guided Biliary Drainage: A Systematic Review and Meta-AnalysisAfkar30No ratings yet
- Nso ErcpDocument3 pagesNso Ercptry dokkNo ratings yet
- Endoscopic Management in The Bariatric Surgical Patient: Benjamin E. Levitzky and Wahid Y. WassefDocument8 pagesEndoscopic Management in The Bariatric Surgical Patient: Benjamin E. Levitzky and Wahid Y. Wasseflourdes marquezNo ratings yet
- Versus: Laparoscopic Open Appendectomy: Which Way To Go?Document6 pagesVersus: Laparoscopic Open Appendectomy: Which Way To Go?Claudiu Ungureanu ClauNo ratings yet
- Original Research ArticleDocument9 pagesOriginal Research ArticleAnand ShanmugaiahNo ratings yet
- Effects of Weight Loss On Acoustic Parameters After Bariatric SurgeryDocument2 pagesEffects of Weight Loss On Acoustic Parameters After Bariatric SurgeryTony Miguel Saba SabaNo ratings yet
- Posthepatectomy Liver Failure: A Definition and Grading by The International Study Group of Liver Surgery (ISGLS)Document12 pagesPosthepatectomy Liver Failure: A Definition and Grading by The International Study Group of Liver Surgery (ISGLS)drsubramanianNo ratings yet
- Repair of Bowel Perforation Endoscopic State of The ArtDocument6 pagesRepair of Bowel Perforation Endoscopic State of The ArtAthenaeum Scientific PublishersNo ratings yet
- Prospective StudyDocument23 pagesProspective Studyjumatika91No ratings yet
- Aliment Pharmacol Ther - 2022 - Tergast - Home Based Tunnelled Peritoneal Drainage System As An Alternative TreatmentDocument11 pagesAliment Pharmacol Ther - 2022 - Tergast - Home Based Tunnelled Peritoneal Drainage System As An Alternative TreatmentTens AiepNo ratings yet
- Art07 PDFDocument6 pagesArt07 PDFadan2010No ratings yet
- SurgeryDocument7 pagesSurgeryFrancisco GilNo ratings yet
- Distal Pancreatectomy Outcomes: Perspectives From A Community-Based Teaching InstitutionDocument6 pagesDistal Pancreatectomy Outcomes: Perspectives From A Community-Based Teaching InstitutionmfachrezaaNo ratings yet
- Is 9Document9 pagesIs 9intan juitaNo ratings yet
- LAPAROSDocument13 pagesLAPAROSpancholin_9No ratings yet
- 2020-01 - Endoscopic Retrograde Cholangiopancreatography in Recurrent Acute Pancreatitis - Determining The Optimal Subgroup of Patients in Whom The Procedure Is BeneficialDocument2 pages2020-01 - Endoscopic Retrograde Cholangiopancreatography in Recurrent Acute Pancreatitis - Determining The Optimal Subgroup of Patients in Whom The Procedure Is BeneficialNawzad SulayvaniNo ratings yet
- Yeh 2019Document5 pagesYeh 2019sigitdwimulyoNo ratings yet
- Medicina: Is It Safe To Combine A Fundoplication To Sleeve Gastrectomy? Review of LiteratureDocument7 pagesMedicina: Is It Safe To Combine A Fundoplication To Sleeve Gastrectomy? Review of LiteratureRadu MiricaNo ratings yet
- Laparoscopic OvariectomíaDocument15 pagesLaparoscopic Ovariectomíasimon alfaro gonzálezNo ratings yet
- Risk Factors For Pancreatic FistulaDocument6 pagesRisk Factors For Pancreatic Fistulahenok seifeNo ratings yet
- Laparoscopic Sleeve GastrectomyFrom EverandLaparoscopic Sleeve GastrectomySalman Al-SabahNo ratings yet
- Detection of Phishing WebsitesDocument6 pagesDetection of Phishing WebsitesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Vertical Farming System Based on IoTDocument6 pagesVertical Farming System Based on IoTInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Detection and Counting of Fake Currency & Genuine Currency Using Image ProcessingDocument6 pagesDetection and Counting of Fake Currency & Genuine Currency Using Image ProcessingInternational Journal of Innovative Science and Research Technology100% (9)
- Osho Dynamic Meditation; Improved Stress Reduction in Farmer Determine by using Serum Cortisol and EEG (A Qualitative Study Review)Document8 pagesOsho Dynamic Meditation; Improved Stress Reduction in Farmer Determine by using Serum Cortisol and EEG (A Qualitative Study Review)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Influence of Principals’ Promotion of Professional Development of Teachers on Learners’ Academic Performance in Kenya Certificate of Secondary Education in Kisii County, KenyaDocument13 pagesInfluence of Principals’ Promotion of Professional Development of Teachers on Learners’ Academic Performance in Kenya Certificate of Secondary Education in Kisii County, KenyaInternational Journal of Innovative Science and Research Technology100% (1)
- The Impact of Music on Orchid plants Growth in Polyhouse EnvironmentsDocument5 pagesThe Impact of Music on Orchid plants Growth in Polyhouse EnvironmentsInternational Journal of Innovative Science and Research Technology100% (1)
- Consistent Robust Analytical Approach for Outlier Detection in Multivariate Data using Isolation Forest and Local Outlier FactorDocument5 pagesConsistent Robust Analytical Approach for Outlier Detection in Multivariate Data using Isolation Forest and Local Outlier FactorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Realigning Curriculum to Simplify the Challenges of Multi-Graded Teaching in Government Schools of KarnatakaDocument5 pagesRealigning Curriculum to Simplify the Challenges of Multi-Graded Teaching in Government Schools of KarnatakaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Sustainable Energy Consumption Analysis through Data Driven InsightsDocument16 pagesSustainable Energy Consumption Analysis through Data Driven InsightsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Entrepreneurial Creative Thinking and Venture Performance: Reviewing the Influence of Psychomotor Education on the Profitability of Small and Medium Scale Firms in Port Harcourt MetropolisDocument10 pagesEntrepreneurial Creative Thinking and Venture Performance: Reviewing the Influence of Psychomotor Education on the Profitability of Small and Medium Scale Firms in Port Harcourt MetropolisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Overview of Lung CancerDocument6 pagesAn Overview of Lung CancerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Digital Finance-Fintech and it’s Impact on Financial Inclusion in IndiaDocument10 pagesDigital Finance-Fintech and it’s Impact on Financial Inclusion in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Stress and Emotional Reactions due to the Covid-19 Pandemic in IndiaDocument6 pagesImpact of Stress and Emotional Reactions due to the Covid-19 Pandemic in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Utilization of Waste Heat Emitted by the KilnDocument2 pagesUtilization of Waste Heat Emitted by the KilnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Efficient Cloud-Powered Bidding MarketplaceDocument5 pagesAn Efficient Cloud-Powered Bidding MarketplaceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Designing Cost-Effective SMS based Irrigation System using GSM ModuleDocument8 pagesDesigning Cost-Effective SMS based Irrigation System using GSM ModuleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Effect of Solid Waste Management on Socio-Economic Development of Urban Area: A Case of Kicukiro DistrictDocument13 pagesEffect of Solid Waste Management on Socio-Economic Development of Urban Area: A Case of Kicukiro DistrictInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predictive Analytics for Motorcycle Theft Detection and RecoveryDocument5 pagesPredictive Analytics for Motorcycle Theft Detection and RecoveryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Auto Tix: Automated Bus Ticket SolutionDocument5 pagesAuto Tix: Automated Bus Ticket SolutionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Examining the Benefits and Drawbacks of the Sand Dam Construction in Cadadley RiverbedDocument8 pagesExamining the Benefits and Drawbacks of the Sand Dam Construction in Cadadley RiverbedInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ambulance Booking SystemDocument7 pagesAmbulance Booking SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparative Evaluation of Action of RISA and Sodium Hypochlorite on the Surface Roughness of Heat Treated Single Files, Hyflex EDM and One Curve- An Atomic Force Microscopic StudyDocument5 pagesComparative Evaluation of Action of RISA and Sodium Hypochlorite on the Surface Roughness of Heat Treated Single Files, Hyflex EDM and One Curve- An Atomic Force Microscopic StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Study Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoDocument6 pagesStudy Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Computer Vision Gestures Recognition System Using Centralized Cloud ServerDocument9 pagesComputer Vision Gestures Recognition System Using Centralized Cloud ServerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cyber Security Awareness and Educational Outcomes of Grade 4 LearnersDocument33 pagesCyber Security Awareness and Educational Outcomes of Grade 4 LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Forensic Advantages and Disadvantages of Raman Spectroscopy Methods in Various Banknotes Analysis and The Observed Discordant ResultsDocument12 pagesForensic Advantages and Disadvantages of Raman Spectroscopy Methods in Various Banknotes Analysis and The Observed Discordant ResultsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Blockchain Based Decentralized ApplicationDocument7 pagesBlockchain Based Decentralized ApplicationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Industry That Capitalizes Off of Women's Insecurities?Document8 pagesAn Industry That Capitalizes Off of Women's Insecurities?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Factors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaDocument6 pagesFactors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unmasking Phishing Threats Through Cutting-Edge Machine LearningDocument8 pagesUnmasking Phishing Threats Through Cutting-Edge Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ISRAEL PowerpointDocument86 pagesISRAEL PowerpointRamprasad AkshantulaNo ratings yet
- Assignment On Neurological AssessmentDocument20 pagesAssignment On Neurological AssessmentSumandeep KaurNo ratings yet
- CHARLOTTEDocument18 pagesCHARLOTTEravenNo ratings yet
- Aft MPM Cafs 01Document2 pagesAft MPM Cafs 01Forum PompieriiNo ratings yet
- Production and Industrial EngineeringDocument27 pagesProduction and Industrial EngineeringShivangi MishraNo ratings yet
- Advanced IC Engines: Prof. R. Devaraj Dr. S. Ramachandran Dr. A. AndersonDocument61 pagesAdvanced IC Engines: Prof. R. Devaraj Dr. S. Ramachandran Dr. A. AndersonGopi KrishnanNo ratings yet
- Systemic Functional Grammar: A First Step Into The Theory:, IncludingDocument31 pagesSystemic Functional Grammar: A First Step Into The Theory:, Includingnona nonaNo ratings yet
- Service Tool Screens: JS1 PVE JoystickDocument20 pagesService Tool Screens: JS1 PVE JoystickPitupyNo ratings yet
- Kingdoms of FlameDocument133 pagesKingdoms of Flamerobi255167% (3)
- 2 and Lehr Panzerdivison PDFDocument38 pages2 and Lehr Panzerdivison PDFLeonte Daniel100% (1)
- Wallace State Community College NURSING DATABASE: Nursing HomeDocument9 pagesWallace State Community College NURSING DATABASE: Nursing HomeEnger NushunNo ratings yet
- UGNEWRevisedFinalII IVVI TimeTableAug, Sept03.08.2021Document10 pagesUGNEWRevisedFinalII IVVI TimeTableAug, Sept03.08.2021siva pkbkNo ratings yet
- Black 1950 PDFDocument10 pagesBlack 1950 PDFcis freteNo ratings yet
- Compound Plamar GanglionDocument4 pagesCompound Plamar Ganglionchinmayghaisas100% (2)
- Lecture 1 TF BiomechanicsDocument63 pagesLecture 1 TF BiomechanicsAlfred JacksonNo ratings yet
- Atmel 11121 32 Bit Cortex A5 Microcontroller SAMA5D3 DatasheetDocument1,710 pagesAtmel 11121 32 Bit Cortex A5 Microcontroller SAMA5D3 DatasheetCan CerberusNo ratings yet
- ERAS DR - TESAR SP - AnDocument26 pagesERAS DR - TESAR SP - AnAhmad Rifai R ANo ratings yet
- Bio AdhesiveDocument24 pagesBio AdhesiveNavreet BdaengNo ratings yet
- ComantDocument134 pagesComantsoniaxNo ratings yet
- Operations Management ComprehensiveDocument9 pagesOperations Management ComprehensiveashishNo ratings yet
- LE Handicraft WEEK 3-4 GRADE 7 - 8Document6 pagesLE Handicraft WEEK 3-4 GRADE 7 - 8Michelle Llanes100% (1)
- Dissertation Abstracts International Section B Sciences and EngineeringDocument5 pagesDissertation Abstracts International Section B Sciences and EngineeringCustomPapersWritingSingaporeNo ratings yet
- Dual Operational Amplifier: NJM4560D, NJM4560M, NJM4560E NJM4560LDocument4 pagesDual Operational Amplifier: NJM4560D, NJM4560M, NJM4560E NJM4560LPablo Diego Cecere CasadoNo ratings yet
- Biology AS ClassifiedDocument209 pagesBiology AS ClassifiedMaaz Rashid100% (2)
- Robotic: Differential Motion and JacobianDocument37 pagesRobotic: Differential Motion and Jacobian李尚倫33% (3)
- The Said and The UnsaidDocument19 pagesThe Said and The UnsaidOzana BudauNo ratings yet
- Lab ReportDocument17 pagesLab ReportHabtamu BaynekawNo ratings yet
- Khady's Class Plan PDFDocument11 pagesKhady's Class Plan PDFKhadija RezkNo ratings yet
- TEGOPAC Bond251 012016Document2 pagesTEGOPAC Bond251 012016Pranshu JainNo ratings yet
- Bevel Gear Drive Screw Jack 6000Document5 pagesBevel Gear Drive Screw Jack 6000Elias YeshiwasNo ratings yet