You might also like
- Daily Work ActivityDocument8 pagesDaily Work Activityrussel aquinoNo ratings yet
- Daily Work ActivityDocument1 pageDaily Work ActivityJim C. ValenciaNo ratings yet
- Technological University of The PhilippinesDocument1 pageTechnological University of The PhilippinesPaula CurayagNo ratings yet
- F IRJ 6.6 SJR - Student Job ReportDocument10 pagesF IRJ 6.6 SJR - Student Job ReportwijawijaNo ratings yet
- F IRJ 6.6 SJR - Student Job Report 1Document1 pageF IRJ 6.6 SJR - Student Job Report 1Aldrian BarachinaNo ratings yet
- Weekly Timesheet: Name: Date: Badge #: Dept: ManagerDocument2 pagesWeekly Timesheet: Name: Date: Badge #: Dept: ManagerShaira Nicole PelaezNo ratings yet
- QuestionnareDocument3 pagesQuestionnareVridhi AroraNo ratings yet
- Employee Name: Month: Manager Name: Rate Per Hour:: Week Starting Hours Worked Total PayDocument8 pagesEmployee Name: Month: Manager Name: Rate Per Hour:: Week Starting Hours Worked Total PayHatem HusseinNo ratings yet
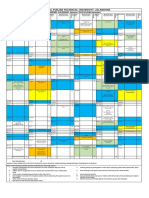
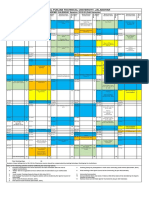
- I.K. Gujral Punjab Technical University, Jalandhar: ACADEMIC CALENDAR Session: 2019-20 (Odd Semester)Document1 pageI.K. Gujral Punjab Technical University, Jalandhar: ACADEMIC CALENDAR Session: 2019-20 (Odd Semester)charu sharmaNo ratings yet
- Academic Calendar July-Nov 2019Document1 pageAcademic Calendar July-Nov 2019Surjit Kumar GandhiNo ratings yet
- Jahanvi ISPAT Weekely ReportDocument1 pageJahanvi ISPAT Weekely ReportRohan ChouhanNo ratings yet
- Wages English2017Document3 pagesWages English2017Martin Kvisvik LarsenNo ratings yet
- I Trimmed Up My Mug, Made and Attached A Handle, and Glazed The BowlDocument1 pageI Trimmed Up My Mug, Made and Attached A Handle, and Glazed The Bowlapi-591482404No ratings yet
- B1 Photocopiables VocabularyDocument16 pagesB1 Photocopiables VocabularyMariaNo ratings yet
- B1 Photocopiables VocabularyDocument16 pagesB1 Photocopiables VocabularyTeresa EscardóNo ratings yet
- B1 Photocopiables GrammarDocument23 pagesB1 Photocopiables GrammarTeresa EscardóNo ratings yet
- Photocopiable Activities: Tips For Using Communicative ActivitiesDocument23 pagesPhotocopiable Activities: Tips For Using Communicative ActivitiesJuan Manuel Mayo Romero100% (1)
- B1 Photocopiables CommunicativeDocument24 pagesB1 Photocopiables CommunicativeLuisa RSNo ratings yet
- Job Report IanDocument7 pagesJob Report IanIan GAMINGNo ratings yet
- Enterprise and Employability Challenge Candidate BookletDocument7 pagesEnterprise and Employability Challenge Candidate BookletalfieNo ratings yet
- Spun Another MugDocument1 pageSpun Another Mugapi-591482404No ratings yet
- Simple PresentDocument2 pagesSimple PresentPatrícia TeixeiraNo ratings yet
- HP Pavilion X 360 Convertible PCDocument7 pagesHP Pavilion X 360 Convertible PCSyed ZamanNo ratings yet
- Actioned By: Task Schedule / Description Information Required Materials Required Additional Notes N.O.TDocument1 pageActioned By: Task Schedule / Description Information Required Materials Required Additional Notes N.O.TMike RaymondNo ratings yet
- Senior Project Journal Documentation 16Document1 pageSenior Project Journal Documentation 16api-591823718No ratings yet
- Amdm Budget ProjectDocument10 pagesAmdm Budget Projectapi-519218367No ratings yet
- Task - Work Timeable EmailDocument7 pagesTask - Work Timeable EmailTania Nayeli DuqueNo ratings yet
- FAQs - Position Management PDFDocument6 pagesFAQs - Position Management PDFSwathi BinduNo ratings yet
- Site Manhours SF 4701Document31 pagesSite Manhours SF 4701Anonymous kuW0obtJ4pNo ratings yet
- Weekly Plan Learning Objectives Learning Sequence Assessment Task Learning Experiences Material - ResourceDocument5 pagesWeekly Plan Learning Objectives Learning Sequence Assessment Task Learning Experiences Material - ResourceInaNo ratings yet
- Employee Name: Manager Name: Week Starting:: Date Day Time in Time Out Time in Time Out Total HoursDocument3 pagesEmployee Name: Manager Name: Week Starting:: Date Day Time in Time Out Time in Time Out Total HoursCeasar Neil SaysonNo ratings yet
- Domain 5Document5 pagesDomain 5api-438623441No ratings yet
- Made A Bowl and A MugDocument1 pageMade A Bowl and A Mugapi-591482404No ratings yet
- Let Me Give You My Card: Unit UnitDocument3 pagesLet Me Give You My Card: Unit Unitkitisuda parnkulNo ratings yet
- Immersion Logbook MENTALDocument5 pagesImmersion Logbook MENTALmartNo ratings yet
- Relationship Saving Activity PlannerDocument16 pagesRelationship Saving Activity PlannerGoma LaweNo ratings yet
- Joseph I Was Not His Father He Was Mine Michael Mclean-1Document6 pagesJoseph I Was Not His Father He Was Mine Michael Mclean-1Gloria SánchezNo ratings yet
- Daily Planner Weekly Planner Monthly PlannerDocument2 pagesDaily Planner Weekly Planner Monthly PlannerJohn Lesther PabiloniaNo ratings yet
- E1 - STOCURI PRODUCTIE - Inventories WIPDocument1 pageE1 - STOCURI PRODUCTIE - Inventories WIPovidiu.tisloveanuNo ratings yet
- 6 Daily Performance Monitoring 101716Document2 pages6 Daily Performance Monitoring 101716Godfrey VelozNo ratings yet
- Copia de 15160068 - 15160011 - 1516067 Calificaciones MOD 2.1Document7 pagesCopia de 15160068 - 15160011 - 1516067 Calificaciones MOD 2.1Rafael RojasNo ratings yet
- Ism Report Attendance ListDocument1 pageIsm Report Attendance ListHassan KhanNo ratings yet
- Vacation-PTO Request Form-Dec 05, 2017Document1 pageVacation-PTO Request Form-Dec 05, 2017Shadul UsmanNo ratings yet
- Run Chart - Lead TimeDocument2 pagesRun Chart - Lead TimeAndreea HavrișciucNo ratings yet
- Weekly Work PlanDocument2 pagesWeekly Work PlanJoe AguilarNo ratings yet
- Miami-Dade County Public Schools Data Collection: LatencyDocument2 pagesMiami-Dade County Public Schools Data Collection: Latencyapi-518977559No ratings yet
- Project ManagementDocument1 pageProject ManagementProxyYtNo ratings yet
- Sle ProposalDocument3 pagesSle Proposalapi-434223284No ratings yet
- Summary of Activities Working Day: Tuesday-Friday Date Working Summary/ Daily ActivitiesDocument4 pagesSummary of Activities Working Day: Tuesday-Friday Date Working Summary/ Daily ActivitiesAniq AmmarNo ratings yet
- Time ManagementDocument8 pagesTime ManagementdragonzeeeNo ratings yet
- Sharikat Fanniya Omaniya LLC: Man-Hour For The Month of June 2020Document2 pagesSharikat Fanniya Omaniya LLC: Man-Hour For The Month of June 2020Sriram BaskaranNo ratings yet
- Attendance Register Cum PayslipDocument13 pagesAttendance Register Cum PayslipHaider50% (2)
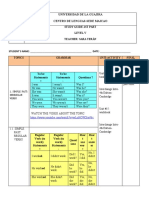
- Universidad de La Guajira Centro de Lenguas-Sede Maicao: Study Guide-1St Part Level V Teacher: Sara TeránDocument12 pagesUniversidad de La Guajira Centro de Lenguas-Sede Maicao: Study Guide-1St Part Level V Teacher: Sara TeránGehiler C'otesNo ratings yet
- 4 3soptool-ProbationperiodresultDocument3 pages4 3soptool-ProbationperiodresultPabloNo ratings yet
- Return Experience Map - Desonance - Nov 11Document1 pageReturn Experience Map - Desonance - Nov 11wenli suNo ratings yet
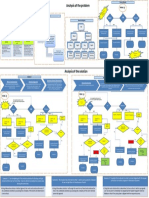
- MIS-730 Personal Information System: Analysis of The ProblemDocument1 pageMIS-730 Personal Information System: Analysis of The ProblemDASHPAGALNo ratings yet
- Skills Audit FormDocument10 pagesSkills Audit FormPurwanto Soe'ebNo ratings yet
- Universidad de La Guajira Centro de Lenguas-Sede Maicao: Study Guide-1St Part Level V Teacher: Sara TeránDocument33 pagesUniversidad de La Guajira Centro de Lenguas-Sede Maicao: Study Guide-1St Part Level V Teacher: Sara TerányarinethNo ratings yet
- Chau Thi Ngoc Quyen HRBP SpecialistDocument3 pagesChau Thi Ngoc Quyen HRBP SpecialistPhuong TranNo ratings yet
- Referral BrgyDocument1 pageReferral BrgyGene CaryNo ratings yet
- Updated MoaDocument6 pagesUpdated MoaGene CaryNo ratings yet
- Application Form Form 1-2Document2 pagesApplication Form Form 1-2Gene CaryNo ratings yet
- Endorsement LetterDocument1 pageEndorsement LetterGene CaryNo ratings yet
- Updated MoaDocument6 pagesUpdated MoaGene CaryNo ratings yet