You might also like
- Mindfulness PDFDocument7 pagesMindfulness PDFDaniel DragulescuNo ratings yet
- 2009 Language-Based Measures of Mindfulness Initial Validity and Clinical UtilityDocument4 pages2009 Language-Based Measures of Mindfulness Initial Validity and Clinical UtilityalotfyaNo ratings yet
- Speech 2nd JulyDocument3 pagesSpeech 2nd JulyAndriNo ratings yet
- Feature Mindfulness Based Cancer RecoveryDocument5 pagesFeature Mindfulness Based Cancer RecoveryR.GamageNo ratings yet
- ! Mindfulness VS Control Pone.0097551Document11 pages! Mindfulness VS Control Pone.0097551Stela PenkovaNo ratings yet
- What Do We Really Know About Mindfulnessbased Stress ReductionDocument14 pagesWhat Do We Really Know About Mindfulnessbased Stress ReductionCody WilliamsNo ratings yet
- Complementary Therapies in Clinical Practice: Patricia L. Dobkin, Qinyi ZhaoDocument6 pagesComplementary Therapies in Clinical Practice: Patricia L. Dobkin, Qinyi ZhaoMonica MenaNo ratings yet
- Mclaughlin Revised Professional Audience PieceDocument10 pagesMclaughlin Revised Professional Audience Pieceapi-625527319No ratings yet
- Mindfulness-Based Stress Reduction and Health Benefits A Meta-AnalysisDocument9 pagesMindfulness-Based Stress Reduction and Health Benefits A Meta-AnalysisVladNo ratings yet
- Effect of Sahaja Yoga Meditation On Quality of LifeDocument8 pagesEffect of Sahaja Yoga Meditation On Quality of LifeVladimir SutanovacNo ratings yet
- CHN LNW EbjDocument3 pagesCHN LNW EbjJacovNo ratings yet
- Major Research Findings - CFM - UMass Medical School - WorcesterDocument2 pagesMajor Research Findings - CFM - UMass Medical School - WorcesterJack LiuNo ratings yet
- 2000 MICHAEL SPECA - A Randomized, Wait-List Controlled Clinical Trial The Effect of A MindfulnessDocument10 pages2000 MICHAEL SPECA - A Randomized, Wait-List Controlled Clinical Trial The Effect of A Mindfulnessnermal93No ratings yet
- Acta Psychiatr Scand - 2011 - Fjorback - Mindfulness Based Stress Reduction and Mindfulness Based Cognitive Therapy ADocument18 pagesActa Psychiatr Scand - 2011 - Fjorback - Mindfulness Based Stress Reduction and Mindfulness Based Cognitive Therapy Amgomez2019No ratings yet
- Add 12140Document9 pagesAdd 12140imadhassanNo ratings yet
- Kindness Based MeditationDocument46 pagesKindness Based MeditationAlvinNo ratings yet
- MINDSENS Composit Index de Algunos Items Del FFMQ y EQ Sensible A Interv PDFDocument7 pagesMINDSENS Composit Index de Algunos Items Del FFMQ y EQ Sensible A Interv PDFIgnacio PisanoNo ratings yet
- 40631665-Review Mindfulness Si Cancer PDFDocument10 pages40631665-Review Mindfulness Si Cancer PDFadri90No ratings yet
- Intervention For Smoking ReductionDocument15 pagesIntervention For Smoking Reductionben mwanziaNo ratings yet
- tmpF7A9 TMPDocument2 pagestmpF7A9 TMPFrontiersNo ratings yet
- Cognitive Behavioural Strategies For General PracticeDocument7 pagesCognitive Behavioural Strategies For General PracticeArturo MelgarNo ratings yet
- Meditation: Nccih - Nih.govDocument8 pagesMeditation: Nccih - Nih.govDianaLupascoNo ratings yet
- Mindfulness - Substance Abuse in A Therapeutic CommunityDocument6 pagesMindfulness - Substance Abuse in A Therapeutic CommunityCarmo de SousaNo ratings yet
- 1529 FTPDocument12 pages1529 FTPPreda LoredanaNo ratings yet
- Child Adolesc Psychiatr Clin N Am 2020 29 1 211-23Document13 pagesChild Adolesc Psychiatr Clin N Am 2020 29 1 211-23Fernando SousaNo ratings yet
- Ayurveda and Panchakarma: Measuring The Effects of A Holistic Health InterventionDocument10 pagesAyurveda and Panchakarma: Measuring The Effects of A Holistic Health InterventionmadhulikkaNo ratings yet
- Wa0045.Document4 pagesWa0045.Arooj MughalNo ratings yet
- Facilitated Pa-Depression-2Document13 pagesFacilitated Pa-Depression-2api-332791374No ratings yet
- Cognitive-Behavioral Therapy For Somatization Disorder: A Randomized Controlled TrialDocument7 pagesCognitive-Behavioral Therapy For Somatization Disorder: A Randomized Controlled TrialMuhammad Bayu WNo ratings yet
- MBSR For Chronic IllnessDocument5 pagesMBSR For Chronic IllnessYudith LouisaNo ratings yet
- 337 FullDocument10 pages337 FullDaniel RojasNo ratings yet
- Self Management Program Among Type 2 Diabetes Mellitus Patients: A Literature ReviewDocument6 pagesSelf Management Program Among Type 2 Diabetes Mellitus Patients: A Literature Reviewbardah wasalamahNo ratings yet
- Benzo 2013 PDFDocument8 pagesBenzo 2013 PDFRAMONA GABRIELA LEBADANo ratings yet
- Jurnal 1.4 yDocument20 pagesJurnal 1.4 yAmbarsari HamidahNo ratings yet
- Cognitive Behavioral TheoryDocument3 pagesCognitive Behavioral TheoryLyzajoyce SeriozaNo ratings yet
- Biopsychosocial Model of HealthDocument10 pagesBiopsychosocial Model of HealthDavin DoNo ratings yet
- Alzh 1 ART Intervenciones Psicosocial y Conductual en Demencia-BurnsDocument5 pagesAlzh 1 ART Intervenciones Psicosocial y Conductual en Demencia-BurnsKitzia AveiriNo ratings yet
- The Healthy Lifestyle and Personal Control QuestionnaireDocument28 pagesThe Healthy Lifestyle and Personal Control QuestionnaireDon Chiaw Manongdo50% (2)
- C Langeland, E., Riise, T., Hanestad, B. R., Nortvedt, M. W., Kristoffersen, K., & Wahl, A. K. (2006) .Document8 pagesC Langeland, E., Riise, T., Hanestad, B. R., Nortvedt, M. W., Kristoffersen, K., & Wahl, A. K. (2006) .Ign EcheverríaNo ratings yet
- Appi Ps 201400535 PDFDocument6 pagesAppi Ps 201400535 PDFArif IrpanNo ratings yet
- 1 s2.0 S0022399920301847 MainDocument10 pages1 s2.0 S0022399920301847 MainMaria SilaghiNo ratings yet
- Mindfulness in Primary School Children ADocument15 pagesMindfulness in Primary School Children AMuhammad Irfan AneesNo ratings yet
- The Hawthorne Effect 2Document8 pagesThe Hawthorne Effect 2David FanelNo ratings yet
- Predictors of Psych Intervention To Promote Health Behaviour Adherence in HF 2021Document14 pagesPredictors of Psych Intervention To Promote Health Behaviour Adherence in HF 2021Bob JoeNo ratings yet
- DK Positive Psychological Functioning With MBSR 17Document1 pageDK Positive Psychological Functioning With MBSR 17Swami-NeoNo ratings yet
- The Journal of Alternative and Complementary MedicineDocument7 pagesThe Journal of Alternative and Complementary Medicineharshadpardeshi45No ratings yet
- Feeling GreatDocument243 pagesFeeling GreatSunny LamNo ratings yet
- Blodgett Et Al. (2022) .What Works To Improve Wellbeing - A Rapid Systematic Review of 223 Interventions Evaluated With The - ScalesDocument27 pagesBlodgett Et Al. (2022) .What Works To Improve Wellbeing - A Rapid Systematic Review of 223 Interventions Evaluated With The - ScalesJosh CarrNo ratings yet
- Mental Health First Aid Training: Review of Evaluation StudiesDocument3 pagesMental Health First Aid Training: Review of Evaluation StudiesLiz RoxNo ratings yet
- MBCT in OCDDocument10 pagesMBCT in OCDRoxi ResurreccionNo ratings yet
- Presentation-WBT PrevDocument12 pagesPresentation-WBT Previn UBBPNo ratings yet
- Landsman Dijkstra2006Document14 pagesLandsman Dijkstra2006Hegymegi-Kiss DalmaNo ratings yet
- Evaluation of A Sudarshan Kriya Yoga (SKY) Based Breath Intervention For Patients With Mild-To-Moderate Depression and Anxiety DisordersDocument8 pagesEvaluation of A Sudarshan Kriya Yoga (SKY) Based Breath Intervention For Patients With Mild-To-Moderate Depression and Anxiety Disorderssankapalrutik10No ratings yet
- ProposalDocument3 pagesProposalAbdullahAlmasNo ratings yet
- Chan Wu YiDocument8 pagesChan Wu YiAlejandra SacanellNo ratings yet
- Huang 2016Document9 pagesHuang 2016backup datadindaNo ratings yet
- Contemporary Clinical TrialsDocument8 pagesContemporary Clinical TrialsAzisahhNo ratings yet
- Mindfulness BasedStressReductiDocument8 pagesMindfulness BasedStressReductiRev NandacaraNo ratings yet
- Marlatt Vipassana BUONISSIMODocument12 pagesMarlatt Vipassana BUONISSIMOMauri Passariello LaezzaNo ratings yet
- Mindfulness Articolo IngleseDocument3 pagesMindfulness Articolo IngleseMauri Passariello LaezzaNo ratings yet
- Smoking MindfulnessDocument9 pagesSmoking MindfulnessMauri Passariello LaezzaNo ratings yet
- Fumo GravidanzaDocument4 pagesFumo GravidanzaMauri Passariello LaezzaNo ratings yet
- Mindfulness SubstanceDocument17 pagesMindfulness SubstanceMauri Passariello LaezzaNo ratings yet
- Mindfulness Addict Review BUONISSIMODocument33 pagesMindfulness Addict Review BUONISSIMOMauri Passariello LaezzaNo ratings yet
- Mindfulness Alcol 2Document17 pagesMindfulness Alcol 2Mauri Passariello LaezzaNo ratings yet
- Santa Claus Is Coming To TownDocument4 pagesSanta Claus Is Coming To TownMauri Passariello Laezza100% (4)
- Mindfulness: 1. What Is Mindfulness? 2. Benefits of Mindfulness 3. Applications of Mindfulness TrainingDocument44 pagesMindfulness: 1. What Is Mindfulness? 2. Benefits of Mindfulness 3. Applications of Mindfulness TrainingMauri Passariello LaezzaNo ratings yet
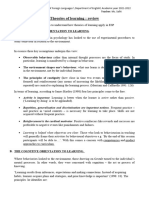
- Lesson 5 Theories of Learning and ESPDocument5 pagesLesson 5 Theories of Learning and ESPRaouf CarloNo ratings yet
- FINALS LESSON 2 in Personality DevelopmentDocument39 pagesFINALS LESSON 2 in Personality DevelopmentAllison TachibananNo ratings yet
- 1-6 UTS Guzman - 3Document2 pages1-6 UTS Guzman - 3Krizzy GuzmanNo ratings yet
- Psykolog Complicated Grief Therapy (CGT) - A Novel Third Wave CBT For ProDocument3 pagesPsykolog Complicated Grief Therapy (CGT) - A Novel Third Wave CBT For ProRob KorényiNo ratings yet
- Neck Houghton 2006Document27 pagesNeck Houghton 2006Hninnandar WinNo ratings yet
- TOP KleinHorneyDocument3 pagesTOP KleinHorneyCamae Snyder GangcuangcoNo ratings yet
- Customer SatisfactionDocument34 pagesCustomer SatisfactionSARA JANE CAMBRONERONo ratings yet
- BCAAN ConsentForm May 2020 FillableDocument3 pagesBCAAN ConsentForm May 2020 FillableAshley LehmanNo ratings yet
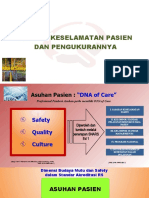
- Xxxxxxbudaya Keselamatan Pasien Dan PengukurannyaDocument59 pagesXxxxxxbudaya Keselamatan Pasien Dan Pengukurannyaputri panji lestariNo ratings yet
- Small Group Counseling For Relational Aggressive Girls: Salvaging SisterhoodDocument28 pagesSmall Group Counseling For Relational Aggressive Girls: Salvaging SisterhoodNur MuhainiNo ratings yet
- Problem Within Family, Family Violence (Muhamad Mufqi Zaidan)Document4 pagesProblem Within Family, Family Violence (Muhamad Mufqi Zaidan)mufqyNo ratings yet
- Motivating Factors For Seeking Cosmetic SurgeryDocument6 pagesMotivating Factors For Seeking Cosmetic SurgeryfumblefumbleNo ratings yet
- ENG8Q2L2 Opinion Marking SignalsDocument14 pagesENG8Q2L2 Opinion Marking SignalsJEROME SALAYNo ratings yet
- Piaget - Resources PDFDocument4 pagesPiaget - Resources PDFapi-533984280No ratings yet
- How To Make This More Objective, Impersonal Version? I Believe That..Document2 pagesHow To Make This More Objective, Impersonal Version? I Believe That..Anne Gleindez100% (1)
- Concept Paper Justine CerialesDocument6 pagesConcept Paper Justine CerialesJustine CerialesNo ratings yet
- Welfare Facilities and Employee Satisfaction in HLL PROJECT REPORT MBADocument91 pagesWelfare Facilities and Employee Satisfaction in HLL PROJECT REPORT MBABabasab Patil (Karrisatte)0% (1)
- The Walsh Family Resilience Questionnaire The Italian VersionDocument14 pagesThe Walsh Family Resilience Questionnaire The Italian VersionWinonaNo ratings yet
- Hilot, Yvonne Pajal - Chapter 1Document14 pagesHilot, Yvonne Pajal - Chapter 1EDUARDO lll NADATENo ratings yet
- Bustamante - NSTP100 Essay #11Document1 pageBustamante - NSTP100 Essay #11Jimin ParkNo ratings yet
- Host Organizations in Montreal: A List ofDocument48 pagesHost Organizations in Montreal: A List ofJashanbir SinghNo ratings yet
- Examining Ways That A Mindfulness-Based Intervention Reduces Stress in Public School TeachersDocument16 pagesExamining Ways That A Mindfulness-Based Intervention Reduces Stress in Public School TeachersAlícia NascimentoNo ratings yet
- Deep Water William Orville Douglas: Subjective ThemeDocument15 pagesDeep Water William Orville Douglas: Subjective ThemeArya kumar MallikNo ratings yet
- 2 NdtopicprDocument15 pages2 NdtopicprPerlita MorongNo ratings yet
- Celie Case StudyDocument8 pagesCelie Case Studyapi-491885108No ratings yet
- Preparation Checklist As Per ISO 45001 & 14001Document66 pagesPreparation Checklist As Per ISO 45001 & 14001vijayNo ratings yet
- Summary Report Prep.Document2 pagesSummary Report Prep.Babylyn RomeroNo ratings yet
- Aaa OB UC3M - Ch9 PDFDocument83 pagesAaa OB UC3M - Ch9 PDFIñigo López-ArandaNo ratings yet
- From Birth To Around 3 MonthsDocument2 pagesFrom Birth To Around 3 MonthsTESL10621 Shameen Farah Binti Mohd AminNo ratings yet
- Fact or Opinion HintsDocument2 pagesFact or Opinion HintsIan John MontalboNo ratings yet