You might also like
- GRADE 6 SCIENCE WORKBOOK - PDF Version 1Document164 pagesGRADE 6 SCIENCE WORKBOOK - PDF Version 1Amnah Hanma100% (6)
- 3600+ Review Questions For Anatomy & Physiology Volume 2 - (4th Edition) PDFDocument151 pages3600+ Review Questions For Anatomy & Physiology Volume 2 - (4th Edition) PDFMauzoom Ali100% (2)
- Pharmacology for Student and Pupil Nurses and Students in Associated ProfessionsFrom EverandPharmacology for Student and Pupil Nurses and Students in Associated ProfessionsNo ratings yet
- Neurogeni C Shock: By: Ervin VicenteDocument34 pagesNeurogeni C Shock: By: Ervin VicenteEjhay Vicente100% (2)
- Recent Advances in The Treatment of ShockDocument52 pagesRecent Advances in The Treatment of ShockasupicuNo ratings yet
- Acls Pre Course Self Assessment Study GuideDocument7 pagesAcls Pre Course Self Assessment Study Guidenova939100% (5)
- Working at Height Rescue PlanDocument1 pageWorking at Height Rescue PlanAbbas AsadNo ratings yet
- Shock in The Pediatric Patient: or Oxygen Don't Go Where The Blood Won't Flow!Document63 pagesShock in The Pediatric Patient: or Oxygen Don't Go Where The Blood Won't Flow!hana_shamsNo ratings yet
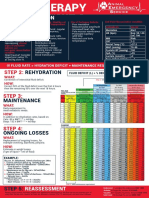
- FLUIDTHERAPY STEP 1: PERFUSIONDocument1 pageFLUIDTHERAPY STEP 1: PERFUSIONChristian De Leon100% (1)
- Shock and Its Management: Presented byDocument72 pagesShock and Its Management: Presented bysheme171150% (2)
- Vital SignsDocument94 pagesVital Signsglennm68100% (5)
- Brain Bee Quiz by Neil JainDocument1 pageBrain Bee Quiz by Neil Jainneiljainhd100% (2)
- Approach to Shock in 4 StagesDocument28 pagesApproach to Shock in 4 StagesSyasya ZulkiffliNo ratings yet
- ShockDocument49 pagesShockpaulyn ramos100% (1)
- ATLS Pre-Test (With Front Page)Document10 pagesATLS Pre-Test (With Front Page)Nourah A.Al Moqbel100% (2)
- NCP NeuroDocument20 pagesNCP NeuroNica Gaborne Navarro100% (3)
- Shock in Covid PatientDocument21 pagesShock in Covid PatientGHALEB A. AlmekhlafiNo ratings yet
- Circulation: Amal Alabbadi Sukainah Alalwi Fatimha Almarhoon Khadijah AlmubarakDocument33 pagesCirculation: Amal Alabbadi Sukainah Alalwi Fatimha Almarhoon Khadijah AlmubarakaliNo ratings yet
- Medical Surgical - Multiorgan Failure ReviewerDocument15 pagesMedical Surgical - Multiorgan Failure ReviewerNatricia TrondilloNo ratings yet
- Heart Failure 5ADocument86 pagesHeart Failure 5AK Praful KumarNo ratings yet
- Management of Shock in ChildrenDocument26 pagesManagement of Shock in ChildrenkarinakerenNo ratings yet
- Diagnosis&Manajemen ShockDocument8 pagesDiagnosis&Manajemen ShockHJKIMNo ratings yet
- Shock: Rose Ann J. Raquiza-Perante Post Graduate InternDocument53 pagesShock: Rose Ann J. Raquiza-Perante Post Graduate InternRose Ann RaquizaNo ratings yet
- Diagnosis Dan Penanganan Syok Hemorrhagi. (Manajemen Dan Terapi Cairan)Document31 pagesDiagnosis Dan Penanganan Syok Hemorrhagi. (Manajemen Dan Terapi Cairan)Idea HouseNo ratings yet
- Kuliah ShockDocument17 pagesKuliah Shockmuhammad hidayahNo ratings yet
- SYOKDocument76 pagesSYOKRiri EltadezaNo ratings yet
- Shock: Coass Anestesi Periode 12 Desember 2017 - 13 Januari 2018Document18 pagesShock: Coass Anestesi Periode 12 Desember 2017 - 13 Januari 2018iqbalNo ratings yet
- Handout 5 CardioVascular System Overview (Recovered)Document7 pagesHandout 5 CardioVascular System Overview (Recovered)Orlyn Joy TanaweNo ratings yet
- 11 - ShockDocument30 pages11 - ShockGalassa AbdiNo ratings yet
- Syock & ManagementDocument34 pagesSyock & ManagementIndra Anwari RukmanNo ratings yet
- Diagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaDocument51 pagesDiagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaHilmaNo ratings yet
- SHOCKDocument28 pagesSHOCKMohammad Azzlan Abd RahmanNo ratings yet
- 03 - Special Clinical SituationsDocument32 pages03 - Special Clinical SituationsClaudia KosztelnikNo ratings yet
- ShockDocument6 pagesShockShum Wing Hei JoanneNo ratings yet
- P 3a Gagal JTGDocument35 pagesP 3a Gagal JTGAnaMariyaMaNo ratings yet
- Heart Failure & Cardiac Arrest: Rony YuliwansyahDocument92 pagesHeart Failure & Cardiac Arrest: Rony YuliwansyahSasha ManoNo ratings yet
- SHOCK LEC Modified (2nd)Document86 pagesSHOCK LEC Modified (2nd)spanishthingz01No ratings yet
- Syok Kardiogenik Dr. Rani Maliawan, SP JPDocument59 pagesSyok Kardiogenik Dr. Rani Maliawan, SP JPLuh Leni AriniNo ratings yet
- 11 - Management Post Operative Low Cardiac Output SyndromeDocument46 pages11 - Management Post Operative Low Cardiac Output SyndromeNat SNo ratings yet
- Kuliah Bidan - Syok HipovolemikDocument28 pagesKuliah Bidan - Syok HipovolemikAsri PrameswariNo ratings yet
- DR Anuj Raj BijukchheDocument95 pagesDR Anuj Raj BijukchheMUHAMMAD JAWAD HASSANNo ratings yet
- Shock, Acid-Base Balance and Fluid Therapy: Shock Stages of ShockDocument4 pagesShock, Acid-Base Balance and Fluid Therapy: Shock Stages of ShockLonely WolfNo ratings yet
- NCP 3 - Deficient Fluid VolumeDocument4 pagesNCP 3 - Deficient Fluid VolumeKrishelle Kate PannigNo ratings yet
- Shock Said 20-21Document10 pagesShock Said 20-212859bathinaNo ratings yet
- Shock OverviewDocument6 pagesShock OverviewKrys Segarra GalarzaNo ratings yet
- Neonatal DocingDocument15 pagesNeonatal Docingchar21092000No ratings yet
- Fluid Dss PKB - RsDocument39 pagesFluid Dss PKB - RsancillaagraynNo ratings yet
- SHOCK LEC Modified (2nd)Document86 pagesSHOCK LEC Modified (2nd)spanishthingz01No ratings yet
- Lecture 12 Cardio Intensive CasesDocument32 pagesLecture 12 Cardio Intensive Casesraul0% (1)
- Integrated Diag and Treat of ShockkDocument79 pagesIntegrated Diag and Treat of ShockkDesy Randiahartika Sagita ZukhrinNo ratings yet
- ShockDocument70 pagesShockDawit g/kidanNo ratings yet
- Diagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaDocument49 pagesDiagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaSiti rahmawatiNo ratings yet
- DR - Nursamsu, SpPD-KGH-Penggunaan Cairan Koloid Pada Kondisi Syok PDFDocument38 pagesDR - Nursamsu, SpPD-KGH-Penggunaan Cairan Koloid Pada Kondisi Syok PDFNONANo ratings yet
- ShockDocument27 pagesShockyashmodi5555No ratings yet
- Sodium Imbalances (Hyponatremia Vs Hypernatremia)Document17 pagesSodium Imbalances (Hyponatremia Vs Hypernatremia)Angel FiloteoNo ratings yet
- Managing Hypovolemic ShockDocument12 pagesManaging Hypovolemic Shockرفاعي آكرمNo ratings yet
- null3Document24 pagesnull3Muneeb Ur RehmanNo ratings yet
- Shock: Definition, Pathophysiology, Features and Epidemiology of ShockDocument12 pagesShock: Definition, Pathophysiology, Features and Epidemiology of ShockMohamed omarNo ratings yet
- Resusitasi CairanDocument48 pagesResusitasi Cairanadi tiarmanNo ratings yet
- S1M3 Update Fluid Resuscitation Management in Emergency CasesDocument70 pagesS1M3 Update Fluid Resuscitation Management in Emergency Casesgriya medicaNo ratings yet
- Vas OpressorDocument41 pagesVas Opressorstevanus handrawanNo ratings yet
- ShockDocument86 pagesShockmeadwaiet1999No ratings yet
- Syok-Dr RaptoDocument64 pagesSyok-Dr RaptoMUHAMMAD HERNANDI YUSUFNo ratings yet
- Managing Hypovolemic ShockDocument12 pagesManaging Hypovolemic Shockرفاعي آكرمNo ratings yet
- Chronic Heart Failure: I. Brief Definition Iv. Disease ProcessDocument12 pagesChronic Heart Failure: I. Brief Definition Iv. Disease ProcessJennifer BeguinwaNo ratings yet
- Terapi Cairan PD Syok KardiogenikDocument27 pagesTerapi Cairan PD Syok KardiogenikSri AsmawatiNo ratings yet
- Shock BBDocument31 pagesShock BBVirang ParikhNo ratings yet
- Pediatric ResuscitationDocument55 pagesPediatric ResuscitationMargaretDeniseDelRosarioNo ratings yet
- Preoperative Cardiac Evaluation With Thoracic Echocardiography Before Non-Cardiac SurgeryDocument8 pagesPreoperative Cardiac Evaluation With Thoracic Echocardiography Before Non-Cardiac SurgeryMario AlexanderNo ratings yet
- Sedacion:Dolor:DelirioDocument49 pagesSedacion:Dolor:DelirioRamón Díaz-AlersiNo ratings yet
- What Is APRVDocument3 pagesWhat Is APRVMario AlexanderNo ratings yet
- Bumc0023 0313Document3 pagesBumc0023 0313Mario AlexanderNo ratings yet
- Intravenous Vs Intraosseous Adrenaline.76Document5 pagesIntravenous Vs Intraosseous Adrenaline.76Mario AlexanderNo ratings yet
- Ip Pals2020Document7 pagesIp Pals2020Mario AlexanderNo ratings yet
- 10 1016@j Bja 2020 10 040Document8 pages10 1016@j Bja 2020 10 040Mario AlexanderNo ratings yet
- Cerebral Abscess Hyponatremia DiagnosisDocument3 pagesCerebral Abscess Hyponatremia DiagnosisMario AlexanderNo ratings yet
- Evolving Consensus in Portal HypertensionDocument10 pagesEvolving Consensus in Portal HypertensionMario AlexanderNo ratings yet
- Development Disturbance of - Schizencephaly Type IIDocument9 pagesDevelopment Disturbance of - Schizencephaly Type IIneutronboyzNo ratings yet
- The Changing Role of Beta-Blocker Therapy in Patients With CirrhosisDocument11 pagesThe Changing Role of Beta-Blocker Therapy in Patients With CirrhosisMario AlexanderNo ratings yet
- Platelet Production and Destruction in Liver Cirrhosis: Background & AimsDocument7 pagesPlatelet Production and Destruction in Liver Cirrhosis: Background & AimsMario AlexanderNo ratings yet
- Jurnal 3Document8 pagesJurnal 3Bunga Maulani IskandarNo ratings yet
- E BM White PaperDocument14 pagesE BM White PaperpongidaeNo ratings yet
- Stem Cell TransplantDocument23 pagesStem Cell TransplantMario AlexanderNo ratings yet
- Effect SimvastatinDocument4 pagesEffect SimvastatinMario AlexanderNo ratings yet
- Cover Referat BPHDocument2 pagesCover Referat BPHMario AlexanderNo ratings yet
- Jurnal BMJDocument11 pagesJurnal BMJMario AlexanderNo ratings yet
- Translate Alva 2003Document8 pagesTranslate Alva 2003Mario AlexanderNo ratings yet
- Circulation WorksheetDocument3 pagesCirculation Worksheetholagato100% (1)
- NCP Deficient Fluid VolumeDocument5 pagesNCP Deficient Fluid VolumeCHRISTINE GRACE ELLONo ratings yet
- Acute Coronary Syndrome: Patsadee Nachom MDDocument58 pagesAcute Coronary Syndrome: Patsadee Nachom MDRachapon OngwibunwongNo ratings yet
- PHYSIO ReviewerDocument3 pagesPHYSIO ReviewerPHILYP EPHRAIM PARANGALANNo ratings yet
- BURN AnesthDocument58 pagesBURN AnesthKelvin TuazonNo ratings yet
- Research Article on Characteristics of Coronary Heart Disease Patients in North MalukuDocument10 pagesResearch Article on Characteristics of Coronary Heart Disease Patients in North MalukuAbduNo ratings yet
- Health Effects of Sleep DeprivationDocument7 pagesHealth Effects of Sleep DeprivationEmily KajlaNo ratings yet
- Ody Temperature As Evidenced by Temperature of 38.5Document1 pageOdy Temperature As Evidenced by Temperature of 38.5Jordz PlaciNo ratings yet
- Abg Interpretation 24738867503245712906Document2 pagesAbg Interpretation 24738867503245712906Joey CuayoNo ratings yet
- 200L FON PRESENTATION Group 1Document13 pages200L FON PRESENTATION Group 1jonaNo ratings yet
- NCM106 - Pharmacology Module 2.1 Nursing Process Focus: Care Patients Receiving Loop Diuretic: TorsemideDocument2 pagesNCM106 - Pharmacology Module 2.1 Nursing Process Focus: Care Patients Receiving Loop Diuretic: TorsemideBrandy RectoNo ratings yet
- Human Physiology From Cells To Systems 7th Edition Sherwood Test Bank Cells To Systems 7th Edition Sherwood Test BankDocument16 pagesHuman Physiology From Cells To Systems 7th Edition Sherwood Test Bank Cells To Systems 7th Edition Sherwood Test Bankteresamckenzieafvo100% (13)
- Revised Neurophysiology of Pain QuestionnaireDocument2 pagesRevised Neurophysiology of Pain QuestionnaireivanNo ratings yet
- Biology November Circulatory System Arav Nair 8A ROLL NO - 11Document35 pagesBiology November Circulatory System Arav Nair 8A ROLL NO - 11aravnair2302No ratings yet
- Autonomic Nervous System Anatomy and PhysiologyDocument50 pagesAutonomic Nervous System Anatomy and PhysiologyMAHARANINo ratings yet
- Sleep Deprivation and Mental HealthDocument4 pagesSleep Deprivation and Mental Healthapi-341198049No ratings yet
- كتاب التمريض الجديد2022Document206 pagesكتاب التمريض الجديد2022mohamed mohamedNo ratings yet
- Adrenal Gland Hormones and DisordersDocument2 pagesAdrenal Gland Hormones and DisordersSuneel Kumar PrajapatiNo ratings yet
- Cells Tissues Organs and Systems Power PointDocument11 pagesCells Tissues Organs and Systems Power PointNidonama E. KabmatNo ratings yet
- The 12 Steps of Muscle ContractionsDocument1 pageThe 12 Steps of Muscle ContractionsgraceNo ratings yet
- Drugs Affecting Respiratory SystemDocument19 pagesDrugs Affecting Respiratory SystemRuby Ann DimayugaNo ratings yet
- The Respiratory System 2019 dk-20191118110326Document26 pagesThe Respiratory System 2019 dk-20191118110326Jackson JastariNo ratings yet
- Lec Activity16-And-17 Digestive SystemDocument8 pagesLec Activity16-And-17 Digestive SystemYda Maxine PalmaNo ratings yet