You might also like
- Recent Advances in The Treatment of ShockDocument52 pagesRecent Advances in The Treatment of ShockasupicuNo ratings yet
- Syock & ManagementDocument34 pagesSyock & ManagementIndra Anwari RukmanNo ratings yet
- Pediatric Shock: Dr. Lilia Dewiyanti, Spa, MsimedDocument40 pagesPediatric Shock: Dr. Lilia Dewiyanti, Spa, MsimedLa Ode RinaldiNo ratings yet
- Golden Period Septic ChildDocument32 pagesGolden Period Septic ChildcallNo ratings yet
- Fluid Dss PKB - RsDocument39 pagesFluid Dss PKB - RsancillaagraynNo ratings yet
- ShockDocument27 pagesShockyashmodi5555No ratings yet
- Kuliah ShockDocument17 pagesKuliah Shockmuhammad hidayahNo ratings yet
- HYPO and HYPERNATREMIA IN NEONATESDocument10 pagesHYPO and HYPERNATREMIA IN NEONATESraghava mbbsNo ratings yet
- Post Operative Management After TAPVC RepairDocument36 pagesPost Operative Management After TAPVC RepairsreedeviNo ratings yet
- Scenario Title: Community Acquired Pneumonia Learning Outcomes: 1. Assessment and Recognition of The Signs and Symptoms of PneumoniaDocument6 pagesScenario Title: Community Acquired Pneumonia Learning Outcomes: 1. Assessment and Recognition of The Signs and Symptoms of PneumoniaDud AccNo ratings yet
- Management of Shock in ChildrenDocument26 pagesManagement of Shock in ChildrenkarinakerenNo ratings yet
- General Medical PrinciplesDocument5 pagesGeneral Medical PrinciplesNisha DNo ratings yet
- Diagnosis&Manajemen ShockDocument8 pagesDiagnosis&Manajemen ShockHJKIMNo ratings yet
- Paediatric Septic ShockDocument37 pagesPaediatric Septic ShockJavedgouri GouriNo ratings yet
- Resusitasi CairanDocument48 pagesResusitasi Cairanadi tiarmanNo ratings yet
- Pediatric Shock (PICUCOURSE)Document40 pagesPediatric Shock (PICUCOURSE)surasuarezlopezNo ratings yet
- Hypovolemic Shock: Dr. Sherwin BuluranDocument8 pagesHypovolemic Shock: Dr. Sherwin BuluranChristian UretaNo ratings yet
- Shock in Covid PatientDocument21 pagesShock in Covid PatientGHALEB A. AlmekhlafiNo ratings yet
- Alcohol Withdrawal Management: Recognition and Management of DTS, Seizures and Wernicke'S EncephalopathyDocument32 pagesAlcohol Withdrawal Management: Recognition and Management of DTS, Seizures and Wernicke'S EncephalopathySangkaran KumarNo ratings yet
- ShockDocument6 pagesShockShum Wing Hei JoanneNo ratings yet
- Paediatric Septic ShockDocument34 pagesPaediatric Septic ShockSudha YadavNo ratings yet
- Shock and Its Management: Presented byDocument72 pagesShock and Its Management: Presented bysheme171150% (2)
- Post Arrest CareDocument23 pagesPost Arrest CareMohamed RasoolNo ratings yet
- Uzma Mehdi, M.D, Ms NephrologyDocument46 pagesUzma Mehdi, M.D, Ms Nephrologykrish vjNo ratings yet
- Shock EditedDocument56 pagesShock EditedJeevan VelanNo ratings yet
- Transfusion-Associated Circulatory Overload (TACO)Document2 pagesTransfusion-Associated Circulatory Overload (TACO)belongs2diah3058100% (1)
- Acute Renal Failure Nursing Care PlanDocument4 pagesAcute Renal Failure Nursing Care PlanKrisianne Mae Lorenzo Francisco80% (5)
- Severe Sepsis&Septic Shock in Pediatrics.: Abdel Razzaq Abu Mayaleh, MDDocument27 pagesSevere Sepsis&Septic Shock in Pediatrics.: Abdel Razzaq Abu Mayaleh, MDlotskiNo ratings yet
- Aha Acls GuideDocument11 pagesAha Acls GuideIrene PimentelNo ratings yet
- SepsisDocument1 pageSepsisCharlie LeeNo ratings yet
- Ct7 Fluid, Electrolyte ImbalanceDocument9 pagesCt7 Fluid, Electrolyte ImbalanceAlondra VelascoNo ratings yet
- Shock States in ChildrenDocument37 pagesShock States in ChildrenjuanitaNo ratings yet
- ATOTW 136 Major Haemorrhage Part 1 2009Document6 pagesATOTW 136 Major Haemorrhage Part 1 2009viaereaNo ratings yet
- Shock PresentationDocument20 pagesShock PresentationvgmanjunathNo ratings yet
- Diagnosis Dan Penanganan Syok Hemorrhagi. (Manajemen Dan Terapi Cairan)Document31 pagesDiagnosis Dan Penanganan Syok Hemorrhagi. (Manajemen Dan Terapi Cairan)Idea HouseNo ratings yet
- Vasopressors and InotropesDocument31 pagesVasopressors and InotropesReza Prakosa SedyatamaNo ratings yet
- Fluid Resuscitation Algorithm For Adults With SepsisDocument1 pageFluid Resuscitation Algorithm For Adults With SepsisSorina BiliutaNo ratings yet
- 26) Approach To Pediatric ArrhythmiasDocument44 pages26) Approach To Pediatric ArrhythmiasJude AlyousefNo ratings yet
- Antihypertensive AgentsDocument97 pagesAntihypertensive AgentsL2 - MAKILALA, Zion joy B.No ratings yet
- 63 142 1 SMDocument5 pages63 142 1 SMAnnisa NoviliaNo ratings yet
- Poisoning Due To Abrus Precatorius (Jequirity Bean) : CasereportDocument3 pagesPoisoning Due To Abrus Precatorius (Jequirity Bean) : CasereportANDREA ESTEFANIA CUENCA CHIMBONo ratings yet
- Body Fluids and ElectrolytesDocument42 pagesBody Fluids and ElectrolytesQusaiBadr100% (1)
- Sinus Bradycardia: o No TX If AsymptomaticDocument3 pagesSinus Bradycardia: o No TX If Asymptomaticelle50% (2)
- Endpoints of Sepsis Resuscitation - FINALDocument63 pagesEndpoints of Sepsis Resuscitation - FINALMario AlexanderNo ratings yet
- 136 Management of Major Haemorrhage Part 1Document6 pages136 Management of Major Haemorrhage Part 1fitrah fajrianiNo ratings yet
- Disturbances in AcidDocument11 pagesDisturbances in AcidShannen Alija M. LaoNo ratings yet
- Clinical Paperwork 20 2Document3 pagesClinical Paperwork 20 2api-603548679No ratings yet
- Shock PresentationDocument20 pagesShock Presentationrosalyn sugayNo ratings yet
- I STAT Alinity V Utilization Guide ABX 00075R1Document8 pagesI STAT Alinity V Utilization Guide ABX 00075R1DrAlaa ZidanNo ratings yet
- Nursing Care Plan 6 Impaired Gas ExchangeDocument9 pagesNursing Care Plan 6 Impaired Gas Exchangedbryant0101100% (12)
- 2.3 Cập Nhật Chẩn Đoán Và Điều Trị Suy Tim-Phan Thái Hảo-14!11!2021 - .Pptx 4Document1 page2.3 Cập Nhật Chẩn Đoán Và Điều Trị Suy Tim-Phan Thái Hảo-14!11!2021 - .Pptx 4tranlekieutrinh166No ratings yet
- Disorders of Sodium: Presenter: DR Bharath Kumar P Moderator: DR Ramesh K NDocument41 pagesDisorders of Sodium: Presenter: DR Bharath Kumar P Moderator: DR Ramesh K NBharath Kumar PamulapatiNo ratings yet
- What Is Fluid Therapy?Document42 pagesWhat Is Fluid Therapy?Mirel YdianNo ratings yet
- General Measure in The Management of PoisoningDocument43 pagesGeneral Measure in The Management of PoisoningCharlotte Anne Villero TiuNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityAlexis HospitalNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityChris LeeNo ratings yet
- (Local Anaesthetics) : Dr. MizajDocument17 pages(Local Anaesthetics) : Dr. MizajaliNo ratings yet
- Approach To ShockDocument40 pagesApproach To ShockDivesh NaiduNo ratings yet
- SYOK - Desi Surya IniDocument40 pagesSYOK - Desi Surya IniDesi Suryani DewiNo ratings yet
- Neonatal Air Leak Syndrome and The Role Of.3Document9 pagesNeonatal Air Leak Syndrome and The Role Of.3Claudia KosztelnikNo ratings yet
- Neonatal Hyperglycemia, Which Threshold Value, Diagnostic Approach and Treatment?: Turkish Neonatal and Pediatric Endocrinology and Diabetes Societies Consensus ReportDocument5 pagesNeonatal Hyperglycemia, Which Threshold Value, Diagnostic Approach and Treatment?: Turkish Neonatal and Pediatric Endocrinology and Diabetes Societies Consensus ReportClaudia KosztelnikNo ratings yet
- Article - A Case of Conservatively Managed Pneumopericardium in A NeonateDocument1 pageArticle - A Case of Conservatively Managed Pneumopericardium in A NeonateClaudia KosztelnikNo ratings yet
- Mechanical Ventilation Guidelines SNSDocument8 pagesMechanical Ventilation Guidelines SNSClaudia KosztelnikNo ratings yet
- Imaging Findings in Cardiac Tamponade With EmphasiDocument18 pagesImaging Findings in Cardiac Tamponade With EmphasiClaudia KosztelnikNo ratings yet
- Lung Ultrasound For Neonatal Cardio-Respiratory Conditions: Daniele de Luca (MD, PHD)Document52 pagesLung Ultrasound For Neonatal Cardio-Respiratory Conditions: Daniele de Luca (MD, PHD)Claudia Kosztelnik100% (1)
- Neonatal Hyperglycemia, Which Threshold Value, Diagnostic Approach and Treatment?: Turkish Neonatal and Pediatric Endocrinology and Diabetes Societies Consensus ReportDocument5 pagesNeonatal Hyperglycemia, Which Threshold Value, Diagnostic Approach and Treatment?: Turkish Neonatal and Pediatric Endocrinology and Diabetes Societies Consensus ReportClaudia KosztelnikNo ratings yet
- User Guide: IBM Micromedex® Neofax® and PediatricsDocument57 pagesUser Guide: IBM Micromedex® Neofax® and PediatricsClaudia KosztelnikNo ratings yet
- 01 - Early Diagnosis of Congenital Cardiac DefectsDocument40 pages01 - Early Diagnosis of Congenital Cardiac DefectsClaudia KosztelnikNo ratings yet
- Lung Ultrasound For Neonatal Cardio-Respiratory Conditions: Daniele de Luca (MD, PHD)Document52 pagesLung Ultrasound For Neonatal Cardio-Respiratory Conditions: Daniele de Luca (MD, PHD)Claudia Kosztelnik100% (1)
- Echo#Document18 pagesEcho#talktoibbuNo ratings yet
- 01 - Early Diagnosis of Congenital Cardiac DefectsDocument40 pages01 - Early Diagnosis of Congenital Cardiac DefectsClaudia KosztelnikNo ratings yet
- User Guide: IBM Micromedex® Neofax® and PediatricsDocument57 pagesUser Guide: IBM Micromedex® Neofax® and PediatricsClaudia KosztelnikNo ratings yet
- User Guide: IBM Micromedex® Neofax® and PediatricsDocument57 pagesUser Guide: IBM Micromedex® Neofax® and PediatricsClaudia KosztelnikNo ratings yet
- 406ronmfrt0n7269301 PDFDocument5 pages406ronmfrt0n7269301 PDFClaudia KosztelnikNo ratings yet
- Calcule Metal 2Document18 pagesCalcule Metal 2Claudia KosztelnikNo ratings yet
- LAPTARE Copii Cu Patologie...Document8 pagesLAPTARE Copii Cu Patologie...Claudia KosztelnikNo ratings yet
- Tabel Student IDocument1 pageTabel Student IClaudia KosztelnikNo ratings yet
- 01 - Approach To The Post Operative Patient PDFDocument42 pages01 - Approach To The Post Operative Patient PDFClaudia KosztelnikNo ratings yet
- Plansa 1-A2Document1 pagePlansa 1-A2Claudia KosztelnikNo ratings yet
- Guidelines For The Interpretation of The Neonatal ElectrocardiogramDocument16 pagesGuidelines For The Interpretation of The Neonatal ElectrocardiogramccNo ratings yet
- Evolution of NeonatologyDocument17 pagesEvolution of NeonatologyClaudia KosztelnikNo ratings yet
- Allo ImmunizationDocument7 pagesAllo ImmunizationClaudia KosztelnikNo ratings yet
- Evolution of NeonatologyDocument17 pagesEvolution of NeonatologyClaudia KosztelnikNo ratings yet
- Has Anti DDocument4 pagesHas Anti DClaudia KosztelnikNo ratings yet
- High DoseDocument6 pagesHigh DoseClaudia KosztelnikNo ratings yet
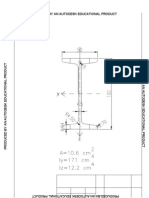
- Produced by An Autodesk Educational ProductDocument1 pageProduced by An Autodesk Educational ProductClaudia KosztelnikNo ratings yet
- Information MSQ KROK 2 Medicine 2007 2020 ANESTHESIOLOGYEMERGENCYDocument73 pagesInformation MSQ KROK 2 Medicine 2007 2020 ANESTHESIOLOGYEMERGENCYHikufe JesayaNo ratings yet
- MPMSU MBBS 1st Year Previous Year Questions (2015-2023)Document83 pagesMPMSU MBBS 1st Year Previous Year Questions (2015-2023)Koshtubh Pratap Singh PariharNo ratings yet
- Referat LP8-2E - CholesterolDocument3 pagesReferat LP8-2E - CholesterolElena DalcaranNo ratings yet
- Top 10 Takeaways Clinicians - UpdatedDocument1 pageTop 10 Takeaways Clinicians - UpdatedBea Barbara CarrascalNo ratings yet
- Chest X-RayDocument101 pagesChest X-RayRizka RamadaniNo ratings yet
- 11 Anti-Coagulants & FibrinolyticsDocument52 pages11 Anti-Coagulants & FibrinolyticsUmmuShefaNo ratings yet
- Kanski'S: Clinical OphthalmologyDocument504 pagesKanski'S: Clinical OphthalmologyMohin hossain100% (1)
- DyspneuDocument9 pagesDyspneuAmy KochNo ratings yet
- Cardiogenic ShockDocument8 pagesCardiogenic ShockMAE RACHELLE LAMOSTENo ratings yet
- 058+ +1595+ +Luh+Made+Indrasuari+ +galleyDocument5 pages058+ +1595+ +Luh+Made+Indrasuari+ +galleyLathief CaakNo ratings yet
- Lesson Plan On EcgDocument3 pagesLesson Plan On Ecganimesh panda100% (1)
- Cardiogenic ShockDocument49 pagesCardiogenic Shockmaibejose0% (1)
- AclsDocument4 pagesAclsAnusha Verghese100% (1)
- TMS ChecklistDocument1 pageTMS ChecklistMuhammad HussnainNo ratings yet
- ITLC Questions 2019Document9 pagesITLC Questions 2019Neil ThomasNo ratings yet
- Citicoline Drug StudyDocument2 pagesCiticoline Drug StudyJC LumayaNo ratings yet
- CSMLS Exam Guide Notes (Referrence Range)Document4 pagesCSMLS Exam Guide Notes (Referrence Range)software4us.2023No ratings yet
- Pulmonary Vasodilator Strategies in Neonates With Acute Hypoxemic Respiratory Failure and Pulmonary HypertensionDocument8 pagesPulmonary Vasodilator Strategies in Neonates With Acute Hypoxemic Respiratory Failure and Pulmonary HypertensionAndres MahechaNo ratings yet
- Critical Care NotesDocument18 pagesCritical Care NotesjulieNo ratings yet
- Pathophysiology of HCVDDocument5 pagesPathophysiology of HCVDNicolne Lorraine100% (1)
- Necrosis and Types of NecrosisDocument2 pagesNecrosis and Types of NecrosisHisham NesemNo ratings yet
- E.C.G Machine: by Er.U.Karthik Premkumar, H.O.D - Biomedical Engineering DepartmentDocument36 pagesE.C.G Machine: by Er.U.Karthik Premkumar, H.O.D - Biomedical Engineering DepartmentAch ThungNo ratings yet
- Thesis On Coronary Artery DiseaseDocument7 pagesThesis On Coronary Artery Diseasesherielliottbillings100% (1)
- Pediatric Nursing: A. Sigmund Freud: Psychosexual TheoryDocument12 pagesPediatric Nursing: A. Sigmund Freud: Psychosexual TheoryMicah MagallanoNo ratings yet
- Endocardul PatologieDocument31 pagesEndocardul PatologieAlexe VladNo ratings yet
- Portal HypertensionDocument4 pagesPortal HypertensiondrstalamNo ratings yet
- Drug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesDocument2 pagesDrug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesSheryhan Tahir BayleNo ratings yet
- Unknown 5Document35 pagesUnknown 5Rayane NaegelsNo ratings yet
- Anatomy and Physiology of The Biliary SystemDocument5 pagesAnatomy and Physiology of The Biliary SystemstephenlopezNo ratings yet
- CH 13 ActivityDocument4 pagesCH 13 Activityash vldnbrNo ratings yet