You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- User Guide: IBM Micromedex® Neofax® and PediatricsDocument57 pagesUser Guide: IBM Micromedex® Neofax® and PediatricsClaudia KosztelnikNo ratings yet
- User Guide: IBM Micromedex® Neofax® and PediatricsDocument57 pagesUser Guide: IBM Micromedex® Neofax® and PediatricsClaudia KosztelnikNo ratings yet
- User Guide: IBM Micromedex® Neofax® and PediatricsDocument57 pagesUser Guide: IBM Micromedex® Neofax® and PediatricsClaudia KosztelnikNo ratings yet
- ERN MRCPCH 3e PDFDocument52 pagesERN MRCPCH 3e PDFrizixxxxxx80% (5)
- Diagnosis and Treatment of Pulmonary Arterial Hypertension A ReviewDocument13 pagesDiagnosis and Treatment of Pulmonary Arterial Hypertension A ReviewLuis Enrique Giraldo PenicheNo ratings yet
- Neonatal Air Leak Syndrome and The Role Of.3Document9 pagesNeonatal Air Leak Syndrome and The Role Of.3Claudia KosztelnikNo ratings yet
- Neonatal Hyperglycemia, Which Threshold Value, Diagnostic Approach and Treatment?: Turkish Neonatal and Pediatric Endocrinology and Diabetes Societies Consensus ReportDocument5 pagesNeonatal Hyperglycemia, Which Threshold Value, Diagnostic Approach and Treatment?: Turkish Neonatal and Pediatric Endocrinology and Diabetes Societies Consensus ReportClaudia KosztelnikNo ratings yet
- Article - A Case of Conservatively Managed Pneumopericardium in A NeonateDocument1 pageArticle - A Case of Conservatively Managed Pneumopericardium in A NeonateClaudia KosztelnikNo ratings yet
- Mechanical Ventilation Guidelines SNSDocument8 pagesMechanical Ventilation Guidelines SNSClaudia KosztelnikNo ratings yet
- Imaging Findings in Cardiac Tamponade With EmphasiDocument18 pagesImaging Findings in Cardiac Tamponade With EmphasiClaudia KosztelnikNo ratings yet
- Lung Ultrasound For Neonatal Cardio-Respiratory Conditions: Daniele de Luca (MD, PHD)Document52 pagesLung Ultrasound For Neonatal Cardio-Respiratory Conditions: Daniele de Luca (MD, PHD)Claudia Kosztelnik100% (1)
- 03 - Special Clinical SituationsDocument32 pages03 - Special Clinical SituationsClaudia KosztelnikNo ratings yet
- Echo#Document18 pagesEcho#talktoibbuNo ratings yet
- Neonatal Hyperglycemia, Which Threshold Value, Diagnostic Approach and Treatment?: Turkish Neonatal and Pediatric Endocrinology and Diabetes Societies Consensus ReportDocument5 pagesNeonatal Hyperglycemia, Which Threshold Value, Diagnostic Approach and Treatment?: Turkish Neonatal and Pediatric Endocrinology and Diabetes Societies Consensus ReportClaudia KosztelnikNo ratings yet
- 01 - Early Diagnosis of Congenital Cardiac DefectsDocument40 pages01 - Early Diagnosis of Congenital Cardiac DefectsClaudia KosztelnikNo ratings yet
- Lung Ultrasound For Neonatal Cardio-Respiratory Conditions: Daniele de Luca (MD, PHD)Document52 pagesLung Ultrasound For Neonatal Cardio-Respiratory Conditions: Daniele de Luca (MD, PHD)Claudia Kosztelnik100% (1)
- 406ronmfrt0n7269301 PDFDocument5 pages406ronmfrt0n7269301 PDFClaudia KosztelnikNo ratings yet
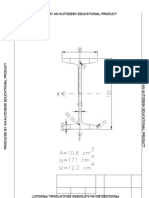
- Calcule Metal 2Document18 pagesCalcule Metal 2Claudia KosztelnikNo ratings yet
- LAPTARE Copii Cu Patologie...Document8 pagesLAPTARE Copii Cu Patologie...Claudia KosztelnikNo ratings yet
- Tabel Student IDocument1 pageTabel Student IClaudia KosztelnikNo ratings yet
- 01 - Approach To The Post Operative Patient PDFDocument42 pages01 - Approach To The Post Operative Patient PDFClaudia KosztelnikNo ratings yet
- Plansa 1-A2Document1 pagePlansa 1-A2Claudia KosztelnikNo ratings yet
- Guidelines For The Interpretation of The Neonatal ElectrocardiogramDocument16 pagesGuidelines For The Interpretation of The Neonatal ElectrocardiogramccNo ratings yet
- Evolution of NeonatologyDocument17 pagesEvolution of NeonatologyClaudia KosztelnikNo ratings yet
- Allo ImmunizationDocument7 pagesAllo ImmunizationClaudia KosztelnikNo ratings yet
- Evolution of NeonatologyDocument17 pagesEvolution of NeonatologyClaudia KosztelnikNo ratings yet
- Has Anti DDocument4 pagesHas Anti DClaudia KosztelnikNo ratings yet
- High DoseDocument6 pagesHigh DoseClaudia KosztelnikNo ratings yet
- Produced by An Autodesk Educational ProductDocument1 pageProduced by An Autodesk Educational ProductClaudia KosztelnikNo ratings yet
- Penyakit Jantung KongenitalDocument30 pagesPenyakit Jantung KongenitalrintiikNo ratings yet
- Saudi License Exam (SLE) 3rd Edt. UQUDocument445 pagesSaudi License Exam (SLE) 3rd Edt. UQUkingmedic98% (41)
- Peds MCQDocument395 pagesPeds MCQSmart NemoNo ratings yet
- Program Book of INAechoDocument15 pagesProgram Book of INAechoAnthomina MayaNo ratings yet
- ECG Symcard 2016 - Electrocardiography On Congenital Heart Disease PDFDocument53 pagesECG Symcard 2016 - Electrocardiography On Congenital Heart Disease PDFCia100% (1)
- Cardio Vascular DisordersDocument62 pagesCardio Vascular DisordersUday Kumar100% (1)
- 14.1 The Hole Inside The Heart ABSTRAKDocument11 pages14.1 The Hole Inside The Heart ABSTRAKYudhistira AdiNo ratings yet
- Pulmonary Atresia With Intact Ventricular Septum: PA/IVSDocument36 pagesPulmonary Atresia With Intact Ventricular Septum: PA/IVSRedmond P. Burke MD100% (1)
- Neonatal PhysiologyDocument65 pagesNeonatal Physiologyunknownsince1986No ratings yet
- Complete Medical TermsDocument32 pagesComplete Medical TermsSharifa Darayan100% (1)
- Lung TransplantationDocument16 pagesLung Transplantationlparen4144No ratings yet
- Physiologic Transition From Intrauterine To Extrauterine LifeDocument6 pagesPhysiologic Transition From Intrauterine To Extrauterine LifeGina M. TañedoNo ratings yet
- Cardiovascular Physiology - Cardiac Cycle and MurmursDocument107 pagesCardiovascular Physiology - Cardiac Cycle and MurmursAaron D. Phoenix100% (1)
- Normal PediaDocument13 pagesNormal PediaChelsea GulfanNo ratings yet
- CV Fellowship Brochure 2013Document15 pagesCV Fellowship Brochure 2013Anonymous Ou02SWgGZNo ratings yet
- Guidelines GUCH FTDocument43 pagesGuidelines GUCH FTmiky1320No ratings yet
- Right + Increased Vascularity + Fixed S2 / Widely Split Austin-Flint (Chronic) Graham Steele MurmurDocument14 pagesRight + Increased Vascularity + Fixed S2 / Widely Split Austin-Flint (Chronic) Graham Steele MurmurRojales FrancisNo ratings yet
- Jugular Venous Pulse: Madras Medical MissionDocument53 pagesJugular Venous Pulse: Madras Medical MissionJoshua JayakaranNo ratings yet
- COMPLETE Medical Disease in PregnancyDocument210 pagesCOMPLETE Medical Disease in PregnancyCHANDREN ARUMUGAMNo ratings yet
- The Pediatric ECGDocument14 pagesThe Pediatric ECGPat Oo KobNo ratings yet
- Congenital Heart Disease Series 1Document9 pagesCongenital Heart Disease Series 1api-216828341No ratings yet
- Medical AbbreviationsDocument18 pagesMedical AbbreviationsFilbertaNo ratings yet
- Congenital Heart DefectsDocument16 pagesCongenital Heart DefectsLara TomašićNo ratings yet
- Atrial Septal DefectDocument2 pagesAtrial Septal DefecttaheNo ratings yet
- Model Test PapersDocument2 pagesModel Test Papersprofarmah6150No ratings yet
- ? - Pedia MidtermsDocument18 pages? - Pedia Midtermsysabel.mendozaNo ratings yet
- LP1ncm109 YboaDocument21 pagesLP1ncm109 YboaMargarette GeresNo ratings yet
- Soal 5Document31 pagesSoal 5Agustinus FatollaNo ratings yet